
Abstract
Purpose
Since its introduction in 1988, the double-tapered polished Exeter cemented stem has been widely adopted in primary total hip arthroplasty (THA). Despite the results coming from the arthroplasty registries have proven great survivorship, the aim of this study was to dig deeper and describe the modes of failure of the Exeter stem at 15 years follow-up while reporting the clinical and radiographic outcomes.
Methods
A search of PubMed, MEDLINE, and Embase was performed using the Preferred Reporting Items for Systematic Review and Meta-Analyses since inception of database to January 2022. A meta-analysis was performed on stem’s failure rates and clinical outcomes using random effects models. Publication bias was assessed with funnel plots.
Results
Overall, ten studies met the inclusion criteria with 2167 hips at mean 14.8 ± 4.1 years follow-up. The meta-effect estimate for revision rate for stem-related reasons was 3.8% (CI 95% 2.1–5.6, p < 0.01). The meta-effect for revision rate for stem aseptic loosening (AL) was 0.22% (CI 95% 0–0.4, p = 0.048) and for periprosthetic fracture was 0.6% (CI95% 0.3–0.9, p < 0.001). The meta effect estimate for Oxford Hip Score (OHS) at final follow-up was 32.4 (moderate; CI 95% 23.2–41.6, p <0.001) with and heterogeneity among the studies of I2 0%. Radiolucent lines were reported in 5.5% of cases, with 1.0% of cases (21 hips) reported to be progressive.
Conclusion
Current evidence suggests that the Exeter cemented stem not only has proven long-term outstanding reliability with a revision rate of 3.8%, but also incredibly low revision rates for AL (0.22%) and periprosthetic fracture (0.6%). It is suitable for a variety of indications, and the consistent radiological appearances indicate durable fixation and load transmission while being associated with a remarkably low stem-related complication rate.
Keywords
Introduction
Total Hip Arthroplasty (THA) is the gold standard in case of end-stage hip osteoarthritis. 1 Despite uncemented being the preferred method of fixation, 2 cemented stems have been reported to have excellent survivorship and clinical outcomes.3,4 Since its introduction, cementing technique has evolved from hand mixing and manual insertion with finger packing, to the modern generation that includes centrifugation, pulsatile lavage, cement plug with pressurization, stem preheating and centralizers.5–8
Cemented stems are associated with decreased risk of periprosthetic fractures, better control of the femoral version, and minimization of thigh pain. 9 Moreover, several limitations described in the past were based on outdated cementation technique that compromised the mechanical strength.1,10–12
The polished taper-slip Exeter Universal stem (Stryker, Kalamazoo, Michigan) was introduced in 1988 and it has been widely used in THA with outstanding results. 13 The Exeter V40 stem was then introduced in 2001, but apart from a minor change to the trunnion to the current 5°40′, the design has remained the same, and continues to perform well at medium-to-long term follow-up. 14
The long-term performance of this specific stem has been widely reported by studies and registries,13,15–25 however, registry reports do not clarify details on the modalities of failure of this stem. Therefore, we sought to evaluate via meta-analysis, the long-term failure rates (15 years) of the Exeter stem focusing on revision for stem related complications, revision for aseptic loosening (AL) of the femoral component, and revision for periprosthetic fracture. In addition, reporting on clinical outcomes, rate of radiological subsidence, and rate of radiolucencies of the cemented Exeter stem.
Materials and methods
Search criteria
This search was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA). 26 The US National Library of Medicine (PubMed/MEDLINE), EMBASE, and the Cochrane Database of Systematic Reviews were queried for publications utilizing the following keywords: “Exeter femoral stem” OR “cemented femoral stem” OR “cemented Exeter femoral component” OR “Exeter cemented system” AND “total” AND “hip” AND “arthroplasty” AND “primary” since inception of database to January 2022. No limit was set regarding the year of publication. Two authors (F.M. and H.T.) independently conducted all the searches and screened the titles and abstracts to identify relevant studies. Differences were resolved by consulting a third senior reviewer (C.W.J.). Only abstracts that evaluated the clinical outcomes of patients with Exeter femoral stem in primary THA with a follow-up greater than 10 years were reviewed. If the title and abstract of each study contained insufficient information, the full manuscript was reviewed. An additional search was conducted by screening the references list of each selected article, as well as the available grey literature at our institution. When studies were reporting outcomes on the same cohort of patients, the one with the longest follow-up was selected.
Inclusion and exclusion criteria
The inclusion criteria were: (1) clinical trials investigating the long-term (>10 years) outcome of the cemented Exeter femoral stem in primary THA, (2) primary outcomes recorded and assessed including (3) implant survivorship free of component revision, (4) revisions due to stem related complications (5) perioperative rates of mortality and complications, (6) clinical outcomes, and (7) radiographic outcomes.
The exclusion criteria were: (1) non-english language studies, (2) studies reporting on less than 10 hips, (3) biomechanical or preclinical studies, (4) studies exclusively using cementless primary THA or cemented THA other than the Exeter stem or hybrid THA including cemented acetabular component and cementless femoral stem, (5) studies on revision THA, (6) studies without clinical, functional, or radiological outcomes, (7) general review and systematic review, (8) registry-based studies, (9) studies with results including mixed types of femoral fixation without stratification per type of femoral fixation, (10) non full text articles, and (11) studies with less than 10 years mean follow-up.
Data collection
Two independent reviewers (F.M. and H.T.) separately examined all the identified studies and extracted data. During initial review of the data, the following information was collected for each study: title, first author, year of publication, study design, number of patients, patients died and lost at follow-up, age of patients, length of follow-up, indication for index surgery, stem revision rate, complication types, reoperations for any reason, implant loosening, dislocations, deep infections, periprosthetic fractures, patient-reported outcomes, and radiographic outcomes.
The level of evidence in the included studies was determined using the Oxford Centre for Evidence-Based-Medicine Level of Evidence (LoE). 27 The “quality assessment” of the studies for methodological deficiencies, as a common alternative to “risk of bias,” was examined by the modified Coleman Methodology Score (MCMS). The methodological quality of each study and the different types of detected bias were assessed independently by each reviewer, and then they were combined synthetically. Finally, a comprehensive analysis of the eligible studies was performed, focusing on specific questions that were relative to the topic. When more than one studies were reporting outcomes on the same cohort of patients at different follow-up times, the one with the longest follow-up was included in the meta-analysis to avoid reporting twice the results of the same cohort.
When reported, the quality of the cementation technique was typically assessed using Barrack’s grading system 28 : grade A is defined as a white-out with complete filling of the medullary canal, grade B as radiolucent lines (RLLs) covering up to 50% of the cement-bone interface (slight defects), grade C as a defective cement mantle or RLLs covering between 50% and 99% of the cement-bone interface, grade D by having 100% of RLLs at the cement-bone interface or complete absence of cement distally and failure to cover the tip of the stem. RLLs were defined as per Kobayashi et al. 29 while osteolysis was described as a progressive non-linear lucency of >2 mm resulting in endosteal erosion of cortical or cancellous bone. 30 The position of lucent lines in the femur was assessed using the zones described by Gruen et al. 31 and extended by Johnston et al. 4 Subsidence of the femoral stem was measured using the method described by Fowler et al. 32
Statistical analysis
For survivorship, the overall number of stems revised, the number of stems revised for AL, the number of stems revised for periprosthetic fracture, and the number of stable stems revised in the context of an acetabular component revision, were the most reported outcomes and used for meta-analysis. For functional outcomes, the Oxford Hip Score (OHS) 33 was the most reported outcomes and used for meta-analysis.
Due to methodological differences of the included studies, random effects models were used to combine reported outcomes. This decision was made, having considered a fixed-effects model not feasible due to outcomes in which the variation in study effects is assumed to occur from sampling error alone as opposed to between-study differences. I2 was reported for each outcome, representing the proportion of variation due to between-studies differences or heterogeneity.
Confidence intervals (CI) at 95% for individual studies are based on normal distribution for clinical scores and binomial distribution for survivorship outcomes. Proportions were combined using a raw proportion model.
Funnel plots were used for each measure meta-analyzed to explore for evidence of publication bias and results were considered statistically significant with an α error of 0.05. All analyses were performed using Jamovi V2.3.9.
Results
The literature search initially yielded 570 relevant citations (Figure 1). After removal of duplicate studies, 392 were subject to application of the predetermined inclusion and exclusion criteria. Following application of these criteria, 28 studies were subject to a full-text screening process. Ultimately, ten studies were included for analysis13,15–25 (Table 1). PRISMA flow diagram outlining the systematic review process. Baseline characterics of the studies. N/A: Not Available; BMI: Body Mass Index; LoE: Level of Evidence; yrs: Years; M: Male; F: Female.

All ten studies were a retrospective cohort design with a level IV LoE. The mean Modified Coleman Score was 61.1 ± 6.4, with scores ranging from 66 to 48, indicating a moderate methodological quality. The mean follow-up was 14.8 ± 4.1 years. A total of 2924 hips were initially included in the studies, while at long-term follow-up 2167 were available (74.1%), in line with the percentage of patients lost to follow-up for long-term studies.15,21,22,34 Mean age of the patients at time of index surgery was 57.9 years (range, 31–69 years) (Table 1).
Indications and characteristics exeter stem total hip arthroplasty.

N/A: Not Available; LV: Low Viscosity; MV: Medium Viscosity; HV: High Viscosity; SS: Stainless Steel; FH: Femoral head; IA: Inflammatory Arthritis; AVN: AVASCULAR necrosis.
Survivorship
All ten studies reported on stem revisions (146 revised stems of 2167). The meta-effect estimate for overall revision rate at 15 years follow-up was 8.3% (CI 95% 2.7–13.9, p = 0.004), however, when excluding the number of well-fixed stems revised during cup revision to provide better exposure, the meta effect estimate for long-term revision rate for stem-related reasons was 3.4% (CI 95% 1.7–5.2, p < 0.01) (Figure 2). If considering a mean follow-up >20 years (mean, 20.3 years), the meta-effect estimate for the overall revision rate was 18.7% (CI 95% 4.3–33, p = 0.011) (Figure 3). Forest plot for overall stem revision rate and revision rate for stem-related reasons. Forest plot for >20 years stem revision rate and revision rate for stem aseptic loosening.
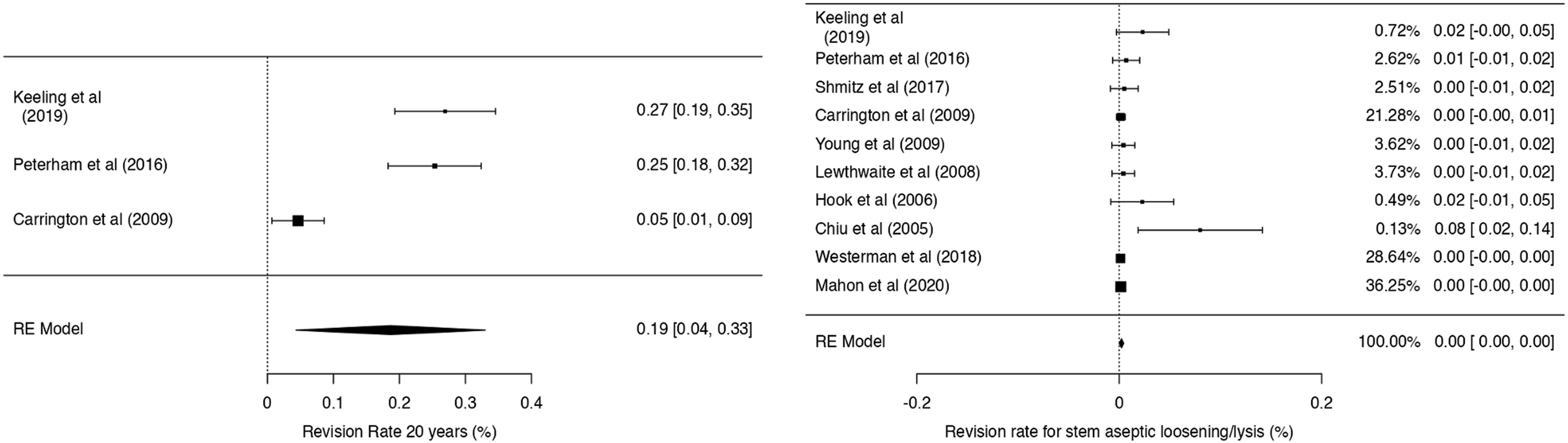
All studies reported on the number of stems revised for AL (13 stems of 2167), demonstrating a meta-effect estimate of 0.22% (CI 0–0.4, p = 0.048) with heterogeneity among the studies of I2 9.23% (Figure 3). When considering the number of stems revised for periprosthetic fracture (16 stems of 2167), the meta-effect estimate was 0.6% (CI95% 0.3–0.9, p < 0.001) with heterogeneity among the studies of I2 0% (Figure 4). Forest plot for stem revision rate for periprosthetic fracture and Oxford Hip Score.
Clinical outcomes and perioperative morbidity
All studies reported on clinical outcomes, however, the most commonly used clinical scoring system was the OHS in six studies.13,15,17–19,21,23,24 The meta effect estimate for OHS at final follow-up was 30.7 (CI 95% 20.8–40.5, p < 0.001) with and heterogeneity among the studies of I2 0% (Figure 4).
Survivorship and complications of exeter hip stems.
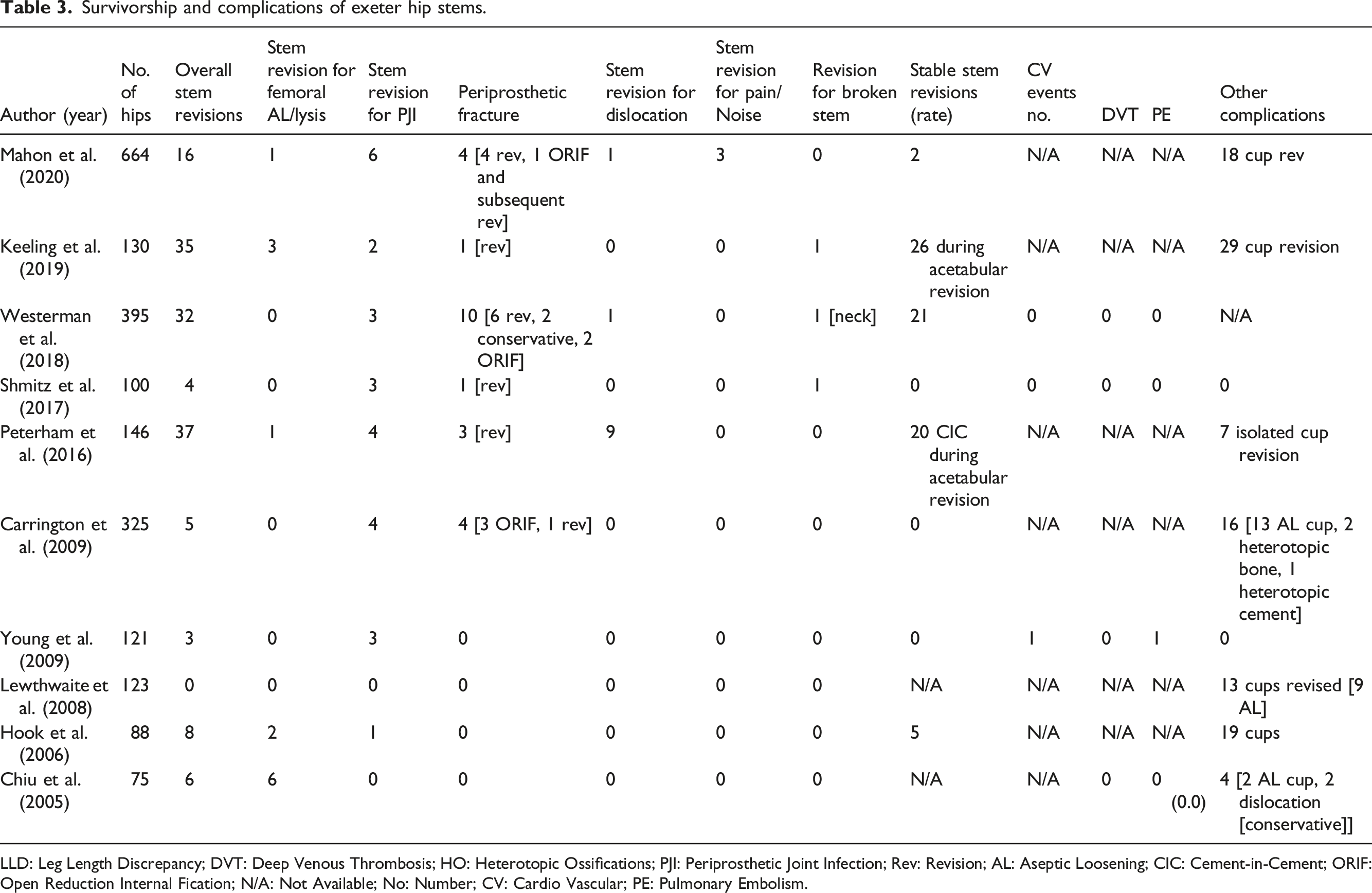
LLD: Leg Length Discrepancy; DVT: Deep Venous Thrombosis; HO: Heterotopic Ossifications; PJI: Periprosthetic Joint Infection; Rev: Revision; AL: Aseptic Loosening; CIC: Cement-in-Cement; ORIF: Open Reduction Internal Fication; N/A: Not Available; No: Number; CV: Cardio Vascular; PE: Pulmonary Embolism.
Radiographic outcomes
Radiographic outcomes were available at a mean follow-up of 15.2 ± 4.41 years, and focused on implant alignment, stem subsidence, presence and progression of peri-implant RLLs. Five studies (1172 hips) reported Barrack Grade classifications17–19,23,25 with 745 hips available for review at the time of follow up reporting grade A, B, C, and D in 406 (36.6%), 224 (19.1%), 87 (7.4%), and 8 (0.68%) hips, respectively. Ten cases (0.85%) were not classified due to poor-quality radiographs, and the remaining cases were not classified due to failure to report grades, lost to follow-up, or death during the follow-up period.
Clinical and radiographic outcomes of exeter hips stems.
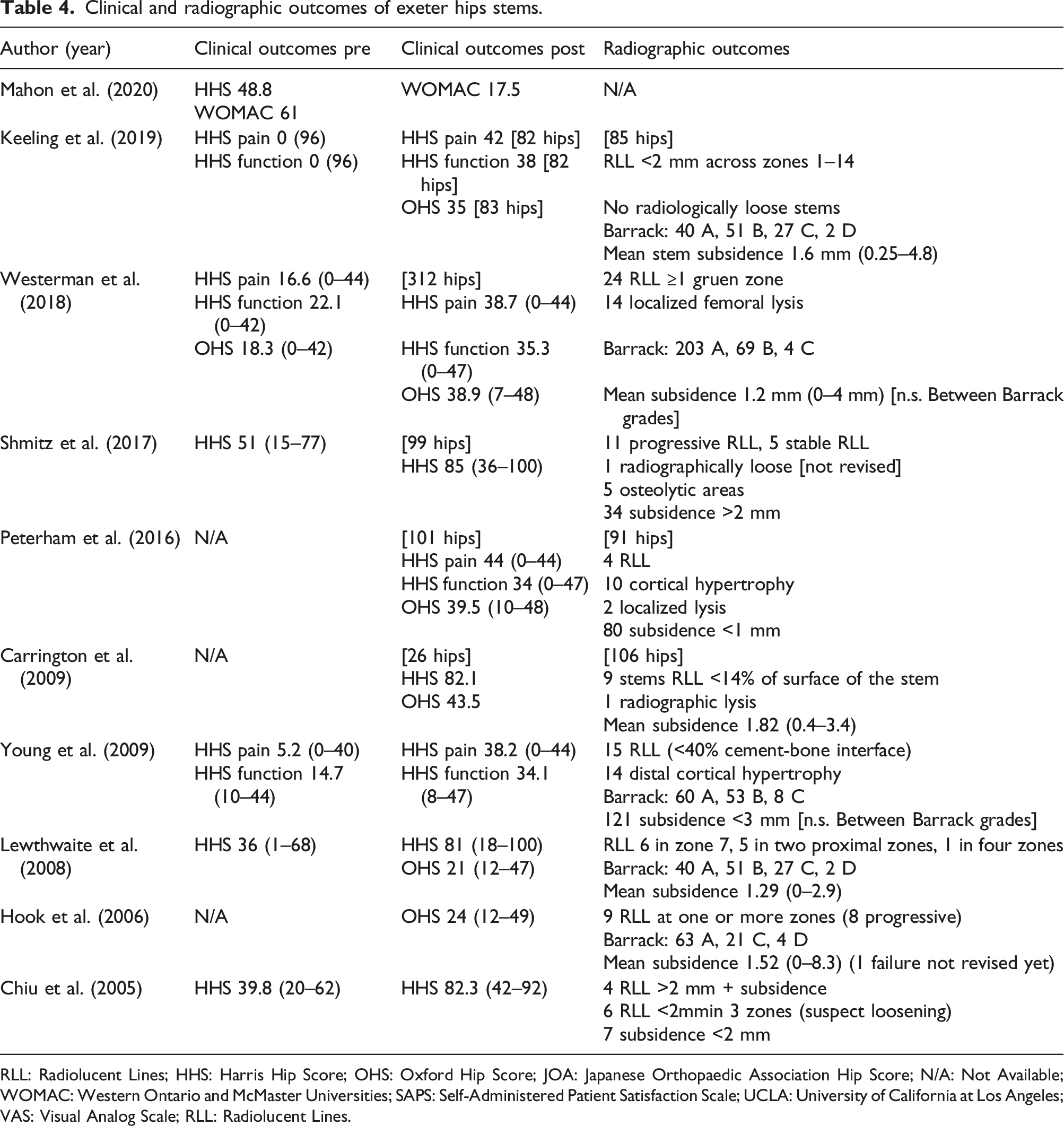
RLL: Radiolucent Lines; HHS: Harris Hip Score; OHS: Oxford Hip Score; JOA: Japanese Orthopaedic Association Hip Score; N/A: Not Available; WOMAC: Western Ontario and McMaster Universities; SAPS: Self-Administered Patient Satisfaction Scale; UCLA: University of California at Los Angeles; VAS: Visual Analog Scale; RLL: Radiolucent Lines.
Publication bias
The reported funnel plots show the level of publication bias; funnel plots are based on symmetry and when asymmetry is shown the plot is suggestive of publication bias.
35
Regarding overall stem revision rate, the funnel plot visually suggests publication bias with smaller studies reporting higher revision rates (p < 0.001). Regarding revision rate due to stem AL, the funnel plot visually suggests modest publication bias with smaller studies reporting higher revision rates (p = 0.003). For revision rate for periprosthetic fracture and for OHS, the funnel plots did not suggest any obvious publication bias (p = 0.369 and p = 0.55). The plots show that for larger studies the error associated with their estimate effect gets smaller, meaning that larger studies are associated with less variation around the true effect while smaller studies associated with greater error may have greater variation (Figure 5). Funnel plot for measured outcomes.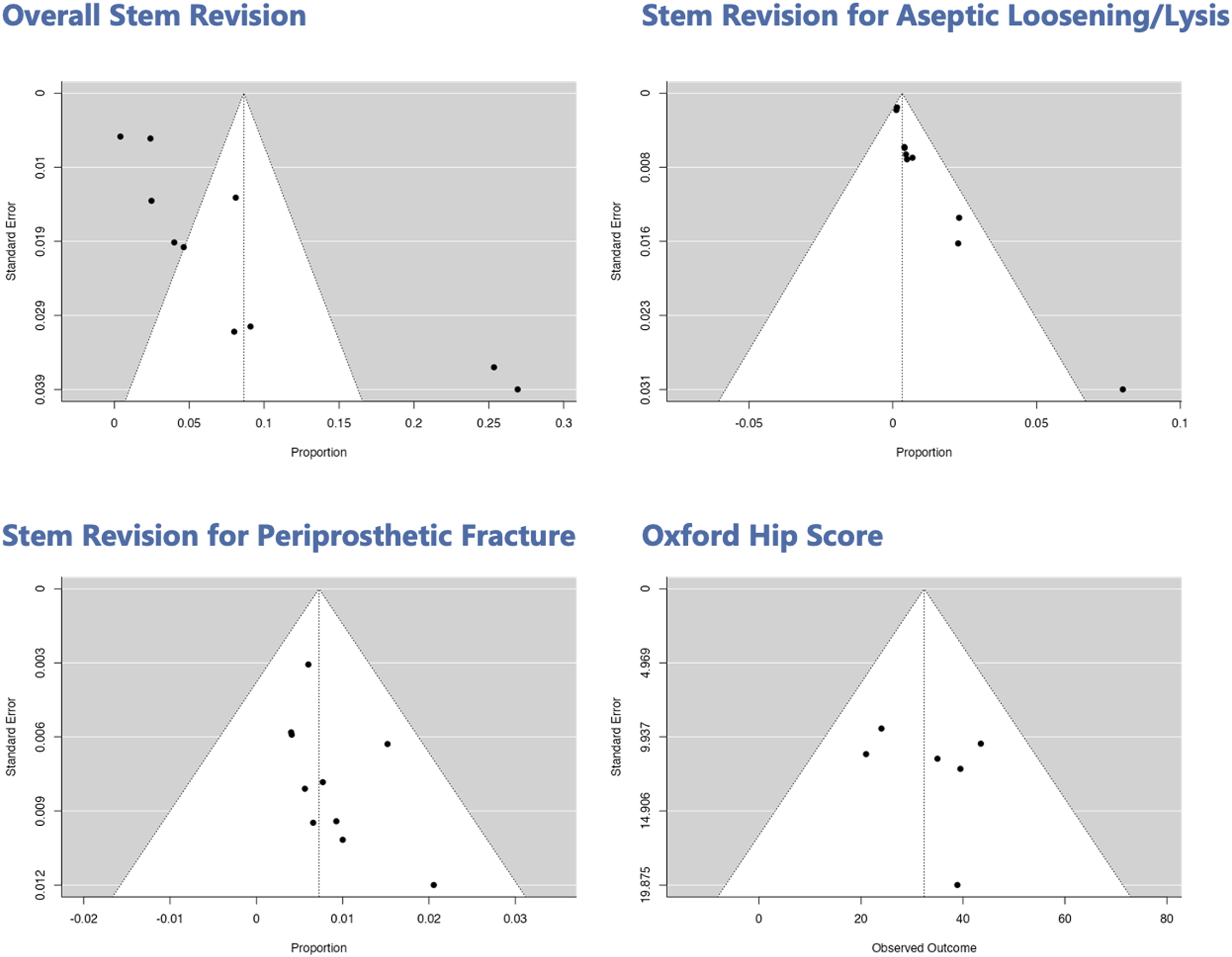
Discussion
In this meta-analysis on long-term outcomes of the Exeter cemented stem in primary THA, we confirmed the well-established excellent overall 15 years survivorship. In addition, we quantified the long-term revision rate for stem-related complications, for AL of the femoral component and for periprosthetic fracture, reporting outstanding results. Difficulties with loss to follow-up can be an issue with long-term studies and the way in which the data is reported, including reporting of numbers remaining at risk at the tail, therefore results must be interpreted with caution. The meta-effect for >20 years stem revision rate was 18.7% (CI 95% 4.3–33, p = 0.011), comparing favorably with studies reporting failure rates up to 35–40% at 20 years follow-up.34,36
Registry reports are extremely important in total joint arthroplasty to evaluate the overall performance of a specific implant design. However, one big limitation is the lack of details regarding the different modes of failure of an implant. If we consider the national registries reporting the highest number of Exeter cemented stems, the overall revision rate at 15 years follow-up of this meta-analysis (8.3%) is in line with the most updated data. The National Joint Registry of England, Wales and Northern Ireland (NJR) reported a revision rate between 2.91 and 7.11% at 15 years. 37 Similarly, the AOA reported a revision rate between 5.6 and 9.8% at the same time mark. 14
Nevertheless, when digging deeper into the long-term performance of the Exeter stem, registries come short in providing additional details. Despite an overall revision rate of 8.3%, the 15 years meta effect estimate for revision rate for stem-related reasons was 3.4% (CI 95% 1.7–5.2, p < 0.01). This because when analyzing the reasons of revision, the authors noted that often a well-fixed Exeter stem was revised with the cement-in-cement (CIC) technique during cup revisions,15–21 highlighting the ease with which this stem can be removed from the cement mantle and exchanged for another one. 38 In addition, after thoroughly analyzing implant failures, the meta-effect for revision rate due to stem AL was 0.22% (CI 0–0.4, p = 0.048). This extremely low rate of AL suggests that the polished tapered Exeter stem provides outstanding reliability and durable mode of fixation after primary THA.
To support the exceptional outcomes of the Exeter stem, our results showed that the femoral component was considered directly related with hip dislocation/instability in 0.005% of the cases (11 stems of 2167 hips), and therefore revised. It is worth noticing that this result compares favorably with data reported on the NJR for either overall cemented (patient time incidence rate [PTIR] 0.8), uncemented (PTIR 0.8) or hybrid fixation (PTIR 0.93). This finding supports the advantage of a cemented stem to allow the surgeon to freely decide the femoral anteversion despite the native bony anatomy and therefore to achieve a more accurate combined version. 39 Moreover, the meta-effect estimate revision rate for periprosthetic fracture was 0.6% (CI 95% 0.3–0.9, p < 0.001) suggesting favorable loading of the femoral bone comparing favorably with the current overall incidence of periprosthetic femur fracture of approximately 4.1%, with higher rates reported for uncemented and revision THA.40,41 It has been reported that late periprosthetic fracture usually account for approximately 6% of revisions and is the third most common reason, after AL and infection.42,43 This can be explained because of the more forceful procedure of trying to achieve a tight interference fit of the uncemented prosthesis compared to cemented devices where a space is left for the cement to act as a grout, thereby reducing the iatrogenic femoral fracture that occur more commonly with cementless prosthesis.
Cementation quality among the studies was reported to be either Barrack type A or B, suggesting high quality of the technique with only 0.7% of the cases being type D. This information relates to the low incidence of AL of the implants. Moreover, radiological review showed that the number of hips with radiolucent lines was small (5.5%), most of them <2 mm and stable, and that progressive ones were reported only in 1% of the cases. The mean subsidence was 1.45 ± 0.27 mm, ranging from 0.00 mm to 8.30 mm, with an average stem subsidence among the studies of <2 mm, in line with what reported by Murray et al.44,45 with a 10-year migration of 1.91 mm, 1.09 of which occurred between years two and ten. This shows once again the strong stability and great reliability of the Exeter stem, proving that progressive migration of this type of stem is not associated with subsequent increased rate of AL. These radiological findings reinforce the taper-slip theory of functioning of the stem where a small amount of subsidence in the cement mantle is a physiological behavior of this design and is not indicative of loosening and failure.46–48 Loudon and Older 49 described femoral component subsidence of more than 2 mm as abnormal. According to our data, only one study 23 reported on cases of subsidence of the femoral component >3 mm (3.6% of that cohort), however, none of them were revised for AL.
On the other hand, the use of cement may relate to disadvantages including a rare but severe risk of cardiovascular complications due to embolism and longer operative (OR) time compared to the use of uncemented prosthesis. 50 However, the infection rate seemed to not be increased by the longer OR time with a stem revision rate for PJI of 1.3%, in line with the current literature, and only one study reported 2 cases of death in the immediate postoperative period (of 2167 patients, 0.0009%), 1 PE-related and 1 MI-related. 25
There were a variety of limitations to this study, including the ones inherent with the approach to conducting a systematic review and meta-analysis. First, due to our strict inclusion and exclusion criteria, only 10 studies were selected for evaluation. Not all studies reported all the same data point and there were studies missing one or more of the variables we used in our analysis. As a result, there was variability in the overall pool of patients and hips that were evaluated for each outcome. This variation of total patients evaluated for each outcome must be considered when interpreting these results. However, achieving a follow-up of more than 20 years is not easy, especially considering as THA is usually undertaken in elderly patients. Second, we were limited by the quality of the original studies, the variability of the preoperative diagnosis, the different cementation techniques, and number of patients analyzed. Third, our methodology did not allow for identification of unpublished literature and is limited by potential publication bias. Fourth, several different outcome scores were used across the included studies to assess overall hip function and the long-term follow-up might have been adversely affected by significant numbers of patients lost and dead during at follow-up. Finally, we deliberately excluded registry-based studies to keep relative homogeneity of number of patients, surgeons performing the operation, and cementation technique.
Conclusion
To sum up, this meta-analysis confirmed the excellent long-term survivorship of the Exeter cemented stem after primary THA. In addition, it showed the principal long-term reasons of failure proving extreme reliability regarding implant fixation with a revision rate for AL of 0.22% and exceptional bone loading of the taper-slip design with a revision rate for periprosthetic fracture of 0.6% at 15 year follow-up. Moreover, this stem was associated with outstanding clinical and radiological outcomes, and it was frequently and easily revised with the CIC technique to provide better surgical exposure in case of cup revision.
Footnotes
Author contributions
FM and MM: Conceptualization. FM and HT: Data curation, formal analysis, investigation. MM, TB, and CJ: Supervision and validation. FM: Writing the original draft. MM, TB, and CJ: review and editing. FM, HT, CJ, TB, and MM: Final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial or material support for the research, authorship, and/or publication of this article.