
Abstract
Purpose
Over the past 12 years, vertebral body tethering (VBT) has been gradually promoted for treating scoliosis, but there are few published studies, with only short-term follow-up. This study aimed to systematically review VBT efficacy and safety for treating scoliosis.
Methods
PubMed, Web of Science, Embase, and the Cochrane Library were searched for studies on VBT treatment of scoliosis published up to November 2021. Two researchers independently screened the literature, extracted data, and assessed the risk of bias in included studies. Data on clinical efficacy, unplanned reoperations, and complications were extracted. The meta-analysis was performed with R 4.1.0.
Results
Twenty-six studies involving 1045 patients were included in the meta-analysis. The correction rate of major curve immediately post-operation was 46.6% ± 13.8% (16%–69%) and that at final follow-up was 53.2% ± 17.9% (16%–79%). The single-arm meta-analysis results of all included studies showed that VBT was effective in general. The overall clinical success rate was 73.02% (95% confidence interval [CI]: 68.31%–78.05%). The pooled overall unplanned reoperation rate was 8.66% (95% CI: 5.53%–13.31%). The overall incidence rate of complications was 36.8% (95% CI: 23.9%–49.7%). The subgroup analysis based on follow-up time indicated that patients with follow-up time >36 months had increased clinical success rate, unplanned reoperation rate, and incidence rate of complications compared with those with <36 months’ follow-up time. The preliminary results showed that after 36 months of follow-up, only 7.17% (95% CI: 4.81%–10.55%) of patients required posterior spinal fusion (PSF) surgery and nearly 93% of patients avoided spinal fusion surgeries.
Conclusions
The current evidence from at least 3-year follow-up in different countries indicates that VBT is an effective surgical approach for treating scoliosis, with 73.88% of patients achieving clinical success. Nevertheless, about one in seven patients (15.8%) required unplanned reoperations, but only 7.17% required PSF. About half (52.17%) of the patients experienced complications. Due to the limitation of the study number and quality, our conclusion may be biased and requires verification by further studies with longer follow-up times.
Introduction
Scoliosis refers to deformity of the three-dimensional structure of the spine, which includes abnormal vertebral body arrangement in coronal, sagittal, and axial positions. Clinically, scoliosis is defined as Cobb angle ≥10° on standing anteroposterior radiographic film and can be divided into neuromuscular scoliosis, idiopathic scoliosis (IS), congenital scoliosis, and scoliosis due to other causes. 1 Scoliosis is more common in adolescents, and the incidence rate of the most common adolescent IS (AIS) is 0.47%–5.2%. 2 Scoliosis that is not treated effectively will seriously affect the patient’s body shape and lead to psychological problems such as lack of confidence, depressive tendencies, and suicidal ideation. Severe scoliosis greatly reduces the patient’s quality of life and increases the economic burden on the family and society. 3 Traditional internal fixation and spinal fusion are effective for controlling the progression of deformity in scoliosis but will reduce spinal mobility, limit growth, and may lead to spinal degeneration and other problems.4,5 Non-fusion techniques, which maintain spinal growth while controlling and correcting the spinal deformity, have been increasingly used in scoliosis treatment in recent years.
Vertebral body tethering (VBT) is a growth-modulation fusionless surgery 6 that uses an implantation system composed of vertebral body screws and a tether to attach to the vertebral body on the convex side. According to the Hueter-Volkmann law, a mechanical compressive force is applied on the convex side of the vertebral body through the tether to limit convex-side growth while the patient’s remaining growth potential will promote further concave-side growth. This will further produce a correction effect during spinal growth and development, controlling the progression of deformity and potentially avoiding spinal fusion surgery. 7 Due to its spinal non-fusion characteristics and reinvention of “old” anterior techniques, VBT again demonstrates the advantages of anterior techniques. Since its first application to IS in 2010, 8 VBT has gradually been widely used 9 and has become a hot topic in scoliosis orthopedic techniques. Different investigators have conducted studies on treating scoliosis with VBT, but most of these studies are case series reports lacking sufficient and effective randomized controlled trials and involving relatively few patients. Therefore, their results are potentially biased and imprecise. There is a lack of favorable evidence for VBT efficacy in treating scoliosis. Meta-analyses are statistical analyses combining the results of multiple studies to systematically assess a body of research and increase individual study generalizability. A meta-analysis is expected to increase the clinical sample size of VBT for treating scoliosis and improve test power.
Therefore, to understand and interpret the existing evidence, we performed a single-arm meta-analysis on VBT efficacy and safety in scoliosis treatment and systematically reviewed the progress in the clinical application of VBT in scoliosis.
Materials and methods
This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 10 The protocol was registered with PROSPERO (ID CRD42021293722). The present work is a secondary analysis based on published literature. Therefore, the requirement for ethics approval by the local institutional ethics committee was waived.
Search strategy
Two authors (X.Q and S.L) performed a computerized search independently in PubMed, Web of Science, Embase, and the Cochrane Library to identify relevant studies on VBT treatment of scoliosis published up to November 2021. Thoracoscopic anterior VBT is also known as anterior spinal growth tethering. 11 Therefore, the search terms included “vertebral body tethering”, “growth tethering”, “growth modulation”, and “scoliosis”. The search strategy combined subject headings and free words and the search syntax was determined after multiple pre-searches. The specific electronic search syntax is shown in Supplementary Material 1. We also manually searched for references cited in the included studies and relevant published systematic reviews to identify articles missed in the initial search.
Inclusion and exclusion criteria
The participants were patients who had undergone VBT for treating scoliosis, regardless of age or gender. For single-arm studies, the treatment modality in the included studies was VBT surgical treatment. For two- or multi-arm controlled studies, the experimental group comprised VBT-treated patients and there was no limitation on the control group intervention measures. The outcome measure was the number of successful clinical treatments/postoperative complications/postoperative revision surgeries. The clinical studies included were randomized controlled trials, case–control studies, cohort studies, and case series studies. The search was restricted to articles published in English.
Exclusion criteria: (1) Case report studies with <5 cases; (2) for duplicate reports for the same study, studies with shorter follow-up time, fewer patients, and earlier publication times were excluded; (3) review articles.
Data extraction
Two authors (X.Q and S.L) independently extracted data from each included study using a pre-designed data collection form and cross-checked them after data extraction was completed.
The following study characteristics were extracted from the included studies: study type, number of patients, sex, and follow-up time. Data related to VBT surgical procedures, namely mean tethering levels, upper and lowest tethering vertebra, estimated blood loss, operative time, and postoperative hospital stay, were extracted. Furthermore, the indications for VBT, i.e., scoliosis etiology and type, age at surgery, triradiate cartilage status, mean preoperative Sanders type, and mean preoperative Risser sign, were extracted.
The following outcome assessment indicators were extracted: major curve and kyphosis angle pre-operation, post-operation, and at final follow-up. The number of clinically successful patients at final follow-up was extracted. Clinical success is defined as a residual curve of <35° 12 or ≤30° 13 and no posterior spinal fusion (PSF) indicated or performed at the latest follow-up. As the studies may not have reported each patient’s Cobb angle at the final follow-up, the original number of patients who achieved clinical success at the final follow-up was extracted, as the criteria used in the studies were actually 35° or ≤30°.
The number of patients with unplanned return to the operating room (UPROR) was extracted. UPROR is defined as postoperative complications that cannot be treated effectively without using additional anesthetics. 14 Moreover, to report the incidence of various UPROR types, we extracted the number of patients who underwent conversion to PSF, tether removal, tether replacement, increased tether levels, decreased tether levels, and screw revision.
The number of patients who experienced complications was extracted. If some articles reported the total number of complication events instead of the number of patients affected, we ensured that the incidence rate of complications was not overestimated with the method of Shin et al. 15 where the incidence rate of complications is calculated using the patients with complications. The number of complication events such as curve progression without tether breakage, curve progression with tether breakage, pedicle screw loosening, overcorrection, adding-on, pulmonary complications, wound infection, and cerebrospinal fluid (CSF) leak were extracted. Furthermore, the complications were classified as grade I, II, III, IVa, IVb, or V according to the modified Clavien-Dindo-Sink complication classification system.16,17 If an UPROR cause or a complication was reported only once in all included studies, it was classified as “other”. 15
Quality assessment
The quality of the included studies was assessed using the modified methodological index for non-randomized studies (MINORS) scale. The assessment indicators were: (1) clearly stated study aim; (2) inclusion of consecutive patients; (3) prospective data collection; (4) endpoints appropriate to the study aim; (5) unbiased assessment of the study endpoint; (6) adequate follow-up period; (7) loss to follow-up rate of <5%; (8) prospective calculation of the sample size. There were a total of eight assessment indicators, each with a score of 0–2 points; 0 points indicated that it was not reported; 1 point indicated that it was reported but the information was inadequate; 2 points indicated that it was reported and adequate information was provided. 18
Statistical synthesis
After data extraction, the results of multiple independent studies of the same type were summarized and integrated using a meta-analysis. If the data format did not conform to the data statistical format or if the results of the included studies were described in descriptive statements, a systematic review of descriptive analysis was performed. The values of major curve, kyphosis angle pre-operation, post-operation, and at final follow-up were summarized and line graphs were plotted to describe the changes at the follow-up time points.
The summary of the meta-analysis results was represented using the proportion of events (the ratio of the number of events to the sample size of the included studies) with a 95% confidence interval (CI). For example, the proportion of patients achieving clinical success was estimated as the number of patients achieving clinical success divided by the number of patients who underwent VBT surgery. A meta-analysis on the clinical success rate of VBT in treating scoliosis, the pooled overall unplanned reoperation rate of patients with UPROR, the unplanned reoperation rate of patients with UPROR due to each cause, and the overall incidence rate of complications and the incidence rate of each complication was performed using the open-access software R 4.1.0. Before the meta-analysis was performed, the rates were converted using logarithmic conversion and logit, arcsine, double-arcsine, and no transformation. 19 A meta-analysis of proportions was used for the included single-arm studies. 20 The incidence of complications and the corresponding 95% CI were calculated using a meta command (analysis of single proportions), and the results were presented using forest plots.
The results of the included studies were tested for heterogeneity using the chi-square test. The magnitude of heterogeneity was analyzed with I 2 (<25% indicated no heterogeneity; 25%–50% represented low heterogeneity; 50%–75% indicated medium heterogeneity; > 75% represented high heterogeneity). 21 If p ≥ 0.1 and/or I2 ≤ 50%, indicating homogeneity among the studies, a fixed-effects model was used for pooled analysis. If p < 0.1 and/or I2 > 50%, indicating heterogeneity among the results of each study, a random-effects model was used for pooled analysis. Furthermore, subgroup analyses were performed according to the possible heterogeneity factors to investigate the source of heterogeneity. For example, a subgroup analysis was performed according to the distribution of follow-up time of the included studies.
R software was used for constructing funnel plots for the outcome measures used in ≥10 included studies to evaluate whether there was publication bias in the meta-analysis. The asymmetry of the funnel plots was statistically tested with the metabias command, i.e., potential publication bias was determined using Egger’s test, and publication bias was considered to exist when p < .05.
The metainf command was used for sensitivity analysis to assess the robustness and reliability of the pooled results of the meta-analysis. We investigated whether the exclusion of a certain study would affect the pooled results by excluding studies one at a time and assessing whether the results of the remaining studies would be significantly affected. p < .05 was considered statistically significant.
Results
Characteristics of included studies and quality assessment
A total of 984 potential studies were retrieved through PubMed (n = 274), Web of Science (n = 317), Embase (n = 383), and the Cochrane Library (n = 10). After excluding duplicates, 603 studies remained. Title and abstract screening of the 603 studies led to 544 studies being excluded. Full-text screening of the remaining 59 studies led to 33 studies being excluded. Finally, 26 studies involving 1045 patients were included in the present systematic review and meta-analysis.13,14,22–45
The studies by Samdani et al. published in 2014
46
and 2015
47
were not included, as a study from the same location but with more cases had already been included in the analysis.
41
Figure 1 shows the literature screening process and results. Table 1 shows the characteristics of the included studies and information on the VBT surgical procedures. Supplementary Table 2 and Supplementary Table 3 show the indications for VBT. Supplementary Table 4 shows the extracted data of patients who achieved clinical success and patients with UPROR. Supplementary Table 5 lists the extracted data of all reported complications. Supplementary Table 3 summarizes the key assessment results of the modified MINORS scale. Flow diagram of literature screening according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. The summarized characteristics of all 26 included studies. Note: NR: not reported.

Major curve and kyphosis angle
VBT can achieve certain deformity correction during the initial operation, control the patient’s spinal growth potential, and make the concave side grow faster than the convex side, thereby realizing continuous correction during subsequent spinal growth while controlling the progression of deformity (Figure 2). Sixteen studies reported the major curve pre- and post-operation and at final follow-up 13,14,22,23,25,28–31,34,35,37,38,41,43,45 (Figure 3). Ten studies reported kyphosis angle pre- and post-operation and at final follow-up13,14,23,28,30,34,37,38,41,45 (Figure 4). Illustration of vertebral body tethering. a) In the natural history of scoliosis, tensile stress is generated on the convex side of the spine and compressive stress is generated on the concave side, with the growth rate of the convex side > the concave side. b) In VBT, a tether applies mechanical compressive force on the convex side of the vertebral body to limit the growth of the convex side while the patient’s remaining growth potential will promote further growth of the concave side.c) During scoliosis progression, the growth rate is as follows: convex side > concave side. d) After VBT treatment for scoliosis, the growth rate is as follows: convex side < concave side. e) During the postoperative long-term follow-up after VBT treatment, the expected growth rate is as follows: convex side ≈ concave side. Major curve pre-surgery, post-surgery, and at final follow-up. Kyphosis angle at pre-surgery, post-surgery, and at final follow-up.

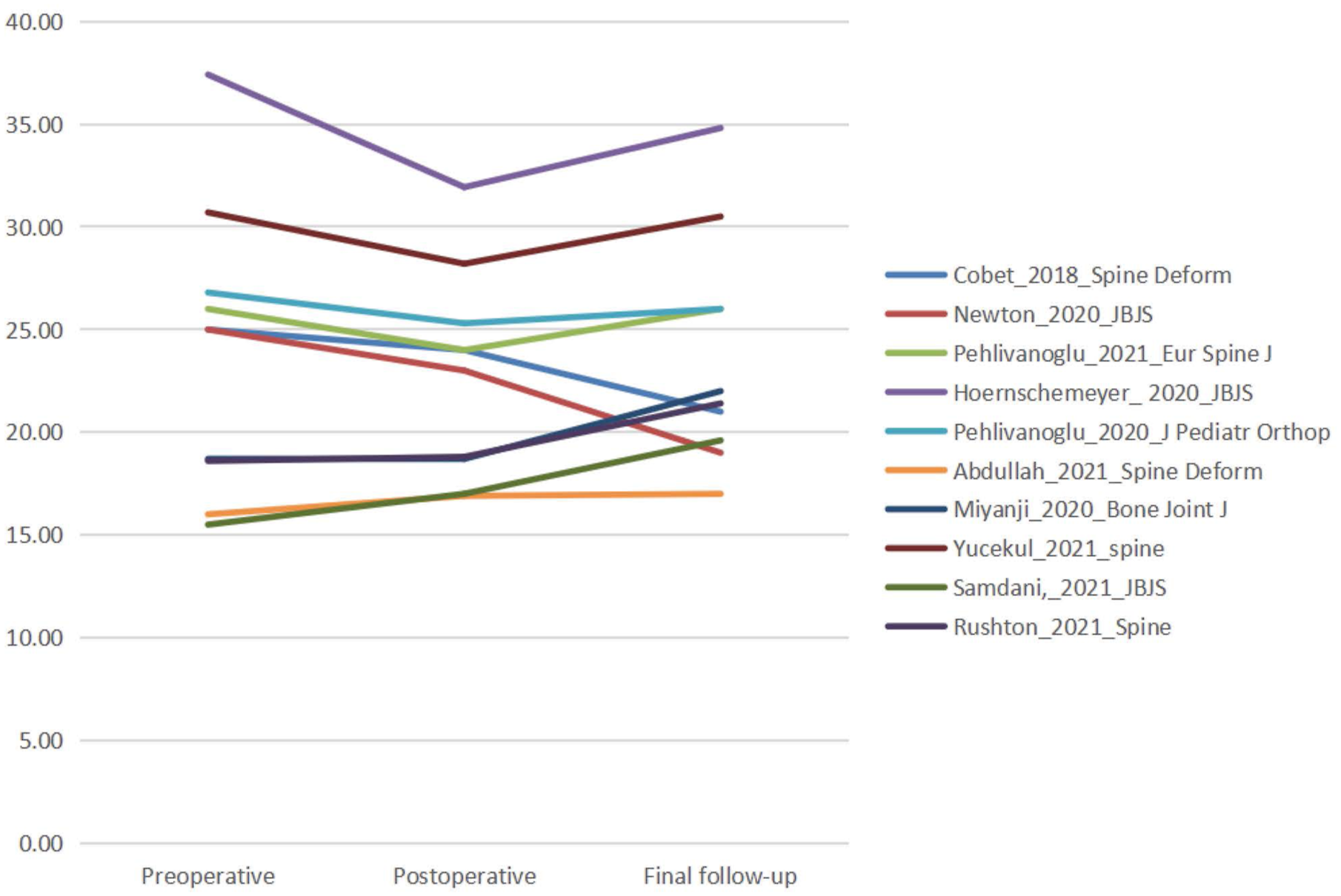
The Cobb angle of the major curve was significantly corrected from 40.06°–59.00° pre-VBT surgery to 15.90°–38.00° immediately post-operation and was 10.00°–38.00° at the final follow-up. In addition, the kyphosis angle was also significantly corrected from 15.50°–37.41° pre-operation to 16.90°–31.93° immediately post-operation and 17.00°–34.81° at the final follow-up.
Overall clinical success rate
To investigate VBT efficacy for treating scoliosis, the pooled overall clinical success rate was analyzed. Seven included studies involved 325 patients13,28,29,35,37,41,45 and 231 patients achieved a response after VBT treatment. Heterogeneity testing showed that I2 = 16% and p > 0.1. The statistical meta-analysis using the fixed-effects model showed that the overall clinical success rate was 73.02% (95% CI: 68.31%–78.05%) (Figure 5 and Table 2). Forest plot and subgroup analysis of the clinical success rate. The meta-analysis results of proportions of single-arm studies reporting clinical outcomes and reoperations of patients due to unplanned return to the operating room. #Subgroup differences were presented as P values, with statistically significant differences set as P <0.05

Pooled overall unplanned reoperation rate
The pooled overall unplanned reoperation rate was calculated to investigate further surgical treatment due to UPROR after VBT treatment. Twenty-three included studies involved 948 patients13,14,22,25–32,34–45 and 93 patients underwent unplanned reoperation after VBT surgery (I2 = 43%, p < .1). There was some heterogeneity among the studies. Using the random-effects model, the statistical meta-analysis showed a pooled overall unplanned reoperation rate of 8.66% (95% CI: 5.53%–13.31%) (Figure 6 and Table 2). Forest plot and subgroup analysis of the reoperation rate due to UPROR calculated based on the number of patients.
The incidence rates of different UPROR types were calculated. The top three were conversion to PSF (3.51%, 95% CI: 2.45%–5.01%), tether removal (2.3%, 95% CI: 1.47%–3.58%), and tether replacement (1.09%, 95% CI: 0.57%–2.08%). Table 2 shows the remaining incidence rates.
Pooled overall incidence rate of complications
The pooled overall incidence rate of complications was analyzed to investigate the safety and complications of VBT for treating scoliosis. A total of 24 studies reported complications13,14,22,24–32,34–45 and involved 1004 patients. Two hundred and eight-six patients had adverse reactions after VBT. The heterogeneity testing showed that I2 = 97%, p < 0.1, indicating heterogeneity among the studies. Using the random-effects model, the statistical meta-analysis showed that the pooled overall incidence rate of complications was 36.8% (95% CI: 23.9%–49.7%) (Figure 7 and Table 3). Forest plot and subgroup analysis of the incidence rate of complications. The meta-analysis results of proportions of single-arm studies reporting complications. #Subgroup differences were presented as P values, with statistically significant differences set as P <0.05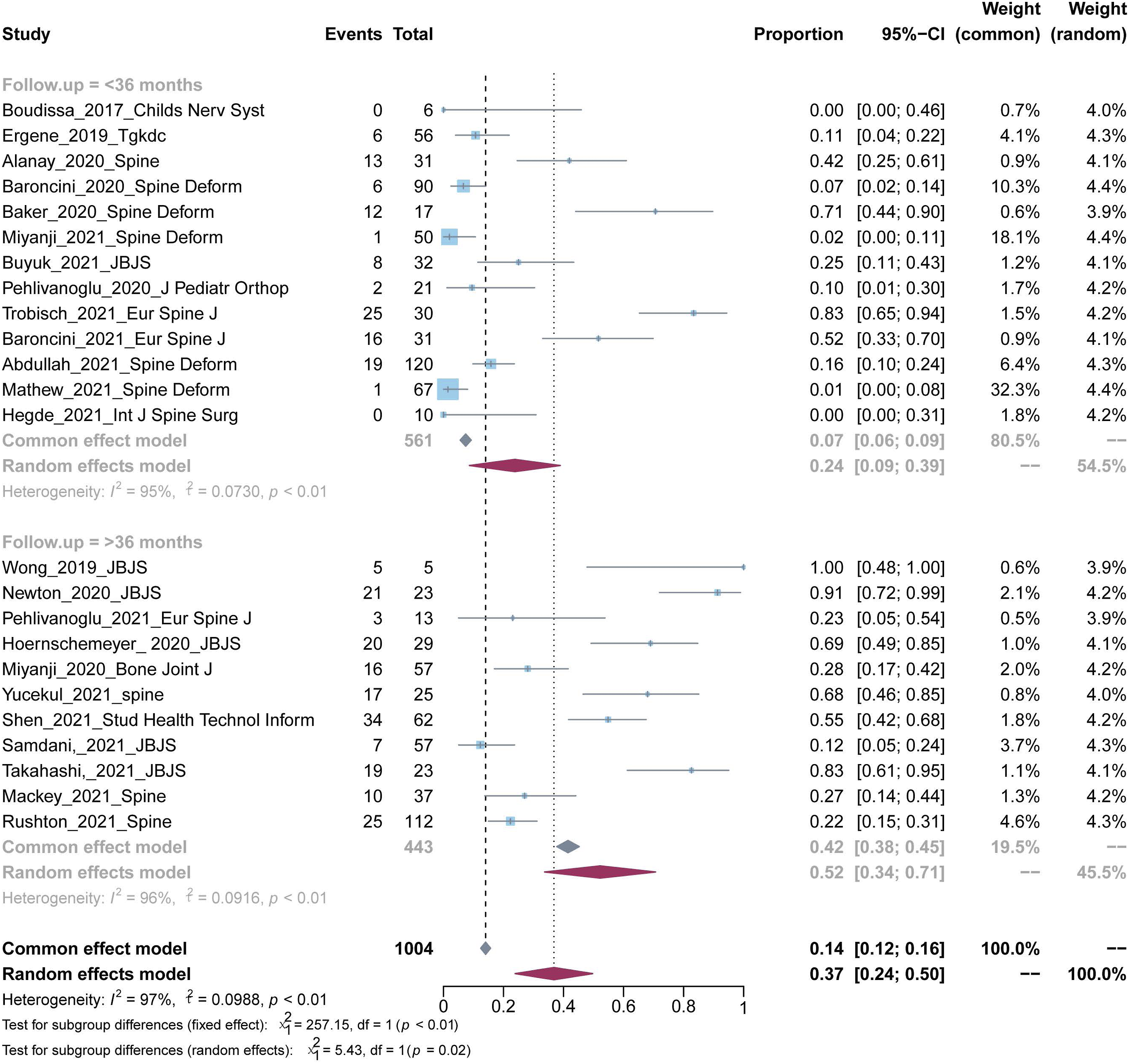
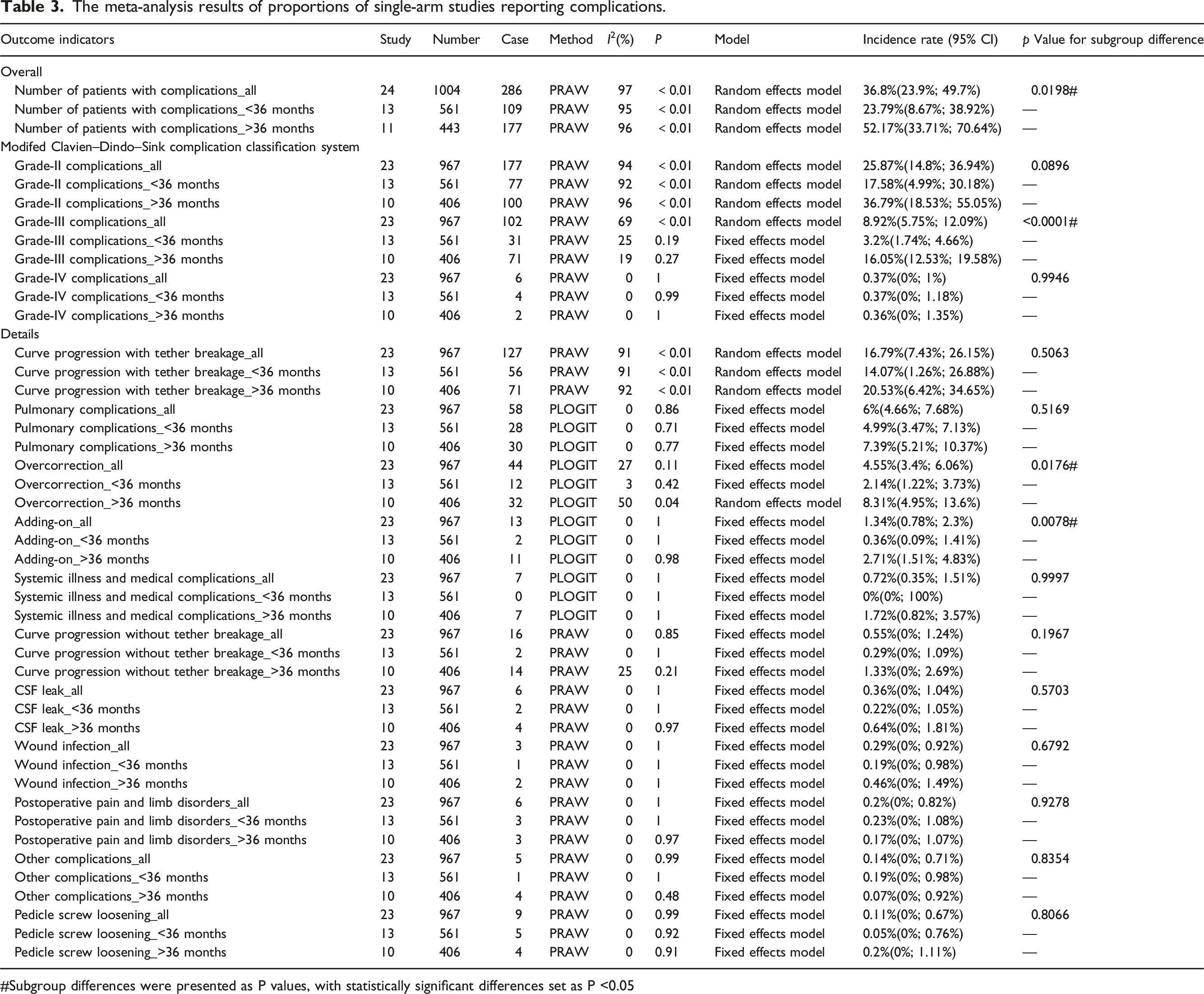
The incidence rates of grade II, III, and IVa complications were 25.87% (95% CI: 14.8%–36.94%), 8.92% (95% CI: 5.75%–12.09%), and 0.37% (95% CI: 0%–1%), respectively, and no grade I, IVb, or V complications were reported.
The incidence rates of the different complication types were calculated. The top three were curve progression with tether breakage (16.79%, 95% CI: 7.43%–26.15%), pulmonary complications (6%, 95% CI: 4.66%–7.68%), and overcorrection (4.55%, 95% CI: 3.4%–6.06%). Table 3 shows the remaining incidence rates.
Long-term (≥3-year) follow-up of outcomes
Among the 26 studies involving 1045 patients, 14 studies involving 581 patients had a mean follow-up time of <36 months.14,22–24,26,27,29,31,32,34–36,39,43 Twelve studies involving 464 patients had a mean follow-up time of >36 months.13,25,28,30,33,37,38,40–42,44,45
Clinical success rate with follow-up time >36 months
The subgroup analysis of clinical success rate showed that the pooled overall clinical success rates in patients with follow-up time <36 months and those with follow-up time >36 months were 65.93% (95% CI: 53.57%–81.14%) and 73.88% (95% CI: 68.86%–79.27%), respectively. There was no significant difference between the two subgroups (p > .05, Figure 5 and Table 2).
Unplanned reoperation rate with follow-up time >36 months
The subgroup analysis of the unplanned reoperation rate showed that the reoperation rates in patients with follow-up time <36 months and those with follow-up time >36 months were 4.55% (95% CI: 3.04%–6.76%) and 15.8% (95% CI: 12.69%–19.5%), respectively. There was a significant difference between the two subgroups (p < .05, Figure 6 and Table 2).
Based on the follow-up time, the patients could be divided into the subgroups with follow-up time <36 months and >36 months. The incidence rates of all eight UPROR types increased with the follow-up time. For example, the incidence rate of conversion to PSF increased significantly from 1.19% (95% CI: 0.53%–2.62%) to 7.17% (95% CI: 4.81%–10.55%) (p = .006). Table 2 shows the remaining incidence rates.
Incidence rate of complications with follow-up time >36 months
The subgroup analysis of the incidence rate of complications showed that the rates in patients with follow-up time <36 months and those with follow-up time >36 months were 23.79% (95% CI: 8.67%–38.92%) and 52.17% (95% CI: 33.71%–70.64%), respectively. There was a significant difference between the two subgroups (p < .05, Figure 7 and Table 3).
Based on the follow-up time, the patients could be divided into subgroups with follow-up time <36 months and >36 months. The incidence rates of nine complication types increased with the follow-up time. For example, the incidence rate of curve progression with tether breakage increased from 14.07% (95% CI: 1.26%–26.88%) to 20.53% (95% CI: 6.42%–34.65%) (p = .5063). Table 3 shows the remaining complications. Nevertheless, the incidence rates of two types of complications decreased with follow-up time: that for postoperative pain and limb disorders decreased from 0.23% (95% CI: 0%–1.08%) to 0.17% (95% CI: 0%–1.07%) (p = .9278) and that of other complications decreased from 0.19% (95% CI: 0%–0.98%) to 0.07% (95% CI: 0%–0.92%) (p = .8354).
Sensitivity analysis and publication bias
The results of sensitivity analysis and publication bias.

#Subgroup differences were presented as P values, with statistically significant differences set as P <0.05
Tests for funnel plot asymmetry should be used only when there are at least 10 studies included in the meta-analysis
†Egger’s test detects potential publication bias, and when P <0.05, it is considered that there is publication bias
The subgroup analysis of the pooled overall unplanned reoperation rate revealed that the heterogeneity test results of the two subgroups were I2 = 24% (p = .20) and I2 = 6% (p = .39), respectively, indicating no significant heterogeneity in both subgroups. The pooled result of the two subgroups was I2 = 43% (p = .02), suggesting that the different follow-up times might be a source of heterogeneity. The comparison between the two subgroups showed that p < .01, indicating a significant difference between the subgroups (Figure 6).
The subgroup analysis of the incidence rate of grade III complications revealed that the heterogeneity test results of the two subgroups were I2 = 25% (p = .19) and I2 = 19% (p = .27), respectively, indicating no significant heterogeneity in both subgroups. The pooled result of the two subgroups was I2 = 69% (p < .01), suggesting that the different follow-up times might be a source of heterogeneity. The comparison between the two subgroups showed that p < .01, indicating a significant difference between the subgroups (Supplementary Figure 1).
The subgroup analyses of the pooled overall incidence rate of complications (Figure 7), incidence rate of grade II complications (Supplementary Figure 2), and incidence rate of curve with tether breakage (Supplementary Figure 3) did not result in decreases in heterogeneity, suggesting that the different follow-up times might not be a source of heterogeneity.
Publication bias was analyzed using funnel plots. The funnel plots for overall clinical success rate, pooled overall unplanned reoperation rate, and pooled overall incidence of complications showed poor symmetry of the individual points (Supplementary Figure 4) and Egger’s test suggested that there was publication bias (Table 4).
Supplementary Figure 5, Supplementary Figure 6 and Supplementary Figure 7 shows the sensitivity analyses of the overall clinical success rate, pooled overall unplanned reoperation rate, and pooled overall incidence rate of complications. Supplementary Figure 8, Supplementary Figure 9 and Supplementary Figure 10 shows the sensitivity analyses of the incidence rates of grade II complications, grade III complications, and curve progression with tether breakage. The sensitivity analyses of the above six rates also indicated no significant changes in the pooled rates after the sequential exclusion of each study, suggesting that the meta-analysis results thereof were robust and reliable.
Discussion
Since the first report of VBT treatment of IS in 2010,
8
VBT has been used throughout the world. However, most of the current published studies did not involve a long follow-up time, and insufficient VBT case reports are followed up to the skeletal maturity stage. To the best of our knowledge, ours is the VBT report involving the largest number of cases and the longest follow-up time to date and systematically describes the clinical success rate for the first time. Moreover, we report their incidence rates in detail after categorizing the reoperation and complication types, providing the most recent reference for clinical research and application. Our study shows that: a. The application of VBT has gradually expanded from simple lumbar curve to lumbar curve, double major curve, and double-sided VBT of double AIS curves. In addition, VBT has also been extended to skeletally mature IS patients and syndromic scoliosis patients; b. the overall clinical success rate of VBT for treating scoliosis was 73.02%; c. the overall unplanned reoperation rate after VBT was 8.66%. Moreover, our preliminary results show that after >36 months of follow-up, only 7.17% of patients required PSF surgery and nearly 93% of patients avoided spinal fusion surgeries, maximizing the preservation of their spinal mobility. In addition, the incidence rates of all UPROR types increased with follow-up time; d. 36.8% of patients experienced complications after VBT. The included studies reported no severe postoperative neurological complications. Furthermore, our study shows that the incidence rates of most complications increased with follow-up time.
Therefore, we should be both optimistic and skeptical about VBT. Although it holds promise, further investigation of its true efficacy and long-term risks remains essential.
Advances in VBT for treating scoliosis
Currently, the indications for VBT remain controversial. The typical indications for VBT are skeletally immature and progressive main thoracic curve and/or main lumbar curve ≥40°. Patients with Risser sign ≤3 and Sanders type < V are considered skeletally immature. 36 Newton deemed patients with Sanders type III or IV as having “ideal” growth potential and therefore suitable for VBT, and believed that the basic principle of indications is that patients at risk of failure of brace treatment and those still at risk of deformity progression after brace treatment are suitable for VBT. 48 The retrospective study of Samdani et al. 47 supported this view.
Previously, VBT was mostly used for main thoracic curve, but lumbar curve was not a contraindication for VBT, and the application of VBT in lumbar curve27,35–37,39,43–45 and double major curve was subsequently reported.24,29,30,35,37,45 In terms of surgical approach, the thoracic approach with a thoracoscope is commonly used for VBT. Typically, T4 to L2 can be observed under the thoracoscope. However, T12 can only be handled via a minimally invasive open retroperitoneal approach due to occlusion of the diaphragm. Moreover, lumbar tethering uses a separate retroperitoneal approach and is performed under direct vision. 49
Skeletal maturity was once considered a contraindication for VBT in IS patients, 37 but Hegde et al. 43 reported 10 cases of VBT in skeletally mature patients whose mean Risser sign and Sanders type were 4.2 ± 0.6 and 7.2 ± 0.6, respectively. Patients with different Sanders types had different scoliosis angle changes after VBT treatment; patients with Sanders type II experienced more overcorrection, and patients with Sanders types III, IV, and V had less risk of mechanical complications. 26 In addition, VBT is not absolutely contraindicated for non-IS patients.12,13,50 However, the application of VBT in patients with syndromic scoliosis should be carefully evaluated, as syndromic scoliosis may lead to relatively unexpected adverse outcomes due to its primary disease.
Clinical efficacy
Our results show that after VBT treatment, the Cobb angle of the major curve was significantly corrected, with a correction rate of 46.6% ± 13.8% (16%–69%) immediately post-surgery and was 53.2% ± 17.9% (16%–79%) at final follow-up.
VBT limits convex-side growth by applying a mechanical compressive force on the convex side of the vertebral body through a tether, while the remaining growth potential of patients will promote further growth of the concave side, thereby reversing the vicious cycle that generates asymmetrical loads leading to vertebral wedging and scoliosis progression. 51 Due to the existence of the chondral growth force response curve (CGFRC), epiphyseal growth plate growth stimulation will reach a threshold under the action of tension and compression forces, beyond which epiphyseal growth plate growth will be inhibited. Therefore, the poor correction or even deterioration after VBT treatment may be attributed to the existence of the CGFRC. 52 Appropriate VBT may result in ineffective correction or overcorrection of scoliosis. To implement an effective growth regulation intervention, it is necessary to understand the relationship between mechanical tension and compression and the resultant change in vertebral body growth behavior to achieve the desired corrective effect. Further molecular biology and biomechanical research can help define this relationship accurately and the surgical decision on VBT can be continuously optimized, patients with appropriate initial scoliosis angle can be selected, and a relatively appropriate initial scoliosis correction rate can be achieved immediately after operation to improve the orthopedic capacity of VBT. 53
Our results show that through the statistical meta-analysis, the overall clinical success rate of the seven included studies was 73.02%, indicating a relatively high clinical effective rate of VBT. Newton et al. 28 recruited 23 patients in the VBT cohort and 26 patients in the PSF cohort to compare the efficacy between VBT and PSF. All patients achieved deformity correction after VBT or PSF, but the PSF group had a better 2-year correction effect; there was no difference in the postoperative follow-up results between the two groups. Nevertheless, the VBT group had a lower correction rate (43%) compared with the PSF group (69%) and a higher number of revisions, but most patients eventually avoided PSF after VBT treatment. Qiu et al. 54 reviewed the data of 62 patients who underwent PSF and 20 patients who underwent VBT from a multicenter registry. The correction rates in the VBT and PSF groups were 59% and 43%, respectively, and there were no significant differences in demographic, clinical, and radiographic data and health-related quality of life between the two groups. Pehlivanoglu et al. 33 retrospectively analyzed the data of 21 patients who underwent VBT and 22 patients who underwent PSF. The patients who underwent VBT had higher SRS-22 (Scoliosis Research Society-22) and SF-36 (Short form 36) scores and better quality of life and satisfaction after surgery compared with the patients who underwent PSF.
Reoperation due to UPROR
Our results show that the overall unplanned reoperation rate due to UPROR was 8.66% (95% CI: 5.53%–13.31%). The top three unplanned reoperations were conversion to PSF (3.51%, 95% CI: 2.45%–5.01%), tether removal (2.3%, 95% CI: 1.47%–3.58%), and tether replacement (1.09%, 95% CI: 0.57%–2.08%). Revision surgeries for VBT mainly included tether removal due to overcorrection, PSF due to scoliosis progression, tether replacement due to tether breakage, and lumbar tether addition due to adding-on. A meta-analysis of magnetically controlled growing rods (MCGR) showed that MCGR had an overall reoperation rate of about 46% (95% CI: 0.35%–0.57%) when the follow-up time was >2 years. 55 In contrast, conventional growing rod techniques require an average of 2–4 additional surgeries per patient.56,57 Therefore, the preliminary results of the present meta-analysis show that VBT has the advantage of reducing the multiple reoperation rate. However, further comparative studies in the future are necessary for comparing the unplanned reoperation rate between VBT and other scoliosis orthopedic surgeries such as PSF and MCGR. 15
Subgroup analyses of the overall unplanned reoperation rate showed that only 4.55% (95% CI: 3.04%–6.76%) of patients with follow-up time <36 months and 15.8% (95% CI: 12.69%–19.5%) of patients with follow-up time >36 months underwent unplanned reoperations. This means that the unplanned reoperation rate gradually increased with follow-up time. In addition, the unplanned reoperation rate due to each cause increased with follow-up time. The above results suggest that as the follow-up time increased, the patients’ growth and development changed, the fixation effect of internal fixation devices gradually decreased, and the unplanned reoperation rate and revision surgeries increased. Our preliminary results show that after follow-up > 36 months, only 7.17% (95% CI: 4.81%–10.55%) of patients required PSF surgery and nearly 93% of patients avoided spinal fusion surgeries, maximizing preservation of their spinal mobility. Further studies should be performed on the follow-up results from the time of VBT surgery up to when the patients are skeletally mature, or even longer, and on the poor outcome after VBT that leads to the eventual conversion to PSF. 43
Complications
In the present study, current evidence from at least 3 years of follow-up in different countries suggests that VBT is an effective technique for correcting spinal deformity, maintaining spinal mobility, and promoting spinal growth. Nevertheless, more than one-third of patients (36.8%, 95% CI: 23.9%–49.7%) experienced complications. In addition, subgroup analyses showed that 23.79% (95% CI: 8.67%–38.92%) of patients with follow-up time <36 months and 52.17% (95% CI: 33.71%–70.64%) of patients with follow-up time >36 months experienced complications. Preliminary studies showed that the incidence rate of complications increased with follow-up time.
This study shows that the top three complications were curve progression with tether breakage (16.79%, 95% CI: 7.43%–26.15%), pulmonary complications (6%, 95% CI: 4.66%–7.68%), and overcorrection (4.55%, 95% CI: 3.4%–6.06%). Our findings are consistent with that in the literature. The complications of VBT mainly include: implant-related complications such as tether breakage, overcorrection, screw loosening, for example, overcorrection caused by excessive tension applied to the apical cone region by the tether during surgery; and thoracoscopic surgical approach-related complications such as wound infection, hemopneumothorax, chylothorax, atelectasis, pneumonia, pleural effusion, for example, lung parenchymal and segmental vascular injuries during thoracoscopic surgery. 48
Tether breakages, which are the most common complications, are indicated by ≥6° increase in angulation between adjacent screws on any two postoperative radiographs. 12 Newton et al. 12 have opined that compared with previous radiographic films, the significantly increased angulation between two adjacent screws represents possible tether breakage but is not necessarily an indication that VBT surgery will fail. This could be due to the fact that VBT yields reliable overall deformity correction for IS and revision surgeries are not required. In addition, Newton et al. 12 have suggested that 1–2 years after VBT is a critical time point for tether breakage. Hoernschemeyer et al. 13 found that among 14 patients with tether breakage, 50% achieved clinical success, 36% experienced clinical failure without any additional surgery, and only 14% underwent PSF. It is worth noting, however, that we usually confirm whether a tether breakage has occurred by measuring X-ray images, which may not be remarkably accurate. Partial tether breakages are identified with certainty during reoperation, but not all patients with tether breakages require reoperation. Therefore, the true incidence of tether breakage is unknown, and our study may underestimate the true incidence of it.
No study included in this article reported severe postoperative neurological complications. Nonetheless, Abdullah et al. 14 and Rushton et al. 45 reported postoperative CSF leak and Shen and Parent 58 reported a case of iatrogenic durotomy with symptomatic Chiari-like deformity in a skeletally immature patient with AIS after VBT. Newton et al. 28 reported one case of postoperative Horner syndrome. Given that the first report of VBT in a patient was in 2010, 8 it has only been used in clinical practice for less than 12 years. For patients with different etiologies, different spinal growth and development potentials, 26 and different Lenke types of scoliosis, the incidence of unplanned reoperations and complications requires further investigation to better guide effective treatment of scoliosis.
The study limitations are: (1) As we included few high-quality articles and few articles with high-level evidence in this study, only case series reports and case–control studies were included for systematic review, and none were a randomized controlled trial. Therefore, the current level of evidence remains relatively low-quality. (2) Although our study included the largest number of patients to date and involved at least 3 years of follow-up, the sample size is nevertheless small. The lack of assessment of long-term efficacy in each study, the varying follow-up durations, and the small sample sizes included in most studies with long follow-up time weakened the strength of evidence for long-term efficacy and safety assessment in this study. However, the sensitivity analysis results indicated that the analytical results of this study were robust. In addition, the inconsistent follow-up time in studies from different hospitals may lead to heterogeneity. Therefore, we conducted subgroup analyses on the length of follow-up time to reduce this effect. (3) The included studies did not have uniform standards for clinically successful treatment; the differences in learning curve and knowledge of surgical techniques between different hospitals led to a difference in the incidence rate of complications. Therefore, measurement bias was objective and heterogeneity was inevitable. (4) Different major curve types may lead to different treatment outcomes of VBT. However, because the included literature did not conduct further analysis after distinguishing patients according to curve types, we could not conduct subgroup analysis according to major curve types.
Conclusion
The present study provides the most recent evidence on the clinical efficacy, unplanned reoperations, and complications of VBT for treating scoliosis. The meta-analysis results of studies with follow-up > 3 years indicated that VBT is an effective surgical approach for scoliosis, promoting spinal growth, and providing a good orthopedic effect while preserving spinal mobility. VBT has a high clinical effective rate (73.88%); only 7.17% of patients required PSF surgery after a follow-up of 36 months. At the same time, preliminary studies showed that as the follow-up time increased to >36 months, the unplanned reoperation rate increased to 15.8% and the incidence rate of complications increased to 52.17%.
Thus, the higher unplanned reoperation rate and incidence rate of complications suggest the need for an improved implant and patient inclusion criteria, and surgeons must still be aware of the substantial risk of complications and unplanned reoperation. Long-term follow-up is still critical to determine the actual effectiveness of VBT, but the quality of the included studies was not comprehensive enough to accurately assess the actual effectiveness of VBT. Our conclusions require verification by high-quality randomized controlled trials. Further studies should be conducted in multiple centers and include comprehensive, long-term, and dynamic follow-up of patients from VBT surgery to final skeletal maturity.
Supplemental Material
Supplemental Material - Minimum 3-year experience with vertebral body tethering for treating scoliosis: A systematic review and single-arm meta-analysis
Supplemental Material for Minimum 3-year experience with vertebral body tethering for treating scoliosis: A systematic review and single-arm meta-analysis for Feng Zhu, Xin Qiu, Shunan Liu, and Kenneth Man-Chee Cheung by Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by Shenzhen Fundamental Research Program, China (No. JCYJ20180306173518936), Sanming Project of Medicine in Shenzhen, China (No. SZSM201612055) and HKU-SZH Fund for Shenzhen Key Medical Discipline(No. SZXK2020084).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.