
Abstract
Purpose
Finite element (FE) analysis and clinical follow-up were used to evaluate the efficacy of modified scarf osteotomy for moderate-to-severe hallux valgus (HV).
Method
We retrospectively evaluated 42 patients (44 feet) who underwent modified rotational scarf osteotomy for moderate-to-severe HV at our institution between January 2010 and January 2019. Radiological indicators and subjective scores were recorded at different time points. To compare the results and elemental characteristics, a FE model of the metatarsophalangeal (MTP) joint that included anatomically realistic geometrical and structural characteristics was built. The biomechanical features and correction differences in dynamic loads as well as the incidence of troughing were estimated.
Results
Both the hallux valgus angle (HVA) and intermetatarsal angle (IMA) showed significant improvement 6 weeks postoperatively (p < 0.05); additionally, the HVA increased from 6 weeks postoperatively to the last follow-up, while the IMA showed no significant changes (p > 0.05). The subjective scores significantly improved from the preoperative period to the last follow-up. The percentages of troughing and recurrence were remarkably low in our pilot study because of the innate stability of the modified rotated fixation.
Conclusion
Our preliminary findings suggest that modified rotational scarf osteotomy offers sufficient stability, correct HV deformity effectively, and good clinical outcomes for moderate to severe HV.
Introduction
Hallux valgus (HV) is characterized by a lateral deviation of the hallux accompanied by a medial displacement of the distal end of the first metatarsal. For moderate-to-severe hallux deformities, first metatarsal osteotomies are often performed to restore first ray alignment. 1 The scarf osteotomy, which was first reported in 1926, is used to correct mild to severe hallux deformities. Although the clinical results are satisfactory,2–4 several complications of a mechanical nature have been reported, 5 notably fracture, troughing and stiffness,1,6–10 with percentages as high as 10, 35 and 41.7%, respectively. Troughing is defined as the collapse of the cortex of the dorsal half of the osteotomy and wedging into the softer cancellous bone, with or without rotation of the plantar half of the first metatarsal shaft. Because traditional scarf osteotomy is associated with this unexpected complication at percentages ranging from 1 to 35%,11,12 numerous experiments on the biomechanical consequences of this invasive procedure have been performed to reduce the rate of complications and improve the surgical management of HV.
In an ideal osteotomy, the initial stability, established by covering the area and distributing the load strength over the osteotomy site, is of prime importance for facilitating earlier postoperative weight bearing. Innate stability is derived from the connected parts of two neighboring strong cortices. Thus, the rotational scarf method has been recommended as a modified procedure for avoiding functional elevation of the first ray and subsequent pronation of foot positions with an overload of the lesser metatarsals. 13
Finite element (FE) analysis is a method for simulating real objects using mathematics to find approximate solutions. It has been widely used in medicine, especially in orthopedics. FE analysis has been favored by many researchers to simulate specific body structures (such as bones) for mechanical analysis to conduct complex and detailed exploration.14–16 The literature shows that FE models used to analyze various mechanical characteristics of feet with HV can also be used to simulate different types of surgery to explore the advantages and disadvantages of each type. This approach can not only show clear and accurate results but can also serve as a powerful supplement to cadaveric biomechanics, which can effectively guide the selection of surgery in clinical practice.14,17
We reviewed the imaging data and functional scores of 42 HV patients (44 feet) who underwent modified rotational scarf osteotomy at different time points. Then, we built a FE model of the MTP joint that included anatomically realistic geometrical and structural characteristics and estimated the biomechanical features and correction differences in dynamic loading as well as the incidence of troughing. Our aim was to verify that the modified rotational scarf osteotomy procedure can prevent troughing; we performed a mechanical analysis of the FE model, assessed the follow-up data for clinical cases, and calculated the clinical and radiographic parameters of the improved rotational scarf osteotomy.
Patients and methods
This study was approved by the ethics committee of our hospital (KY2019150). A retrospective analysis of patients who underwent modified rotational scarf osteotomy in our institution from January 2010 to January 2019 was conducted. Inclusion criteria: patients with moderate to severe HV; patients treated with modified rotational scarf osteotomy. Exclusion criteria: patients with complex forefoot deformity requiring additional correction, inflammatory arthritis, history of forefoot surgery, rheumatoid arthritis, or neurogenic disease; patients lost to follow-up; patients with concomitant serious medical diseases. According to the inclusion and exclusion criteria, 42 cases (44 feet) were finally included for follow-up analysis.
Operative procedure
All surgeries were performed by the same surgeon, who had more than 10 years of clinical experience. The patients were placed in the supine position and underwent lumbar anesthesia or nerve block anesthesia. The senior surgeon operated on all feet with the same surgical technique; the technique was largely consistent with that described by Barouk.
6
A longitudinal incision approximately 6 cm long was created on the inside of the first metatarsophalangeal (MTP) joint (Figure 1(a)), and the skin and subcutaneous tissue were incised in turn to expose the first MTP joint. Then, the joint capsule was incised, and osteophytes on the medial side of the metatarsal head were removed with a pendulum saw. After the medial joint capsule was released, the adductor hallucis muscle was transected outside the first MTP joint, and the first metatarsal shaft was exposed for “Z”-shaped osteotomy
18
(Figure 1(b)). The distal point of the “Z”-shaped osteotomy was located approximately 10 mm proximal to the cartilage surface, whereas the proximal end was located 10–20 mm distal to the metatarsal-cuneiform (MC) joint. Two short parallel cuts at both ends of the longitudinal osteotomy were performed at an approximately 70° angle to the longitudinal axis (Figure 1(b)). The distal metatarsal head was shifted until it could move freely. The distal metatarsal head was rotated outward with the center of the metatarsal shaft cross section as the center of rotation. At this time, it could be seen that the joint surface of the proximal phalanx matched well with the joint surface of the metatarsal head. Two Kirschner wires were applied for temporary fixation. Under fluoroscopy, HV correction was observed to be acceptable and the MTP joint surface to match well (Figure 1(c)). Internal fixation was achieved with two cannulated screws (Bold 3.0 mm, INTEGRA, France). After the medial border of the bunion was trimmed, moderate medial capsular reefing was performed, and the skin was closed. Pictures of the modified scarf osteotomy. (a), Medial incision of the first metatarsophalangeal joint. (b), “Z”-shaped osteotomy. (c), Temporary fixation using Kirschner wire after rotation.
The sutures were removed 2 weeks postoperatively, and partial weight bearing was allowed within 6 weeks after surgery while the patients wore an Aircast (DJO USA) boot. The patients were instructed to perform active and passive exercises of the MTP1 joint and tape their big toes in a straight position. Every three weeks postoperatively, an interim X-ray was performed. If sufficient healing of the osteotomy was observed, then full weight bearing was allowed. In cases of concomitant interphalangeal deformities or severe HV deformities (8 feet, 18.2%), an Akin procedure of the proximal phalanx was also performed. The American Orthopedic Foot and Ankle Society Metatarsophalangeal-Interphalangeal Scale (AOFAS), visual analog scale (VAS), and Manchester-Oxford Foot Questionnaire (MOXFQ) scores were recorded at the preoperative and latest follow-up clinical evaluations.19–21
Radiographic assessment
A standardized weight-bearing radiographic gauge was used to assess and compare the preoperative and postoperative findings, including the hallux valgus angle (HVA), intermetatarsal angle (IMA), distal metatarsal articular angle (DMAA), joint congruency of the first ray and first metatarsal length (FML). Specifically, these radiographic parameters were evaluated preoperatively, six weeks after surgery and at the last follow-up. The congruence of the MTP joints was assessed by observing the degree of parallelism of the MTP articular surfaces.
Statistical assessment
SPSS 20.0 (IBM Corp, USA) was used for statistical analysis. Repeated-measures ANOVA was performed for radiographic parameters preoperatively, at 6 weeks after surgery and at the last follow-up. The least significant difference (LSD) method was used for pairwise comparisons. The three scores obtained before the operation and at the last follow-up were assessed by paired t tests, and p < 0.05 was considered statistically significant.
FE model construction
Material properties of the model components.

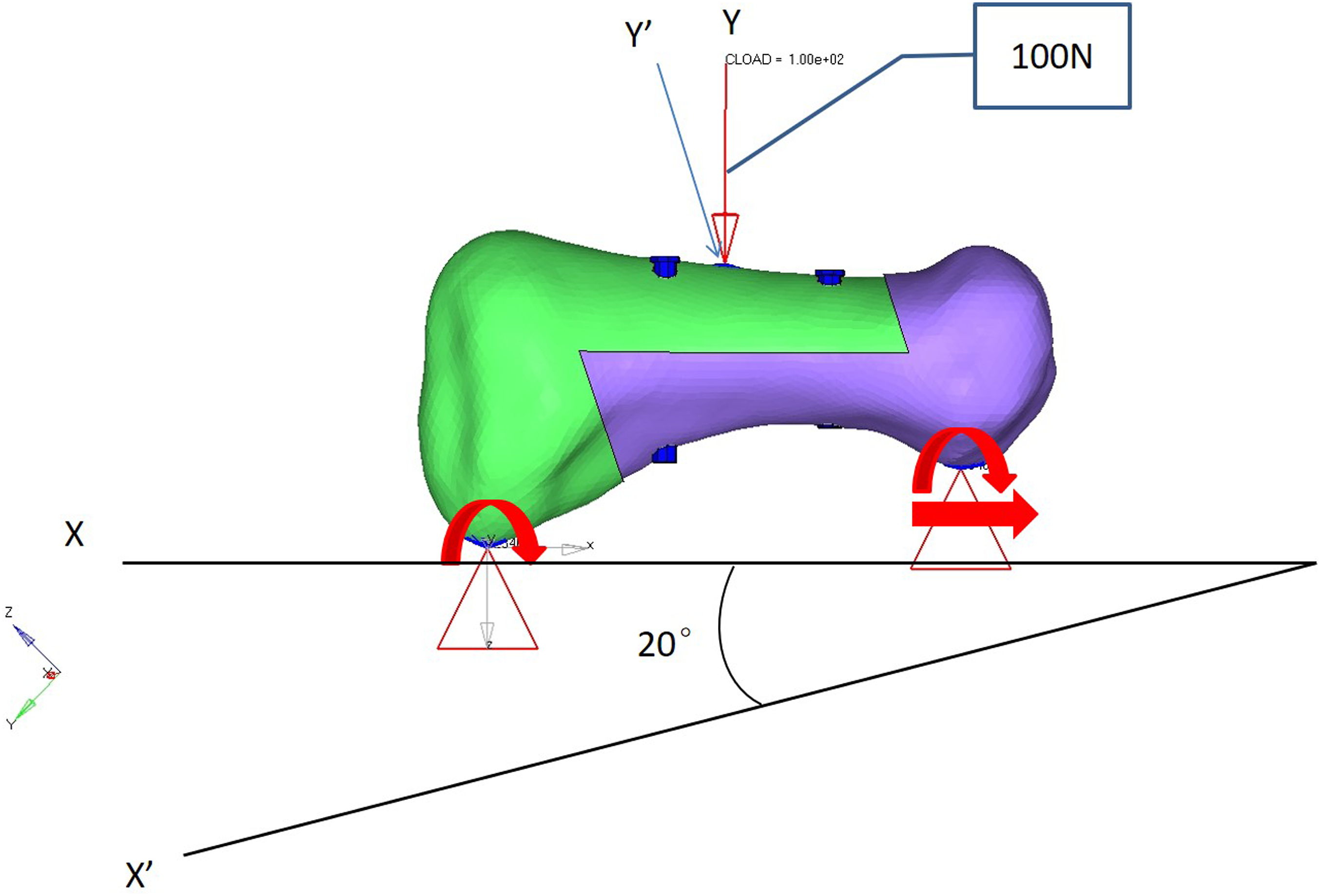
After the 3D model of MTP1 was constructed, all soft tissues, including the articular surfaces, ligaments and tendons, were removed. Surgery was simulated in detail based on our experience (Figure 2(a)). Two types of surgeries were performed: shifting (Figure 2(b)) and rotational (Figure 2(c)) scarf osteotomies (Group S and Group R, respectively). The contact area (CA) and loading distribution were measured. After correction and fixation, we put the first metatarsal in a horizontal position and at a 20° plantar inclination respectively, and applied a load of 100 N directly above it to conduct a three-point bending test at a rate of 100 mm/min (Figure 3). Failure loading and troughing complications were then assessed using the FE model. Illustration of the parameters used for the scarf osteotomy. (a), Sagittal view of the finite element model; the distances from the tip of the Z osteotomy (points a and b) to the joint surface are 1 cm and 1.5 cm, respectively. The two screws (diameter 4.3 mm) (points c and d) divided Line ab into three parts. The angle (Angles fba and eab) is 70°. (b), Group S. (c), Group R. On the axial view, the midpoints of Lines e’f’ and g’h’ are defined as points b’ and c’, respectively. Line a’d’ crosses from the midpoints of the proximal and distal articular surfaces (points a’ and d’). Three-Point bending test. The first metatarsal was placed in a horizontal position and at 20° of plantar inclination, respectively, and a load of 100 N was applied directly above it to conduct a three-point bending test at a rate of 100 mm/min.
Results
According to the inclusion and exclusion criteria, a total of 42 cases (44 feet) were included. Among them, there were 2 males, 40 females, 16 cases involving the right foot, and 28 cases involving the left foot; the mean age was 49.45 ± 17.47 (range 18–77) years, and the mean follow-up duration was 60.52 ± 28.44 (range 12–111) months.
Radiographic assessment
Comparative analysis of radiological indicators at different time points (N = 44).

HVA: hallux valgus angle; IMA: intermetatarsal angle; DMAA: distal metatarsal articular angle; FML: first metatarsal length.
p*: Comparison between the values obtained preoperatively and 6 weeks after surgery.
p**: Comparison between the value obtained at the last follow-up and 6 weeks after surgery.
p***: Comparison between the value obtained at the last follow-up and the preoperative value.
Clinical assessment
Comparative analysis of the three functional scores obtained preoperatively and at the last follow-up (N = 44).
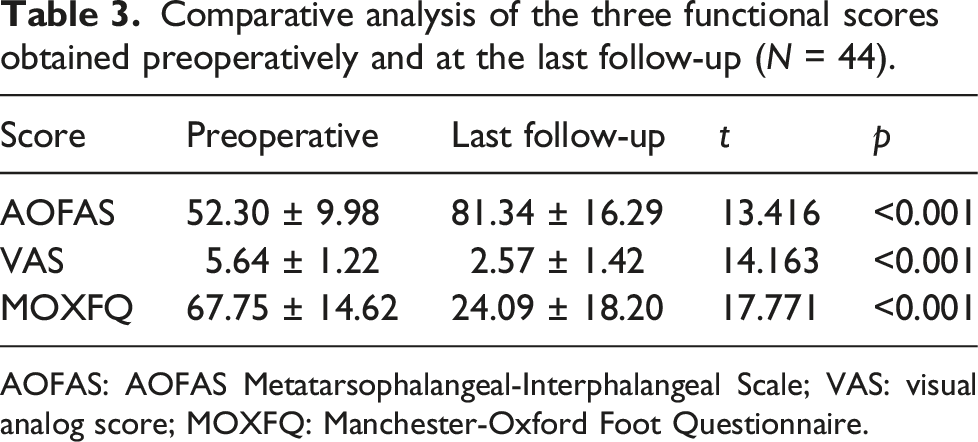
AOFAS: AOFAS Metatarsophalangeal-Interphalangeal Scale; VAS: visual analog score; MOXFQ: Manchester-Oxford Foot Questionnaire.
Complications
One fracture occurred intraoperatively at the proximal end of the osteotomy. We used a fragment fixation pin, and a short cast was applied for 3 weeks after surgery. Although a loss of motion at MTP1 occurred as expected, the degree of correction and patient satisfaction level were acceptable. Within the first six weeks after surgery, we did not observe delayed wound healing or other fractures of the first metarsal, consistent with the findings in the literature. 22 At the last follow-up, 11 patients (26.2%) had undergone reoperation to have their internal fixation removed. None of the patients underwent surgery because of a symptomatic recurrent HV deformity. However, certain patients were defined as “recurrent” according to the radiographic measurements. Furthermore, we did not observe pseudarthrosis, algodystrophy, osteonecrosis, deep venous thrombosis or other complications.
FE model findings
The scarf osteotomy was simulated on the model (Figure 2(a)). Two types of surgeries were performed: shifting (Figure 2(b)) and rotational (Figure 2(c)) scarf osteotomies (Group S and Group R, respectively). The results showed that the CA in Group R was significantly larger than that in Group S (CA Group S = 1.1252; CA Group R = 1.1368). Additionally, the maximum stress of the contact site indicated that the maximum stress deformation in Group S (dynamic maximum value, DMV = 1.91,537) was larger than that in Group R (DMV = 1.79,658) (Figure 4(a) and (b)). The same results were noted on the coronal view (DMV Group S = 0.01,420; DMV Group R = 0.00,949) (Figure 4(c) and (d)) and the sagittal view (DMV Group S = 0.00,139; DMV Group R = 0.00,138) (Figure 4(e) and (f)). Illustration of the dynamic volume at the interface. (a and b), Groups S and R, respectively, on the axial view. (c and d), Groups S and R, respectively, on the coronal view. E and F, Groups S and R, respectively, on the sagittal view under a vertical compressive load (100 N).
Under a 100 N vertical loading force, there was no significant difference in the DMV between the two groups on the sagittal plane (DMV Group S = 0.073; DMV Group R = 0.074) (Figure 5(a) and (b)). However, after the metatarsal head was set at a 20° plantar inclination, the DMV in Group R was lower than that in Group S (DMV Group S = 0.05,423; DMV Group R = 0.04,582) (Figures 5(c) and (d)). Illustration of the dynamic volume of the whole shift on the sagittal view. (a and b), Groups S and R, respectively. A vertical compressive load (100 N) was simulated. (c and d), Groups S and R, respectively, included an additional vertical compressive load (100 N). The shaft is at a 20° plantar inclination to simulate weight bearing.
Discussion
Traditional scarf osteotomy has been used to treat HV deformities.3,23,24 This procedure is performed only when the width of the shaft of the first metatarsal is sufficient, limiting the availability of this option for mild-to-moderate deformities. Devies suggested that under a lateral shift of the distal fragment, at least 1/4–1/3 of the shaft width should remain in contact. 25 When healing does not occur properly, the proximal medial cortex may encounter the distal lateral cortex in an extreme position. However, a medial displacement of more than 50% causes instability, especially with a high degree of intermetatarsal angulation. 6 This instability is a limitation of traditional scarf osteotomy. Previous studies that used rotational displacement reported correction rates of IM angle deformities as high as 23%, 13 expanding the indications to include severe deformities. Adam et al. 26 also noted that their scarf technique involving rotation combined with translation can effectively prevent the occurrence of troughing and yielded good correction. Kilmartin and O’Kane 27 assessed the long-term results of rotational scarf osteotomy and noted that, in the absence of troughing, the incidence of HV recurrence reached 8%. In longitudinal osteotomy, the two ends of the osteotomy line are positioned 2–3 mm away from the dorsal metatarsal side to prevent mutual incarceration of the cortical bone and cancellous bone after separation of the upper and lower ends of the broken end of the osteotomy. 28
The radiographic parameters (HVA, IMA, DMAA) were measured preoperatively by using the central axis of the metatarsal bone, 29 but the metatarsal anatomy changed after the operation, and the central axis was altered mechanically. The connection between the midpoint of the proximal joint surface and the midpoint of the distal joint surface was used as the reference line of the plantar diaphysis to measure the radiographic parameters. 30 Our results showed that rotational scarf osteotomy can significantly correct radiographic parameters in patients, but the HVA at the last follow-up was greater than that 6 weeks after surgery, which is consistent with the results of Sahin’s study, 31 indicating that the HVA has a certain degree of radiological recurrence; however, the IMA did not show significant changes within 6 weeks after surgery or by the last follow-up. In the FE model, the modified osteotomy procedure directly corrected the angle to a greater extent than the traditional scarf procedure. However, osteophyte formation may be excessive at the medial articular edge, 32 which can be misinterpreted as radiologic improvement.
An important factor that affects recurrence is preoperative joint congruity, suggested by Deveci to possibly be the only predictive factor. 32 Fuhrmann also believes that incongruent MTP joints are a very important reason for postoperative HV recurrence. 33 The response of subluxated incongruent MTP joints to DMAA cannot be corrected by scarf osteotomy alone. Many researchers have suggested that the addition of Akin osteotomy would be better for rectifying the interphalangeal deformity than adjustments to DMAA alignments caused by rotational osteotomy. 13 A retrospective research study by Fuhrmann showed that the radiological outcomes of 141 feet treated with an isolated scarf osteotomy remained unchanged within the first three months but worsened by the final radiographic assessment. 33 Recurrence was also reported by Bock at 1.5–2.8 years. 34 In several studies, although recurrence was not explicitly defined, it was considered to be a clinical development of HV after alignment correction.31,35 When the HVA exceeded 30° preoperatively, the results were even worse. In these cases, a combination procedure with Akin osteotomy is recommended. 33 After intraoperative scarf osteotomy, the IMA had improved well, but a few patients still presented with large HVAs. For 8 of these patients, we performed Akin osteotomy of the proximal phalanx in conjunction with a scarf osteotomy. However, the radiographic results were not different between these patients and those who had not undergone Akin osteotomy because of the greater expansion and stiffness caused by fixation of the IP joint. A previous study showed a relatively high radiographic recurrence rate of more than 30%; 36 however, symptomatic recurrence occurred in only 6.5% of patients. Another study showed that the primary concerns of patients were pain and shoe-fitting issues, with others including the restoration of an adequate MTP joint range of motion and relief of metatarsalgia. 27 The rate of patient satisfaction with regard to improved clinical results, including the AOFAS scores, was high.
In our clinical study, troughing was not identified during the follow-up period. The FE model showed that the rotator scarf procedure provided a larger CA than the traditional osteotomy because it allows spreading of pressure from one edge of the cortex to the other, causing the cortical shell of the dorsal fragment to form an “X” shape with the plantar fragment. Because the central axis of rotation around the first metatarsal was used and the IM angle deformity was reduced, the translating osteotomy performed in the traditional procedure was not needed. In addition, partial weight bearing was allowed for all patients at six weeks. As expected based on previous study findings,6,37 the special geometry of the osteotomy provided a relatively stable fixation that allowed more weight bearing in the early postoperative period. We also used two screws torqued to 5 Nm in the rotational scarf group. The maximum failure load caused much greater deformation with the modified osteotomy than with the traditional osteotomy.
However, the proximal screw can cause fractures because of insufficient bone stock. 38 Ideally, the screws should be placed perpendicular to the osteotomy line to reduce the risk of stress fractures. 39 Additionally, the traditional osteotomy likely resulted in better positioning of the two screws, whereas after translation with the scarf osteotomy, the oblique placement of the screws resulted in a less stable fixation. According to our FE model, the modified rotational osteotomy provides a larger area of coverage per degree of angle correction. In addition, the maximum stress of the contact site in Group R was significantly lower than that in Group S, whether on the cross sectional, coronal or sagittal plane, as was the result of the three-point bending test with a load of 100 N, indicating better stability in Group R.
Previous investigations have shown that troughing occurs even in distal metatarsal osteotomies.39–41 However, we found that the distal bone fragment produced a sliding vector created by weight before complete bone healing occurred. The “troughing” from the sagittal position rather than from the coronal view became defined as the notch wedged into the metatarsal head. Therefore, the postoperative broken end is more stable and less prone to pronation.
Rose showed that lengthening the alignment increased the stiffness of the first MTP joint. 42 Wirth and Lenz43,44 showed that shortening of the first metatarsal after surgery potentially leads to postoperative metatarsalgia. Our FE model showed that rotation around the proximal lateral corner of the distal fragment extended the FML. However, during the clinical follow-up period, there were no significant changes in the FML, as the rotational scarf procedure had limited influence on the change in the FML. If necessary, the metatarsal head could potentially be appropriately displaced distally to prolong the FML, but we need to investigate this concept in depth in future studies.
Our study has certain limitations. First, because a comparison was not performed against the results of traditional shifting osteotomies performed in patients in our pilot research, the results may not be sufficiently persuasive. Second, because of the lack of soft tissue lateral to MTP1, the FE model simulations were not completely accurate. Third, the assessment of the ankle in the FE model indicated that excessive osteophyte formation does not result in a change in the midpoint.
Conclusion
Our preliminary findings suggest that the modified rotational scarf osteotomy procedure can effectively correct HV deformity, maintain postoperative stability, and improve clinical outcomes
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Leading scientific and technological innovation talents of the National “10,000 Persons Plan” (414ZA1), 2019 Chief Medical Expert of Chongqing (414Z333) and Science and Technology Innovation Leading Talent Project of National 10,000 Persons Program (4139Z2B1).