
Abstract
Introduction
Flatfoot and patellar instability are both developmental limb deformities that occur frequently in adolescents. A high number of patients with both diseases can be seen in clinic, and there are no studies showing a correlation between the two. The goal of this study is to investigate the association between developmental patellar instability and flat feet in adolescents and its associated risk factors.
Methods
This experiment uses a cross-sectional study to select 74 adolescent patients with flat foot from a randomly selected middle school in this city since December 2021 and obtain relevant data. SPSS26.0 statistical software was used for data analysis. Quantitative data were expressed as mean ± standard deviation, and Pearson correlation coefficient was used for analysis. p < 0.05 indicates a statistically significant difference.
Results
A total of 74 people (40 men and 34 women) were included in this study. The correlation coefficients between Meary angle, Pitch angle, calcaneal valgus angle, CSI, BMI, and Beighton scores and knee joint Q angle are 0.358 (p < 0.01), −0.312 (p < 0.01), 0.403 (p < 0.01), 0.596 (p < 0.01), 0.427 (p < 0.01), and 0.293 (p < 0.05), respectively, indicating that flat foot, overweight, and Beighton scores are all correlated with Q angle. The correlation coefficients between Meary angle, Pitch angle, calcaneal valgus angle, CSI, and BMI were 0.431 (p < 0.01), −0.399 (p < 0.01), 0.319 (p < 0.01), and 0.563 (p < 0.01), respectively, indicating a correlation between flat foot and BMI. The correlation coefficients between Meary’s angle, Pitch’s angle, calcaneal valgus angle, CSI, and Beighton’s score were 0.207 (p > 0.05), −0.240 (p < 0.05), 0.204 (p > 0.05), and 0.413 (p < 0.01), respectively, indicating a correlation between flat foot and Beighton’s score.
Conclusion
We believe that there is a significant correlation between adolescent flatfoot and patellar instability. Excessive weight and ligamental laxity during adolescent development are among the risk factors for flatfoot and patellar instability.
Flatfoot is a foot deformity caused by various reasons, usually manifested as the collapse or even disappearance of the medial longitudinal or transverse arch of the foot. Most patients are accompanied by anterior foot abduction and calcaneal valgus.1,2Adolescent flat foot are mostly flexible and flat foot, with arches that are not fully formed during development and relatively high joint activity. Most adolescent flat foot will return to normal as they age, and some patients will develop into adult flat foot.3,4 Flat foot, due to the low and flat arch of the foot, result in the destruction of the stable structure of the foot, further causing uneven stress between the bones of the foot. With prolonged walking and movement, it causes organic changes in the body structure, resulting in foot pain, ankle arthritis, hip and knee joint injury, and waist pain. 5
Patellar instability is a common disease of the knee joint, usually manifested as knee pain, with a prevalence rate of up to 25%. It is commonly seen in young people. Patients with patellar instability are at risk of patellar dislocation during exercise. 6 Patellar dislocation accounts for 3.3% of all knee joint injuries, with an overall recurrence rate of approximately 30% after the first patellar dislocation. 7 Patellar instability is mainly caused by structural abnormalities of the knee joint, such as dysplasia of the femoral trochlear groove, high patella, looseness of the medial patellar retinaculum, enlargement of the knee joint Q angle, and tibial rotation.6,8 Patellar instability is also recognized as one of the important pathogenic factors leading to patellofemoral arthritis and chondromalacia of the patella in the later stage.9,10
With the development of medical technology, people’s understanding of the human body structure has deepened, and it has gradually been proposed that there is also a certain relationship between independent diseases. Especially when it comes to changes in the stable shape of a certain structure in the lower limb as a whole, it will have a certain impact on the entire lower limb force line, leading to secondary diseases.11–13
Our research group has found clinically that some patients who come to our hospital with flat foot as a diagnosis have patellar instability, while most patients who come to our hospital with patellar dislocation have flat foot. Based on this issue, this study explored the correlation and risk factors between adolescent flat foot and developmental patellar instability.
Materials and methods
A cross-sectional study was selected for investigation. Our team conducted a flat foot screening for seventh grade students at a random middle school in Urumqi, China. Two foot and ankle specialists with years of experience observed the height of the foot arch for initial screening, and then conducted foot print testing. Patients diagnosed as flat foot based on the degree of foot print collapse were considered suitable candidates for this study. The researchers re screened the selected population based on the inclusion and exclusion criteria to select patients for inclusion in the study. Inclusion criteria; (1) Age: no more than 14 years old, no less than 12 years old, (2) no other soft tissue, joint, or bone lesions except for the affected limb, (3) diagnosed as flat foot (with or without foot pain); Exclusion criteria: (1) Previous history of foot trauma (tendon injury, fracture, etc.); (2) Patients who cannot walk on their own; (3) Patients with other neurological diseases; (4) Stiff flat foot. All participants have signed an informed consent form, and the medical institution where our team works has reviewed and approved this study.
Demographic data.

A total of 74 patients underwent the investigation.
° plus one point (both sides), ② shoulder joint is raised 90°, forearm is extended and wrist joint is flexed, The thumb can reach the forearm plus one point (both sides) ③ Excessive back extension of the elbow 10° plus one point (both sides) ④ Excessive back extension of the knee 10° plus one point (both sides) ⑤ When bending the hips and extending the knees, place both palms flat on the floor plus one point.
Clinical index measurement: The X-ray film was taken in the Sixth Affiliated Hospital of Xinjiang Medical University, and the relevant angles were measured on the X-ray film. Meary angle: The included angle formed by the intersection of the long axis of the talus and the first metatarsal bone. Pitch angle: The angle between a line parallel to the ground and a line along the downhill axis of the calcaneus. Calcaneal valgus angle: The included angle formed between the line connecting the long axis of the tibia and the long axis of the calcaneus in the Saltzman position. The Chippaux-Smirak Index of foot prints is measured using a foot print foot pressure detection board produced by the Meishuer Foot and Ankle Orthopedics Store. The value obtained by measuring the width of the middle foot of the foot print compared to the width of the metatarsal bone is the Chippaux-Smirak Index. BMI obtains the height and weight through physical examination of the patient, and calculates the height ÷ weight 2 The resulting value is BMI. Knee joint Q angle: (The angle from the midpoint of the patella to the tibial tubercle that intersects the traction line of the quadriceps femoris is called the Q angle) When the patient stands in a neutral position, mark the positions of the anterior superior iliac spine, the midpoint of the patella, and the tibial tubercle, and then measure the Q angle. The Beighton score is evaluated by researchers on a one-on-one physical examination of patients.
We evaluated the correlation between Meary angle, Pitch angle, calcaneal valgus angle, CSI, BMI, and Beighton scores and knee joint Q angle, as well as the correlation between lateral talus first metatarsal angle, lateral calcaneal inclination angle, calcaneal valgus angle, and foot print Chippaux Smirak Index and BMI, Beighton scores. Statistical analysis of the data was conducted using SPSS26.0, and Pearson correlation coefficient was used for testing. p < 0.05 was considered statistically significant.
Results
Clinical and examination outcomes (N = 74).

Abbreviations: Chippaux Smirak Index (CSI); Body Mass Index(BMI).
Correlation analysis between measured data and knee joint Q angle.

P<0.05 means that the result is statistically significant.
Abbreviations: Chippaux Smirak Index (CSI); Body Mass Index(BMI).

(a) Calcaneal valgus angle, (b) Knee joint Q angle, (c) Examiner’s foot print.

A linear scatter plot showing the correlation between all measured data and the Q angle.
Correlation analysis between foot measurement data and BMI.
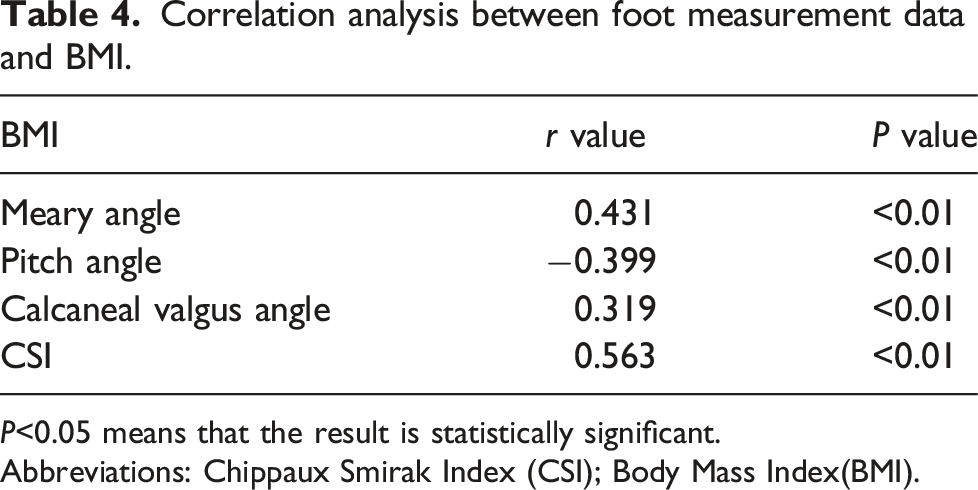
P<0.05 means that the result is statistically significant.
Abbreviations: Chippaux Smirak Index (CSI); Body Mass Index(BMI).
Correlation analysis between foot measurement data and Beighton scores.

P<0.05 means that the result is statistically significant.
Abbreviations: Chippaux Smirak Index(CSI); Body Mass Index(BMI).
This study uses Pearson correlation coefficient to statistically analyze the data, and the results show that there is a significant correlation between flat foot and patellar instability. Patients with heavier flat foot have a larger knee joint Q angle, which can increase the risk of patellar instability in patients. Moreover, overweight and excessive ligamental laxity may be risk factors for flat foot and patellar instability.
Discussion
Newborn infants have loose physiological ligaments in their foot, resulting in lower and flat arches, which are similar to flat foot in appearance. However, as the child gradually grows and develops and walks with weight on their foot, plantar fat decreases, and the longitudinal and transverse arches of the foot begin to develop significantly.14,15Acquired flat foot is mainly affected by external factors such as physical activity levels, footwear habits, and living areas. Preschool age is the main stage of arch development, and most children’s arch growth is fixed and shaped at the age of 8–12 years. 16 It is reported that flat foot before the age of 10 is physiological, and children with flat foot at this time usually have no functional limitations or clinical symptoms of the foot, and the collapsed arch of the foot will gradually recover with age. 14 The prevalence of flat foot in children shows a significant downward trend from the appearance of the arch of the foot to the rapid development of the arch of the foot. The younger the age, the greater the probability of flat foot appearing. 17 Some scholars have reported that the detection rate of flat foot in boys is higher than that in girls, which is the same as the proportion of the population included in this study, but contrary to the results of adult studies.18,19 This may be due to the early puberty of girls, the maturation of the arch of the foot earlier than boys, and the thicker plantar fat pads of boys than girls. Laxity of joint ligaments is also a factor in the occurrence of flat foot in children and adolescents, and exceeding the standard range of joint activity is considered to be one of the inducing factors for flexible flat foot in children. 20 This is consistent with the results in this study. There is a moderate correlation between the ligamental laxity score and the CSI of the foot print, while there is a slight correlation between the CSI and the Pitch angle. Excessive ligamental laxity may lead to collapse of the foot arch. Children will experience a period of joint ligament development, during which joint ligamental laxity may be caused by underdevelopment. It is a process of self construction and self organization within the human body and a manifestation of the gradual maturation of the human body. Generally speaking, joint ligamental laxity gradually improves with age, and most cases are caused by normal physiological phenomena. Overweight is also a high risk factor for flatfoot. The incidence rate of flatfoot in high weight children is more than twice that of normal weight children. High weight children have relatively little exercise. Over time, the incidence rate of flatfoot has increased. 21 However, flat feet may also cause an increase in body weight. When patients with flat feet experience foot fatigue or pain, patients reduce their activity to avoid limb discomfort, and as time passes, the lack of exercise leads to a slow increase in body weight. The correlation between BMI and foot-related data and the footprint C-S index in this study suggests that there is a correlation between overweight and flat feet, but a causal relationship between the two cannot be proven.
The stability of the patella is also affected by the height of the patella and the alignment of the lower limbs. High patella leads to the inability of the patella to smoothly enter the femoral trochlear, resulting in poor matching of the motion trajectory during flexion and extension of the knee joint, which is prone to dislocation; Uneven alignment of the lower limbs, such as increased femoral anteversion angle, knee valgus, and tibial rotation, all increase the risk of patellar dislocation[7]. The results of this study suggest that excessive weight and excessive ligamental laxity may be risk factors for patellar instability, increasing the risk of patellar dislocation during exercise.
With the development of science and technology, people’s understanding of the human body structure has gradually deepened, and some scholars have gradually proposed that there is also a certain relationship between independent diseases, especially when the stable shape of a structure in the lower limb as a whole is changed, which will have a certain impact on the entire lower limb force line, leading to secondary diseases. Due to the collapse of the arch of the foot, the calcaneus valgus, and the uneven distribution of plantar pressure in flat foot, after a large amount of weight bearing exercise, the damage to the anatomical relationship of the foot is aggravated. The calcaneus valgus is obvious, the foot bone hyperplasia, plantar fasciitis, etc., and the foot presents discomfort and pain, which further affects the patient’s standing, walking posture, and lower limb force line changes. 22 Nguyen A D 23 has reported studying the relationship between lower limb alignment feature selection and Q angle in the pelvis, hip, knee, and foot, and finally concluded that Q angle poses a certain risk to the entire lower limb.Min Z 12 conducted a correlation analysis between the severity of flat foot and knee osteoarthritis after grouping, and the results showed that the severity of flat foot was significantly related to the symptoms of knee osteoarthritis. They believed that patients with flat foot and their severity should be considered when treating knee osteoarthritis.The balance movement ability of patients with flat foot can change due to changes in the foot structure. Excessive valgus of the hind foot can lead to reduced posture stability during movement. The pronation of the front foot of flat foot not only affects the biomechanics of the foot, but also affects the lower limb motion chain during the entire gait period, such as peak pronation of the knee joint and range of motion of the pelvis. These changes in foot kinematics can increase the risk of musculoskeletal disease, A systematic review describes flat foot and high arch foot as associated with lower limb injuries compared to common foot types.24,25
Olerud C 26 reported that when the foot is in different positions of internal, external, pronation, and supination, the corresponding knee joint and even the hip joint are affected to some extent, and the knee joint Q angle changes with the position of the foot.Saxena A 27 treated 102 patients with patellofemoral chondromalacia and patella pain syndrome with a semi flexible plantar orthosis, and the results showed that 76.5% of the patients had improved pain. It was concluded that the use of semi flexible orthosis shoes was significant in alleviating the symptoms of patellofemoral chondromalacia and patella pain syndrome. For patients with flat foot with knee joint lesions, the pain symptoms of the knee joint can be significantly improved after treatment for flat foot, giving us reason to believe that there is a certain correlation between flat foot and knee joint lesions. Han Y 28 collected 72 young patients with flat foot, measured and analyzed relevant indicators, and concluded that there was a correlation between flat foot and patellar subluxation. However, the majority of the population included in this study were adults, and all had symptoms of foot pain. Considering that patients with developmental patellar instability often occur in adolescents, and that the initial formation of the human foot arch is approximately after the age of 10 years, this study selected adolescents in their developmental stages as the research target for more comprehensive clinical data acquisition.
There are some limitations in this study: ① This study is a cross-sectional study, and patients in the latent or remission stages are prone to misdiagnosis and bias. ② The number of patients included in the study is small, which has a certain impact on the accuracy of the results The selected patients are still in the development process, so the selected age group is relatively narrow and lacks coverage. ④ There are many clinical indicators of developmental patellar instability, but only using the Q angle as an evaluation indicator has certain limitations.
Conclusion
The results of this study indicate that there is a high correlation between flatfoot and patellar instability, and overweight and excessive ligamental laxity are both risk factors for flatfoot and patellar instability. These results indicate that the development of the knee joint in adolescents is also affected by the height of the arch of the foot, and we need to strengthen our understanding of flat foot. Therefore, we recommend taking flat foot as a routine physical examination item during adolescent development, and formulating an effective plan for early intervention and treatment of flat foot.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81860164).