
Abstract
Aims
Our objective is to compare the functional results in patients that underwent surgery for recurrent anterior shoulder instability (RAGHI) during the COVID-19 pandemic with remotely-based rehabilitation, to those who had surgery before the pandemic and had in-person rehabilitation therapy.
Methods
A retrospective case series of 68 patients were included and divided into two groups: In person-group and Home-based group. Western Ontario Shoulder Instability Index (WOSI) and Subjective Shoulder Value (SSV) scores were used to evaluate objective and subjective clinical parameters. Time and level of return to sports was studied by the Subjective Patient Outcome for Return to Sports (SPORTS) score.
Results
The mean SSV score was 82% (40–100) on the In-Person group compared with 87% (65–100) for the Home-Based group. Results for WOSI score were similar, with an average of 210.42 (90%) for In-Person and 261.45 (88%) for the Home-Based group (p 0.12). Return to sports was carried out in an average of 6.6 (4–16) months for In-Person group, compared to 6.5 (5–8) months for Home-Based.
Conclusion
Follow-up and rehabilitation methods for patients who underwent surgery for RAGHI, during COVID-19 lockdown, were not significantly (p 0.12) affected on functional and athletic return in comparison to traditional methods according to WOSI scale.
Level of evidence
IV Retrospective series of cases
Intro
Recurrent anterior glenohumeral instability (RAGHI) mainly affects young adults and has a variable clinical presentation.1–7 Functional limitation, reduced athletic performance and impaired quality of life, are the most frequent reasons for consultation. 8 Most cases of RAGHI require a surgical approach. 9 The most common techniques used today are arthroscopic Bankart surgery, with the anatomical reinsertion of the capsule-labral complex; and Latarjet surgery, using the coracoid process as a graft on the anterior aspect of the glenoid, allowing to solve complex instability scenarios with bone defects. 9
Statistically satisfactory results are achieved using both surgical techniques. 7 Numerous factors affect results on surgical treatments. 5 Postoperative rehabilitation and follow-up during the first semester is crucial, and traditionally performed in-person in specialized centers. This was highly affected during the COVID-19 pandemic. 1
At the beginning of 2020, the pandemic changed our medical practice, generating an impact that could become permanent in the modality of patient care.1,2 A cohort of patients affected by this context underwent a surgical procedure in the immediately preceding period and during the pandemic; lockdown in our country started on March 2020, affecting their postoperative follow-up and rehabilitation methods. Modifications of this essential aspect of treatment may predispose to suboptimal post-surgical results.2,10,11
The objective of this study is to evaluate the functional results and return to sports in patients treated for RAGHI according to their rehabilitation and medical follow-up methodology. Patients who have gone through the first six postoperative months during the COVID-19 pandemic performed an alternative, remotely-based rehabilitation method and in-person medical control (Home-Based group, HB) were compared with those who underwent surgery before the pandemic, performing all controls and rehabilitation in a conventional face-to-face way (IN-Person group, IP). Our hypothesis is that the patients in the HB group would have worse functional results and a lower average of return to sports compared to the IP group.
Methods
A retrospective study was carried out in a tertiary referral hospital. We included patients who underwent primary surgical treatment (Arthroscopic Bankart or Latarjet) for RAGHI between January-October 2019 and February-September 2020, under 50 years of age at the time of surgery, and with a minimum post-operative follow-up of 1 year. Patients with rotator cuff tears, humeral avulsion of the glenohumeral ligament, multidirectional instability and with previous surgery on the affected shoulder were excluded.
All surgical procedures were performed by the same surgeon. The Latarjet procedure was performed according to the original technique modified by Walch. 12 Bankart surgery was performed according to the technique described by Zimmermann. 13 The decision to perform Latarjet versus Bankart was taken by using the ISIS score, as described by Boileau. 14
Data was collected from the medical charts from the hospital. Quality of life measurement was evaluated with the Western Ontario Shoulder Instability Index (WOSI) 15 and subjective shoulder value assessment (SSV) method 16 The WOSI score instrument consists of 21 items. The patient is asked to grade the function of a specific item on a horizontal visual analog scale from 0 to 100 mm. The questions were divided into 4 sections (domains). There were 10 questions addressing physical symptoms and pain. Sport, recreation, and work were addressed in 4 questions. There was a section with 4 questions dealing with lifestyle and social functioning, and another section for emotional well-being with 3 questions. Each question results in a number between 0 and 100 and the total score was presented as a number between 0 and 2,100 (where 0 represents no deficit and 2,100 the worst). The score can also be presented as percentage of a normal healthy shoulder, which may be more clinically useful. SSV scale is defined as a patient’s subjective shoulder assessment expressed as a percentage of an entirely normal shoulder, which would score 100%. The time and level of return to sports was recorded and measured by the Subjective Patient Outcome for Return to Sports (SPORTS) score. 17 Complications, episodes of postoperative instability and reoperations were recorded. “Postoperative instability” was defined as an episode of glenohumeral dislocation that required reduction by a medical professional using the Zimmermann criteria, 13 and “Subluxation” as a subjective sensation of dislocation of the glenohumeral joint, followed by spontaneous reduction.
The patients were divided into two groups: IN-PERSON (IP) and Home-Based group (HB). The IP group, operated between January and October 2019, was evaluated with face-to-face medical controls at day 7, 15, 30, 60, 90 and 180 post operation. Additionally, they performed rehabilitation in a specialized center 3 times a week for 24 weeks (which is the standard practice in our country’s protocols) under the direct supervision of a physiotherapist with the possibility of using all the recommended equipment. They also carried out a rehabilitation program at home but personally instructed and controlled based on an exercise guide indicated progressively by the surgeon, which was indicated during clinical controls, independent from physiotherapy. Patients operated with the Bankart technique were immobilized for 4 weeks with a sling and underwent rehabilitation according to the guidelines of the American Shoulder and Elbow Society. This post-operative program consisted of 1 month of immobilization with a sling as previously described; elbow and wrist movements, trapezius and scalene exercises were authorized. Between the 4th and 6th week, passive and then active movements were indicated to regain range of motion without muscle strengthening until the second month, and after that the recovery phase of neuromuscular function and strengthening began. 18 The return to sport was allowed after 6th months. Some of these patients may have conditioned and delayed the return time to sports because of the pandemic’s government restrictions that banned team sports between April and August 2020. In Latarjet cases, post-operative program was performed with immobilization with a sling for 2 weeks. Active and passive mobility exercises during the first 3 months with a focus on regaining range of motion. After the 3rd month, if patients recovered their range of motion, a computed tomography control was performed to assess graft consolidation. Muscle strengthening exercises started in the 3rd month. After the fourth month, patients were allowed a progressive return to their previous sports. These guidelines are based on Liotard et al. 19 ’s study with 307 patients, with excellent results.
The HB group of patients treated between February and September 2020, which was affected by the pandemic, performed telerehabilitation once a week guided by a physiotherapist, doing a self-administered daily rehabilitation program, and conducting limited physical examinations. Times and phases of rehabilitation were respected. The difference with the IP group was that the rehabilitation was self-administered, guided by two weekly telemedicine sessions, exemplifying, and making corrections with schematic videos. In turn, the clinical face-to-face controls with their surgeon were carried out at 48 h, 15 days, and 3 months after surgery. In the same way as the IP rehabilitation, permission was granted to practice sports when having full range of motion, biological healing times of 6 months for Bankart, 4 months for Latarjet (consolidated CT-scan), and strengthening work completed. In this group although the rehabilitation and follow-up were compromised, return to sports was not affected in any way by government restrictions due to COVID 19.
Statistic analysis
Data were obtained from a sample with a normal distribution, which were expressed with their mean and respective standard deviation (±SD) or median and interquartile range according to distribution. This study is considered analytical and was analyzed through the T or Mann Withney test to determine the statistical significance (p ≤ 0.05) of the WOSI scale, the SSV scale, the return to sports in months and the level of competitiveness. between IP group and HB group. The comparison between demographic characteristics of both groups was carried out with the Snedecor’s F-test, with a p < 0.05 level of significance. The information obtained was stored in the Excel program and processed through the Graph Pad Prism 8.02 program.
Results
Patients demographics
Between January 2019 and September 2020, a total of 71 non profesional competitive athletes were surgically treated for RAGHI at our center. Of the total number of patients, one refused to participate in the study, and 3 were excluded because they did not reach the minimum follow-up of 1 year. Therefore, a total of 68 patients were included in the study. The average post-operative follow-up of patients was 29 months (25–33 months) for the IP group and 16 months (13–20 months) for the HB group. Regarding the epidemiological results, we could identify that both groups were comparable in distribution and have homogeneous characteristics. To corroborate this assumption, the homoscedasticity test was used using the Snedecor F- test, obtaining a value of F (1.2052) (95% CI: 0.36 – 2.12).
In-person group
Among the patients in the IP group, 28 (87.5%) were men and 4 (22.5%) were women. 25 were right-handed and seven left-handed, 20 of the surgeries (62.5%) were done on the dominant shoulder. 15 patients performed contact sports (47%) and 17 non-contact sports (53%), all of them were nonprofessional competitive athletes. 14 underwent Latarjet procedure (43.8%), and 18, Bankart surgery (56.2%) (Graph 1). The average number of preoperative dislocations was 7.3 (2–15) per person and time from first dislocation to surgery was 16.2 months (4–50 months). The average age at the time of the intervention was 22 years (20–27.5 years) (Table 1). Return to sports was 6.53 (4–16) months; of these, 26 patients (81.25%) reported returning with the same previous level. Of the operated patients, six (18.75%) did not return to the same sport that they did previously with an average SPORTS score of 7.5 (4–10); one of whom returned to the gym with isometric exercises at the time of the study. Of the remaining 5 patients, four reported not having returned to sport due to the isolation measures relative to the pandemic, and one due to fear of a new injury. Surgeries divided by technique. Demographic characteristics of the patients.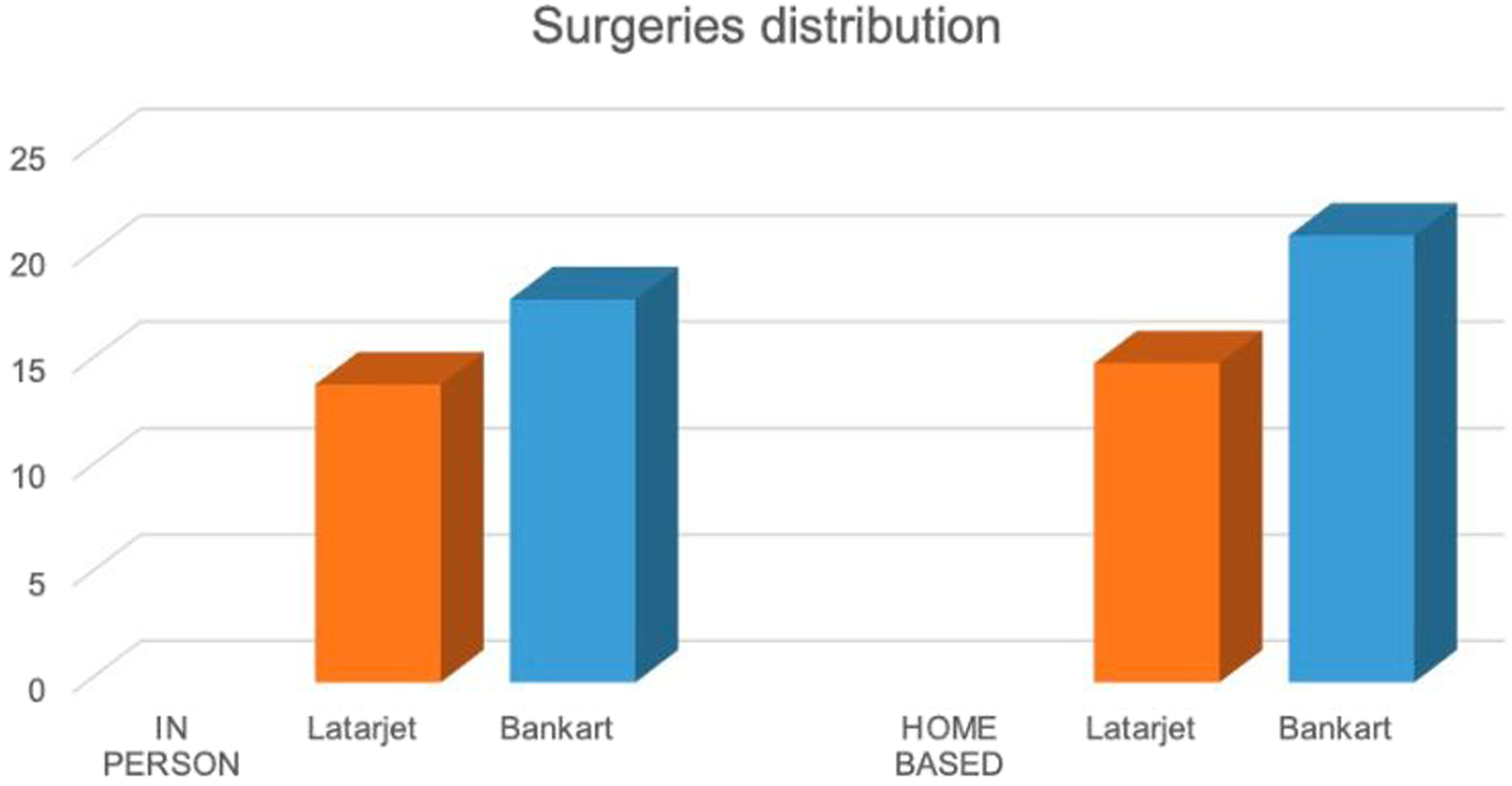
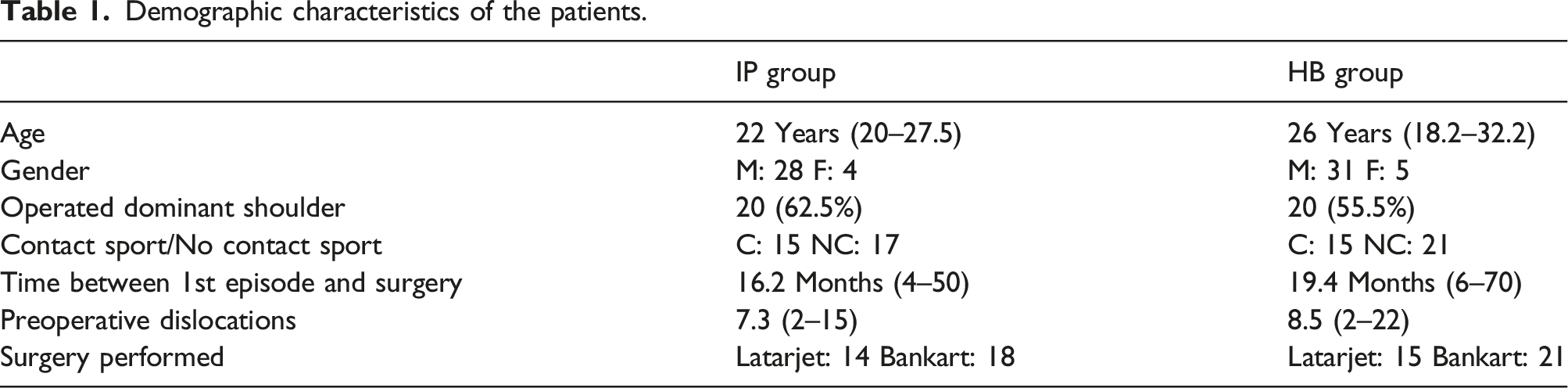
In this group, a patient operated with the Latarjet technique presented recurrent instability that required revision surgery by means of Eden Hybinette technique. 20
Home based group
Functional results. IP (InPerson). HB (HomeBased).

A patient undergoing the Latarjet technique presented an acute hematoma as a complication that had to be drained in the operating room. No re-dislocations or other complications were recorded in this group.
We consider it important to emphasize that both groups were affected by the pandemic restrictions in terms of their return to sports in different ways. In Argentina, sports activities were restricted from April to August 2020, therefore IP group had standard rehabilitation but some of them some of them may have delayed their return to sports due to the pandemic restrictions. On the other hand, HB group suffered a major modification in the rehabilitation and follow-up, however the return to sport was not directly limited by the pandemic.
Functional outcome
The mean SSV score was 82% (40–100) in the IP group compared to 87% (65–100) in the HB group, representing a non-significant difference (p 0.087). Regarding the WOSI score, the results were also not significant, this time with an average of 210.42 (90%) in the IP group and 261.45 (88%) in the HB group (p. 012).
Discussion
The main finding of this study was that the postoperative results and the level of return to sports of RAGHI were not significantly affected in the telerehabilitation and remote follow-up group.
Latarjet surgery was performed in the IP group in 18 occasions, and 21 were performed in the HB group (p: 0.33). On the other hand, arthroscopic Bankart surgery was performed in 14 and 15 occasions, (p: 0.33) respectively. In our study, 30 patients performed contact sports at an amateur competitive level; and within this group, 19 played rugby (63.3%).
Return to sports in operated patients shows good results in the literature.13,21–23 As Dekker demonstrated, in his paper where 23 athletes were evaluated, the average sports return was 4.5 months with both techniques. 24 In a comparative study, Blonna recorded an average of 6 months for sports discharge, without differences according to the technique of choice. 25 On the other hand, in his systematic review, Lalenti registered a return to sports at 6.1 (Bankart) versus 5.3 (Latarjet). 26 In our study, the patients in the IP group recorded an average of 6.53 months until returning to sports, against an average 6.5 months in the HB group, showing no significant differences (p 0.062). It is important to emphasize that our patients, especially in the HB group, had their return to sports affected in timing by the restrictions due to COVID-19 pandemic. Although these results are below those published in the literature by Dekker, with return to same sports level of 96%, and Mazzocca, 100%, the interviews with the patients showed us that 9 of the 10 patients who did not return to their sports activity corresponds to the sports restrictions imposed by the COVID-19 pandemic, where for long periods of time the sport was limited and even prohibited .24,27
Hovelius reported in his study excellent results, a WOSI score with an average of 88% with the Latarjet technique and 79% with the Bankart arthroscopic technique. 20 With high satisfaction rates, Blonna obtained 82% and 84% respectively. 24 Our study showed that both the IP and the HB groups showed a WOSI score of 89.98% and 87.55% respectively, without significant differences (p 0.012).
Gilbart, in his comparative work between the SSV and Constant scores, concludes that values higher than 75% represent high rates of satisfaction. 16 In our study, we recorded an average of 82.35% (40–100) in the IP group and of 86.78% (65–100) in the HB group, with results comparable to those reported in the literature by Blonna, with 86%, and Ernstbrunner, with 86%.25,27
At the time of this study, only one article published in the literature was found that compared rehabilitation in specialized centers to home telerehabilitation, in patients surgically treated for RAGHI. Ismail evaluated the postoperative results of only Bankart surgery, obtaining similar results in ROM and function on both groups, concluding that both rehabilitation modalities were equally effective in the treatment of RAGHI. 22 Similar conclusions were reported in the published literature, where both types of rehabilitation methods following different orthopedic surgeries are compared.28,29 In his review of the postoperative rehabilitation techniques for rotator cuff repair, G. Longo concludes that in literature there are no significant differences between both forms of rehabilitation in terms of satisfaction and functionality. 28 In another prominent article, where M. Buhagiar evaluated the postoperative results of total knee replacement; he shows that there is no superiority concerning the types of rehabilitation. He suggested that home-based rehabilitation is the rehabilitation of choice in patients with conventional surgeries. 29 In accordance with the bibliography, our study also did not show significant differences between the two forms of rehabilitation, demonstrating that good functional results and a high return-to-sports rate can be achieved both ways.
Our study has certain limitations. (1) Having used two different surgical techniques for treatment, even though both groups had a similar distribution of patients with both surgical treatments. (2) In our study we can also find a different frequency in the clinical evaluation based on government regulations because of the pandemic because both groups were evaluated in person, This is something that was not decided by the authors, but was an adaptation of our medical practice to the pandemic. (3) Evaluation of the moment of return to sport. Sports activities were heavily restricted between April and August 2020; so mainly the IP group had major restrictions. Strikingly, the results show similar return times, however, the comparison of the return time between both groups is a major limitation of the work. It was not possible to remove this bias for obvious reasons, and our patients live in different regions of our country, so the restrictions were not uniform, which further complicate the interpretation of return times. As strengths, the topicality of the subject and the possibility of providing information for future decision-making stand out. All surgeries were performed by one surgeon (DG) and the patients completed the same rehabilitation protocol giving validity to the conclusions obtained.
This is early preliminary evidence that telehealth might be a suitable alternative to more traditional face to face rehabilitation and acknowledge that further studies, such as in the form of a randomized controlled trials are needed to evaluate this further before any firm recommendations can be drawn.
Conclusion
Follow-up and rehabilitation methods for patients who underwent surgery for RAGHI, during COVID-19 lockdown, were not significantly (p 0.12) affected on functional and athletic return in comparison to traditional methods according to WOSI scale.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.