
Abstract
Purpose
Because modified Broström procedure provides a restoration of mechanical stability by reinforcing attenuated host tissue, poor quality of remnant ligamentous tissue is considered as a prognostic factor for ligament repair surgery. The purpose of this study was to assess the intermediate-term clinical results after anatomic anterior talofibular ligament repair augmented with suture-tape for chronic lateral ankle instability (CLAI) with poor quality of ligament remnants.
Methods
64 patients with the insufficient anterior talofibular ligament confirmed by preoperative magnetic resonance image and intraoperative inspection were followed for ≥3 years after the augmented anterior talofibular ligament repair. The clinical outcomes were assessed with the Foot and Ankle Outcome Score, Foot and Ankle Ability Measure. Measurements on stress radiographs were performed to assess the changes of mechanical instability. To identify the changes of functional ankle instability, postural control ability was analysed with single leg stance test.
Result
Foot and Ankle Outcome Score and Foot and Ankle Ability Measure scores improved from preoperative mean 58.3 and 53.6 points to 90.2 and 88.7 points at final followup, respectively (p < 0.001). Talar tilt angle and anterior talar translation improved from preoperative mean 16.5° and 13.4 mm to 3.2° and 4.4 mm at final followup, respectively (p < .001). Two patients (3.1%) showed a recurrence of instability. Although balance retention time improved from preoperative mean 3.9–6.2 seconds at final followup (p < .001), a significant side-to-side difference was found.
Conclusion
Anatomic anterior talofibular ligament repair augmented with suture-tape appears to be a useful surgical option for CLAI with poor quality of ligament remnants at intermediate-term followup. Through anatomic repair of attenuated ligaments and suture-tape augmentation, this combined procedure can provide the reliable restoration of mechanical stability and advantages of the anatomic ligament repair. Postural control deficit compared to the uninjured ankle supports a necessity of continuous proprioceptive-oriented rehabilitation.
Keywords
Introduction
As a surgical treatment modality for chronic lateral ankle instability, the modified Broström-Gould repair is well known to be a representative procedure.1,2 However, the modified Broström procedure (MBP) alone is not always the most appropriate operative technique for patients with chronic lateral ankle instability.3–5 Although a consensus on the relative contraindications of the modified Broström procedure remains controversial, such conditions are known to include generalized ligament laxity (joint hypermobility), history of long-standing instability, severe obesity (high Body Mass Index), hindfoot cavovarus deformity, and failed previous ligament repair surgery.1,6–9 Patients with these poor prognostic factors may need a longer period of postoperative protection and have higher probability of recurrent ankle instability. Because the modified Broström procedure is an anatomic ligament repair surgery which depends on quality and quantity of the remnant ligamentous tissues, poor host tissue potentially can be another negative prognostic factor. 1 In contrast with other poor prognostic factors, the accurate evaluation for quality and quantity of remnant ligamentous tissues prior to surgery is likely to be a difficult problem to assess.
Many chronic lateral ankle instability patients have poor lateral ligaments and joint capsule following repeated sprain injuries. Although magnetic resonance imaging (MRI) analysis provides significant information in assessing the patients with chronic lateral ankle instability, it may be mainly simple interpretation such as the complete or partial rupture of the anterior talofibular ligament and calcaneofibular ligament (CFL). 10 In addition, recent systemic review reported a limitation of magnetic resonance imaging in detecting calcaneofibular ligament injuries in chronic lateral ankle instability. 11 Surgeons seems to frequently experience a inconsistency between preoperative magnetic resonance imaging and intraoperative findings of the lateral ligaments.12,13
Lateral ligaments reconstruction is typically undertaken for the patients with insufficient or poor-quality ligament remnants. A recent consensus report by Michels et al. 14 showed that most surgeons preferred the ligament reconstruction procedure in patients with poor ligament quality determined during surgery. However, the ligament reconstruction procedure needs additional skin incision and advance preparation for an autograft or allograft, when compared to the conventional lateral ligaments repair procedure. Therefore, a supplementary strategy based on the intraoperative findings of ligament remnants should be considered. Ligament augmentation with suture-tape in chronic lateral ankle instability has been introduced to protect an elongation of the repaired ligament by early load and to enhance a faster rehabilitation.15,16 As an alternative to insufficient repair construct, suture-tape augmentation may be helpful for patients with poor-quality of remnant ligament tissues. In addition, surgeons are able to perform ligament augmentation after decision making based on the intraoperative findings.
While the biomechanical superiority of suture-tape augmentation in chronic lateral ankle instability has been demonstrated,17–19 clear indications for its clinical use have not been established. As a strategy to improve the clinical results in patients with poor remnant ligament tissues, we hypothesized that anatomic anterior talofibular ligament repair augmented with suture-tape provides the enhanced mechanical stability and functional restoration without ligament reconstruction using tendon graft. In the current study, we aimed to assess the intermediate-term clinical results after anatomic anterior talofibular ligament repair with suture-tape augmentation for chronic lateral ankle instability with poor quality of ligament remnants.
Materials and methods
Research subjects
Between April 2012 and October 2018, a total of 104 patients (112 ankles) with poor quality of ligament remnants consecutively underwent anatomic anterior talofibular ligament repair augmented with suture-tape for chronic lateral ankle instability. Of these patients, 68 patients (68 ankles) who met inclusion criteria were enrolled, and 64 patients (64 ankles) with followup for more than 3 years after surgery were eventually analyzed (Figure 1). A quality of the anterior talofibular ligament remnants was confirmed with preoperative magnetic resonance imaging and intraoperative inspection. In the current study, a quality of the anterior talofibular ligament remnants was classified to three groups as follows: good (signal or width change on magnetic resonance imaging, but suitable to repair on intraoperative inspection), fair (deficient remnants on magnetic resonance imaging, but repairable on intraoperative inspection), poor (deficient or no remnants on magnetic resonance imaging and not suitable to repair on intraoperative inspection) (Figure 2). All the 112 ankles in this study were classified into the poor group. In addition, there were 81 ankles in the good group and 227 ankles in the fair group. All physical examinations prior to surgery and operations including intraoperative inspection were done by single senior surgeon, and all magnetic resonance imaging interpretations were done by one orthopedic surgeon and one radiologist. The reliability of the magnetic resonance imaging grading system used in the current study was evaluated by calculating intraclass correlation coefficients, which indicated interobserver agreement and intraobserver reproducibility. Intraobserver reproducibility of two researchers was average 0.92 (range, 0.91–0.94) and interobserver agreement between two researchers was average 0.9 (range, 0.84–0.95). Therefore, the reliability of preoperative magnetic resonance imaging interpretations was found to be excellent. The inclusion criteria in the current study were as follows: (i) poor quality of the remnant of anterior talofibular ligament as shown by magnetic resonance imaging and intraoperative inspection, (ii) unilateral ankle instability, (iii) no previous operation history involving the affected ankle, (iv) no generalized ligamentous laxity, (v) no osteochondral lesion needing microfracture or osteochondral graft. Eight patients (16 ankles) with bilateral ankle instability, 9 with previous surgical history, 7 with generalized ligamentous laxity, and 11 with advanced osteochondral lesion were excluded. In addition, one patient was unwilling to participate and was excluded from this study. Flow chart of the current research. A poor quality of the ATFL remnants confirmed with preoperative magnetic resonance image and intraoperative inspection. (a) Deficient or no remnants on MRI scan, and (b) a thin and weak remnant tissue not suitable to repair on intraoperative inspection.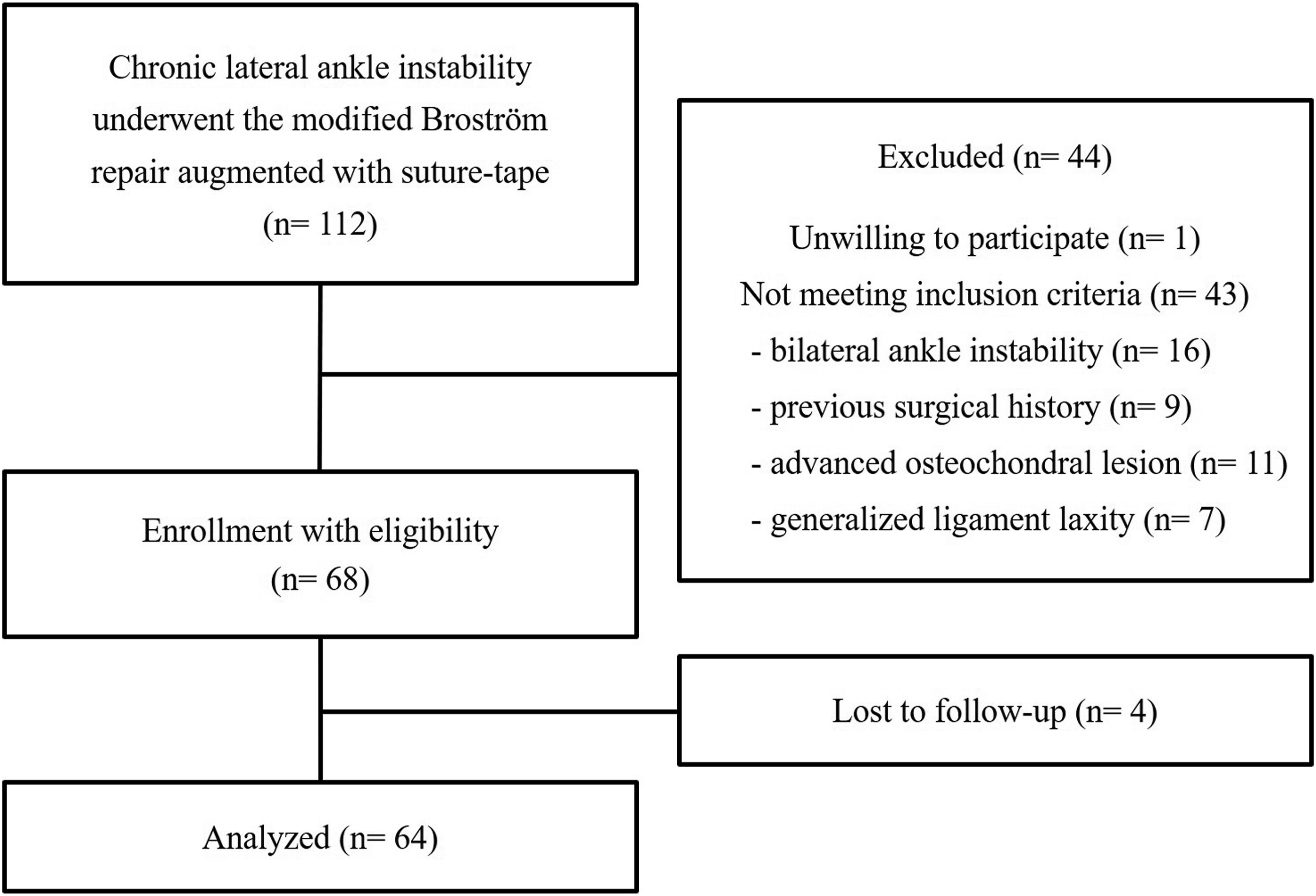

The mean age of patients was 30.3 years (range, 21–46 years), and the mean length of followup was 61.4 months (range, 36–114 months). The mean duration of ankle instability prior to surgical intervention was 58.8 months (range, 11–168 months). This study consisted of 23 male and 41 female patients. The mean body mass index (BMI) was 25.6 kg/m2, and no professional athletes were included. The study protocol and clinical research were approved by the ethics committee of Institutional Review Board.
Surgical technique
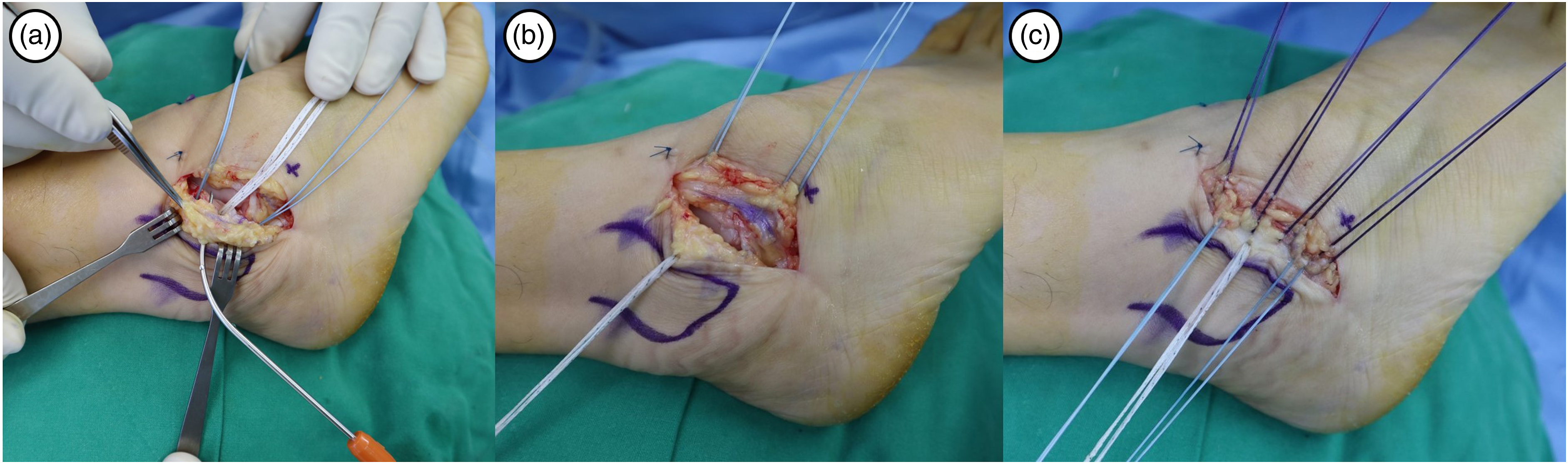
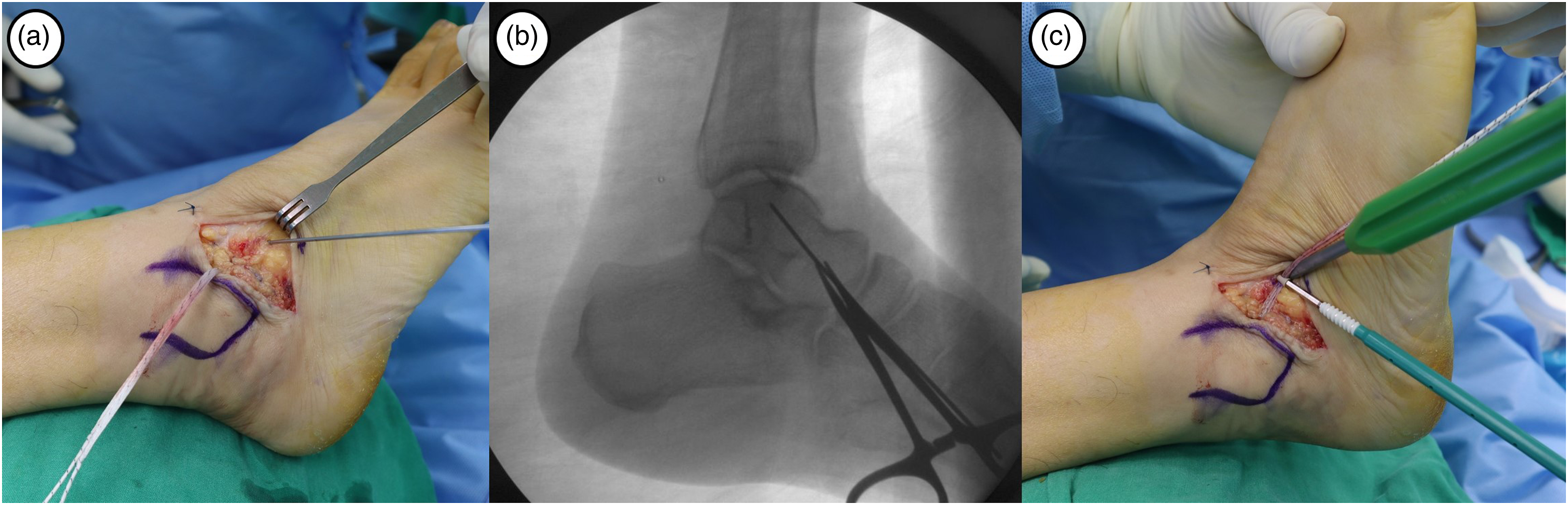
An ankle arthroscopic procedure (chondral debridement, loose body removal and synovectomy) was performed in all patients prior to the index ligament surgery. A 3 cm sized curved skin incision was made along the anteroinferior border of the lateral malleolus. After the articular capsulotomy, both quality and quantity of the anterior talofibular ligament remnant was inspected by one senior surgeon (Figure 3). The anterior talofibular ligament remnant was evaluated into two groups (repairable or not suitable to repair) based on presence of grossly normal ligamentous tissue, thickness and consistency of the remnant tissue, as well as resistance against a pulling force. For patients with poor quality of ligament remnants, intraoperative decision was made to perform an anatomical anterior talofibular ligament repair augmented with suture-tape. The condition of the calcaneofibular ligament was simply checked without repair procedure. The fibular periosteum was carefully dissected from the lateral malleolus and retracted proximally. Two 3.5 mm metallic suture anchors (Corkscrew®, Arthrex, Naples, FL, USA) were inserted into the anteroinferior border of lateral malleolus. Subsequently, a 3.5 mm SwiveLock® biocomposite suture anchor (Arthrex, Naples, FL, USA) with FiberWire® suture-tape was inserted between two metallic suture anchors (Figure 4). Suture-tape was passed outside through the fibular periosteum using suture lasso (shuttle relay). While maintaining the ankle joint in neutral flexion and slight eversion, the anterior talofibular ligament and lateral capsule are repaired with suture anchors and imbricated (overlapping) to the periosteum with horizontal mattress suture technique using 2-0 Vicryl (Figure 5). Entry point of suture-tape into the talar neck was determined with temporary guidewire fixation under fluoroscopic image. Finally, the repaired anterior talofibular ligament was augmented with suture-tape using a 4.75 mm SwiveLock® biocomposite suture anchor fixation (Figure 6). The suture-tape was tensioned while maintaining the ankle in a neutral position to avoid over-tightening. Prior to the second biocomposite anchor insertion, we marked a line on suture-tape with the ankle in a neutral position. Then, biocomposite anchor and suture-tape were inserted until a marked line reached the entrance of portal, to achieve appropriate tension. Intraoperative photographs show (a) a curved skin incision along the anteroinferior margin of the lateral malleolus, and (b) the evaluation for quality and quantity of the ATFL remnant following the articular capsulotomy. A weak remnant tissue with absence of normal ligament is confirmed. Intraoperative photographs show (a) fixation of two 3.5 mm metallic suture anchors to repair the ATFL and lateral capsule, and (b–c) fixation of FiberWire® suture-tape into the fibula using a 3.5 mm SwiveLock® biocomposite suture anchor. Intraoperative photographs show (a–b) passage of suture-tape outside of fibular periosteum using suture lasso (shuttle relay). (c) The ATFL and lateral capsule are repaired with suture anchors and imbricated (overlapping) with horizontal mattress suture technique using 2–0 Vicryl. (a) Intraoperative photograph and (b) fluoroscopic image show an entry point of suture-tape which is determined with temporary guidewire fixation. (c) The repaired ATFL is augmented with suture-tape which is fixed into the talus using a 4.75 mm SwiveLock® biocomposite suture anchor.

Patient-reported clinical outcomes measure
The assessment of clinical outcomes was performed with the Foot and Ankle Outcome Score 20 and Foot and Ankle Ability Measure. 21 Both patient-reported scoring systems were foot and ankle-specific outcome measures which had been reported to be valid, reliable, and responsive for the use with ankle ligament injury. 22 However, validation and cross-cultural adaptation of Korean version of the patient-reported scoring systems were performed only in the Foot and Ankle Outcome Score. 23
Evaluation of mechanical ankle instability
Stress radiographic examination was performed to evaluate the changes of mechanical ankle instability. The anterior drawer and varus stress radiographs were periodically performed using Telos equipment. All measurements for talar tilt angle and anterior talar translation on digital PACS image system were performed by three orthopedic surgeons, and the measurements were averaged.
Evaluation of functional ankle instability
To assess the changes of functional ankle instability, static postural control ability was periodically evaluated with the modified Romberg test 24 (single leg stance test with eyes closed). One orthopedic surgeon measured the balance retention time to when participants placed their non-stance leg on the floor with a feeling unable to keep position. This examination was repeated twice on each leg at an interval of 1 minute, and the measurements were averaged.
Results
Clinical outcomes and complications
Patient-reported clinical outcomes assessed with the foot and ankle outcome score, the foot and ankle ability measure (Wilcoxon signed-rank test).
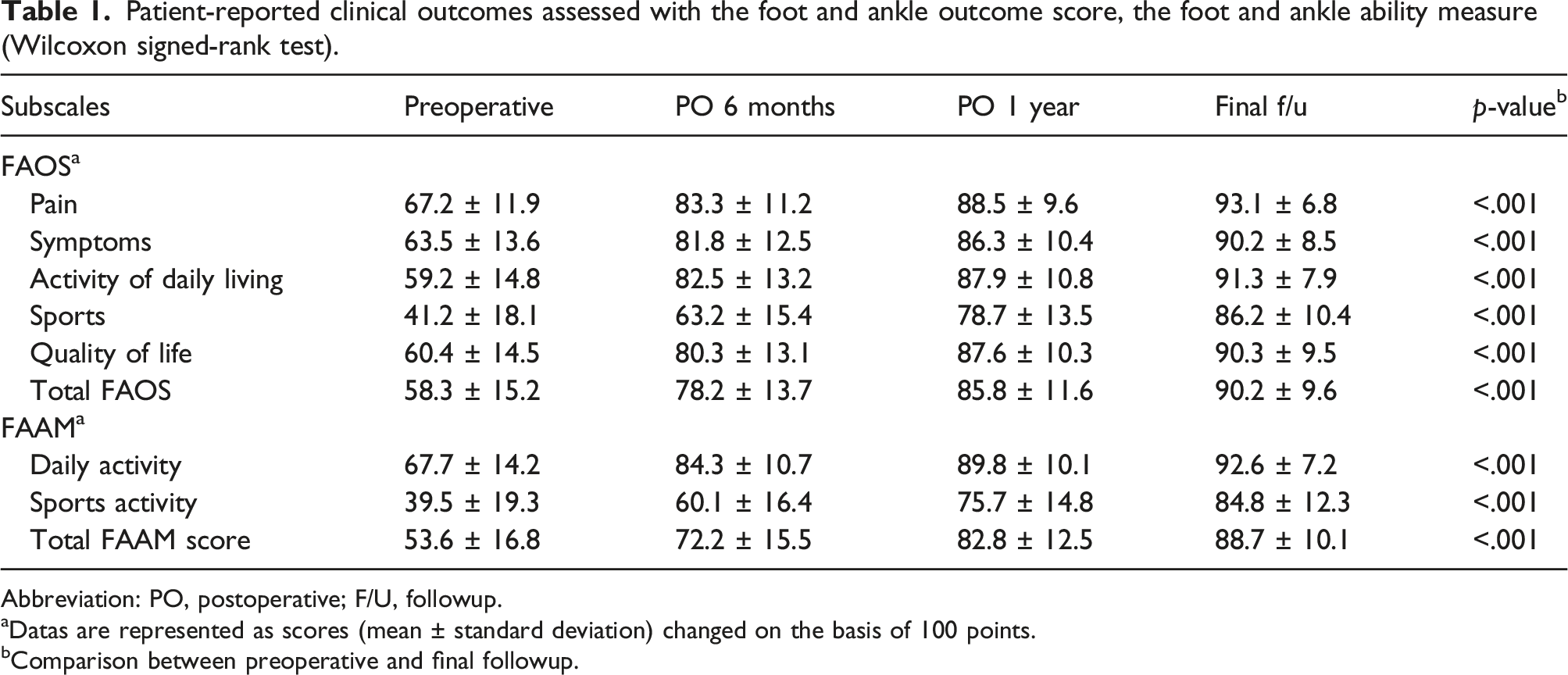
Abbreviation: PO, postoperative; F/U, followup.
Datas are represented as scores (mean ± standard deviation) changed on the basis of 100 points.
Comparison between preoperative and final followup.
Postoperative complications included three wound problems (two with superficial infection and one with focal dehiscence), two skin irritations by suture material, and two superficial peroneal nerve injuries with temporary paresthesia on foot dorsum. All wound problems were treated by antibiotics therapy and dressing. Two patients with skin irritation underwent the removal of suture materials under local anesthesia. Superficial peroneal nerve symptoms were improved postoperatively 3 and 7 months, respectively. While 13 patients sustained a sprain injury postoperatively, two (3.1%) out of the 64 patients showed a recurrence of mechanical and subjective instability. One patient underwent the lateral ligament reconstruction with auto-tendon graft 28 months postoperatively and obtained satisfactory clinical outcomes. The other patient refused a revision surgery.
Changes of mechanical ankle instability and postural control ability
The changes of mechanical ankle instability assessed with the periodic stress radiographs (Wilcoxon signed-rank test).

Abbreviation: PO, postoperative; F/U, followup.
Datas are represented as mean ± standard deviation.
Comparison between preoperative and final followup.
The changes of postural control ability assessed with the modified Romberg test (Wilcoxon signed-rank test).

Abbreviation: PO, postoperative; F/U, followup.
Datas are represented as mean ± standard deviation.
Comparison between preoperative and final followup.
Comparison between the affected and unaffected ankle
Comparison between the affected and unaffected ankle in mechanical ankle instability and postural control ability (Mann–Whitney U test).

Datas are represented as mean ± standard deviation.
Discussion
This study demonstrates that anatomic anterior talofibular ligament repair augmented with suture-tape is an effective stabilization procedure for chronic lateral ankle instability in patients with questionable remnant tissue quality for repair. Through anatomic repair of attenuated ligament and suture-tape augmentation, this combined procedure can provide enhanced mechanical stability and well-known advantages of the anatomic ligament repair (the restoration of physiologic joint kinematics, the motion preservation at the ankle and subtalar joints, technical simplicity, no morbidity associated with the graft, and a quick functional recovery).1,6,25 In addition, this procedure allows surgeons to perform the ligament augmentation without additional skin incision or advance preparation of tendon graft based on the intraoperative findings of remnant ligament tissues.
Because a basic concept of the modified Broström procedure is the anatomical ligaments repair, the status of lateral ligament remnants can be critical for histological healing and successful clinical outcomes. Strategies to address the limitations of traditional Broström repair procedure have been reported with modified techniques and new devices. As one of recently developed alternative procedures, clinical use of augmentation of primary repair with a synthetic ligament like suture-tape is in increasing trend.4,15,16,26,27 Kirk et al. 28 reported that Broström repair could provide only 50% strength of the native anterior talofibular ligament immediate postoperatively. Because the modified Broström procedure needs postoperative protection to allow the ligament tissue to mature adequately, suture-tape augmentation can play a role as an internal brace to prevent stretching out (elongation) of the repaired ligament. 18 Recent biomechanical studies demonstrated that lateral ankle ligament augmented with suture-tape had better durability compared to anatomically repaired or healthy ligaments.17–19 In addition, intraoperative supplementation of mechanical stability using suture-tape can be helpful in cases with insufficient restoration of lateral stability even after the anatomic ligament repair. Considering the controversy of cost-effectiveness in the routine use of suture-tape augmentation, we decided the necessity of suture-tape augmentation based on preoperative magnetic resonance imaging and intraoperative finding of remnant ligamentous tissues.
While the effectiveness of suture-tape augmentation for chronic lateral ankle instability has been demonstrated on various biomechanical and clinical studies,4,15,17–19,27 the issues of long-term stability and complication are still controversial. Although the standard indications are not agreed upon, short to intermediate-term clinical and functional results following suture-tape augmentation have been reported. Ramírez-Gómez et al. 16 reported that Broström-Gould procedure with suture-tape augmentation was effective in protection against the recurrence of ankle instability, and resulted in excellent clinical results at intermediate-term followup. Coetzee et al. 15 reported that modified Broström procedure augmented with suture-tape was an efficacious procedure to allow accelerated rehabilitation and to prevent recurrent instability at a mean 11.5 months of followup in 81 patients with chronic lateral ankle instability. In this study, Foot and Ankle Outcome Score and Foot and Ankle Ability Measure scores significantly improved from preoperative mean 58.3 and 53.6 points to 90.2 and 88.7 points at final followup, respectively. These results were comparable to previous studies evaluating the modified Broström procedure with suture-tape augmentation. DeVries et al. 26 reported that patients with modified Broström procedure and suture-tape augmentation showed a lower frequency of recurrent instability and reoperation compared to those with arthroscopic Broström procedure. In the current study, there were 2 cases (3.1%) of recurrence of subjective and mechanical instability and 1 case of revision surgery (lateral ligament reconstruction with auto-tendon graft) on 61.4 months of the mean followup duration. The talar tilt angle and the anterior talar translation on stress radiographs were slightly increasing at final followup compared to the early postoperative period. However, clinical outcomes including Foot and Ankle Outcome Score and Foot and Ankle Ability Measure scores remained improved over the course of time.
Cho et al. 3 reported satisfactory clinical results including a low recurrence rate (3.6%) in 28 patients with generalized ligament laxity. Another study by Cho et al. 7 demonstrated the satisfactory clinical and functional improvements after the revision modified Broström procedure with suture-tape augmentation in 30 patients with recurrent ankle instability (failure of previous ligament repair surgery). Based on these clinical studies, they suggested that modified Broström procedure augmented with suture-tape could be useful as an alternative for the patients with poor prognostic factors of the modified Broström procedure. Because there has been no published literature reporting the clinical outcomes after the modified Broström procedure with suture-tape augmentation in patients with poor quality of ligament remnants, an objective comparison with clinical and functional outcomes in the current study was not available. Further wide clinical use of modified Broström procedure with suture-tape augmentation needs to be supported by various clinical studies with high-level of evidence.
A comparison of clinical superiority between traditional modified Broström procedure and modified Broström procedure augmented with suture-tape may be a debate with large interest and needs to be investigated through the further studies. Xu et al. 5 reported that modified Broström procedure with suture-tape augmentation showed a better clinical results (Foot and Ankle Ability Measure scores) compared to the modified Broström procedure without suture-tape augmentation. In a 5 years randomized controlled trial, Porter et al. 4 reported that the Broström-Gould repair combined with ligament augmentation reconstruction system (LARS) resulted in better clinical outcomes compared to the Broström-Gould repair alone. Recent multicenter randomized controlled trial demonstrated that suture-tape augmentation allowed for earlier return (average 13.3 weeks) to preinjury level of activity than modified Broström procedure alone (average 17.5 weeks). 29 In addition, suture-tape augmentation group showed a lower complication rate (1.7%) compared to the modified Broström procedure alone group (8.5%). To the best of our knowledge, there was no published study comparing the clinical outcomes between traditional modified Broström procedure and modified Broström procedure augmented with suture-tape in patients with poor quality of ligament remnants.
The present study has a few limitations. First, the current study included no evaluation of time to return to sports at the preinjury level. Although accelerated rehabilitation and early return to previous level of activity have been suggested as an important advantage of the modified Broström procedure augmented with suture-tape,15,29 we did not consider it as one of the evaluation factors. Second, this study included no comparative analysis between the patients with and without return to previous level of sport activity. Because a consensus regarding the factors associated with failure to return to previous level of sport activity is not yet established, 30 any differences in various causing factors (insufficient restoration of postural control ability, mechanical ankle stability, peroneal strength, and proprioception) need to be evaluated and compared. The third limitation is the insufficiency of objective evidence on the changes of postural control ability. We evaluated only static postural control ability using the modified Romberg test, without an evaluation of dynamic postural control ability. Instrumental tests (star excursion balance test or multiple hop test on a force platform)31,32 may help to comprehend the effects of the modified Broström procedure augmented with suture-tape on postural control ability.
Conclusion
Anatomic anterior talofibular ligament repair augmented with suture-tape is demonstrated to be a useful surgical approach for chronic lateral ankle instability with poor quality of ligament remnants at intermediate-term followup. Through anatomic repair of attenuated ligaments and suture-tape augmentation, this combined procedure can provide reliable restoration of mechanical stability and carry the advantages of the anatomic ligament repair regardless of the remnant tissue quality. Considering a significant postural control deficit compared to the uninjured ankle at final followup, a necessity of continuous proprioceptive-oriented rehabilitation is supported. Long-term stability and safety of the suture-tape should be approached in further studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This resesarch was supported by Chungbuk National University, Korea National University Development Project (2021).