
Abstract
Background
Mechanical failure of the endoprostheses is a concern in paediatric patients with primary bone sarcoma. Their long-term results are variable in the Asian population, thus we aim to investigate the outcome by assessing the mechanical failure, its risk factors and the functional results.
Methods
We retrospectively reviewed 38 paediatric patients (mean 13.29, range 6–18) with primary bone sarcoma of lower extremity undergone chemotherapy and limb salvage surgery with tumor endoprosthesis between 2003 and 2016. All hospital notes were reviewed for any type of failures. Risk factors for implant loosening like stem size, remaining bone length, stem length, extracortical bone bridge ingrowth (EBBI), the ratio of resected bone length to whole bone length, bone stem ratio and custom-made versus modular were analyzed. The limb function was recorded by Musculoskeletal Tumor Society (MSTS) score. Median follow-up time was 7.42 years (3.0–15.4 years) and minimum follow-up for surviving patients was 2 years.
Results
Endoprosthesis survivorship, according to Kaplan Meier was 94.7%, 85.4% and 66.2% at 2, 5 and 10 years respectively. Type II failure occurred in three patients (7.9%). Type III failure occurred in four patients (10.5%). Type IV failure occured in two patients (5.2%). Only EBBI independently predicted implant loosening (p = .007). Risk factors like stem size, remaining bone length, stem length, the ratio of resected bone length to whole bone length and custom-made versus modular were not associated with increase in implant loosening (p > .05). The mean stem size was 9.41 mm in asymptomatic group, comparable with 9.22 mm in the failure group (p = .79). The MSTS score was 29.62.
Conclusions
Our data suggests that paediatric Chinese patients with small body built had good and excellent mid-term results in implant survival and limb function respectively. EBBI is important in preventing loosening in tumor endoprosthesis. In contrast to the reported higher failure risk with stem size <12 mm, we found no increased loosening rate with smaller stem size endoprosthesis.
Level of evidence
Class III
Introduction
Osteosarcoma is the most common primary malignant bone tumor of children and adolescents. Chemotherapy and tumor resection with negative margins is important in achieving long-term survival in patients with non-metastatic high-grade osteosarcoma. 1 With the advent of chemotherapy, imaging modalities, and surgical techniques, outcomes in paediatric osteosarcoma have greatly improved over the past few decades, with the reported 5-year survival ranging from 50 to 75%.2–5 Orthopaedic oncology surgeons can avoid amputation and perform limb-salvage surgery to retain limb functions.6–8
Endoprosthetic reconstruction is the mainstay of treatment following the resection of bone sarcoma in limb-salvage surgery. As it is a non-biological bone reconstruction, endoprosthetic related complications are expected to increase in time with surviving patients. In a study of 776 bone tumor patients who underwent endoprosthetic reconstruction, 34% of patients had revision surgery due to mechanical failure, infection, and local tumor recurrence at a mean follow-up of 15 years. Implant survival at 10 years was 75%, with mechanical failure as the endpoint. 9 The long-term survivors with endoprostheses may have to undergo an average of 2.7 further operations at the mean follow-up of 29.4 years 10 The high failure rate seen with the endoprosthesis is thought to be caused by the younger age of the sarcoma patients and also high stresses exerted on the components and at the bone-implant interface. Risk factors like smaller stem size, higher bone to stem ratio, and a greater percentage of bone resected were reported.11,12
It lacks large studies reporting long-term results in Asian Paediatric and adolescent patient groups. Given the relatively smaller body-built in Asians 13 and a higher percentage of bone resection for a same-sized tumor compared with that of the Caucasian, it is debatable if the endoprostheses lead to a higher risk of aseptic loosening or mechanical failure. 14
Our institution has been using endoprostheses for limb reconstruction following resections of paediatric and adolescent bone sarcoma since 2003. We reported our early results in 2010. 15 At a mean follow-up of 42.8 months, the endoprostheses had no mechanical failure or aseptic loosening that required revision surgery. The mean functional MSTS score in primary bone sarcoma was 28 (out of 30). 15 This study is a continuation of our previous work. The aims were to report (1) the survival of the endoprostheses, (2) the primary outcome as the mode of failure of the endoprostheses, and (3) the secondary outcome by analyzing the factors leading to the mechanical failure.
Patients and methods
The demographic information of the study.

Osteosarcoma (OS); Parosteal sarcoma (PS); Ewings (ES); Joint sparing (JS); Joint growing (JG); Joint saving growing (JSG); Modular (MD), cemented (C); Cementless (Cl), Hydroxyapatite coated (H); Porous (P).
There were 36 osteosarcomas, 1 Ewing sarcoma, and one parosteal osteosarcoma. Locations of the sarcoma were distal femur (N = 24) and proximal tibia (N = 14). Twenty-one endoprostheses were custom-made and 17 were modular. Custom-made endoprostheses were used if the size of the modular system did not match with the bone defect following tumor resection. An extendable endoprosthesis was required to correct the anticipated leg shortening (>2 cm) after reaching skeletal maturity, or a joint-saving tumor resection was performed. Patients were selected for the joint-saving surgery if (1) there was no epiphyseal tumor involvement on MRI (T1-weighted coronal view); (2) a residual epiphyseal bone of at least 1 cm was available to allow adequate fixation to the endoprosthesis; and (3) tumor responded to neoadjuvant chemotherapy by showing no evidence of tumor progression on MRI. 16 The custom-made endoprostheses were six joint-saving, six extendable, and nine extendable joint-saving implants. The custom extendable and modular prostheses were rotating hinged design at the knee articulation. Table 1 shows the demographic information of all patients and endoprostheses.
The endoprostheses had either Hydroxyapatite (HA)-coated or porous collars at the bone-implant junction so to facilitate extracortical bone bridge formation (EBBI) for better implant longevity Figure 1(a) and (b). Normal periosteum was preserved if possible to cover the collars, and cancellous bone graft obtained during endoprosthetic joint replacement was added to the bone-implant junction. These two biologic augments were added to enhance the EBBI. Cementless hydroxyapatite (HA) coated stems were used instead of cemented stems if the stem size was smaller than 8 mm in diameter Figure 1(a). The HA-coated extracortical plate was added to the bone-implant junction of a custom-made endoprosthesis for epiphyseal fixation or if the length of the cemented stem was shorter than 120 mm. Figure 1(c) and (d). A–D. The photographs show (a) the cementless femur stem (*) of a custom extendable joint-saving implant with Hydroxyapatite (HA)-collar (yellow arrow); (b) the porous surface (yellow arrow) of the cemented stem of a distal femur modular implant; (c) HA-coated extracortical plate (yellow arrow) at the proximal implant junction of a custom extendable joint-saving implant and (d) HA-coated extracortical plate (yellow arrows) at the distal epiphyseal junction of a custom extendable joint-saving implant.
For patients with proximal tibia bone sarcomas, medial gastrocnemius muscle flaps were performed to cover the endoprostheses and reconstruct the knee extensor mechanism with the remaining patellar tendons.
Postoperatively, the patients had early physiotherapy for leg mobilization. They were allowed to walk with a protective knee-ankle-foot hinged brace and partial weight-bearing for 4 weeks and then full weight-bearing if a joint-sparing surgery was performed or a cementless stem was used. Immediate weight-bearing walking was allowed if a cemented stem was used. Patients with distal femur endoprosthetic reconstruction were allowed to mobilize their knees from 0° to 90° for 4 weeks and then free knee range of motion. Patients with proximal tibia endoprosthetic reconstruction underwent gradual knee flexion mobilization to 90° in 8 weeks to protect the knee extensor mechanism reconstruction. All patients wore the protective brace for a total of 12 weeks. Chemotherapy was resumed in patients with high-grade osteosarcoma or Ewing sarcoma 2 weeks post-operatively. All patients were followed up at postoperative 1 month, every 3 months for the first 2 years, every 6 months until 5 years, and then annually. The duration of follow up was counted from the date of surgery to the date of the last clinical evaluation. Overall median follow-up time was 7.42 years (3.0 - 15.4 years), and the minimum follow-up for surviving patients was 2 years. Five of the patients died due to disease progression from the primary bone sarcoma. Thirty-three children were alive at the final follow-up.
Primary outcome of the complications after limb salvage surgery was defined according to Henderson’s classification
17
: Type 1, soft tissue failure; Type 2, aseptic loosening; Type 3, structural failure; Type 4, infection and Type 5 tumor progression. Limb function was measured using MSTS scores.
18
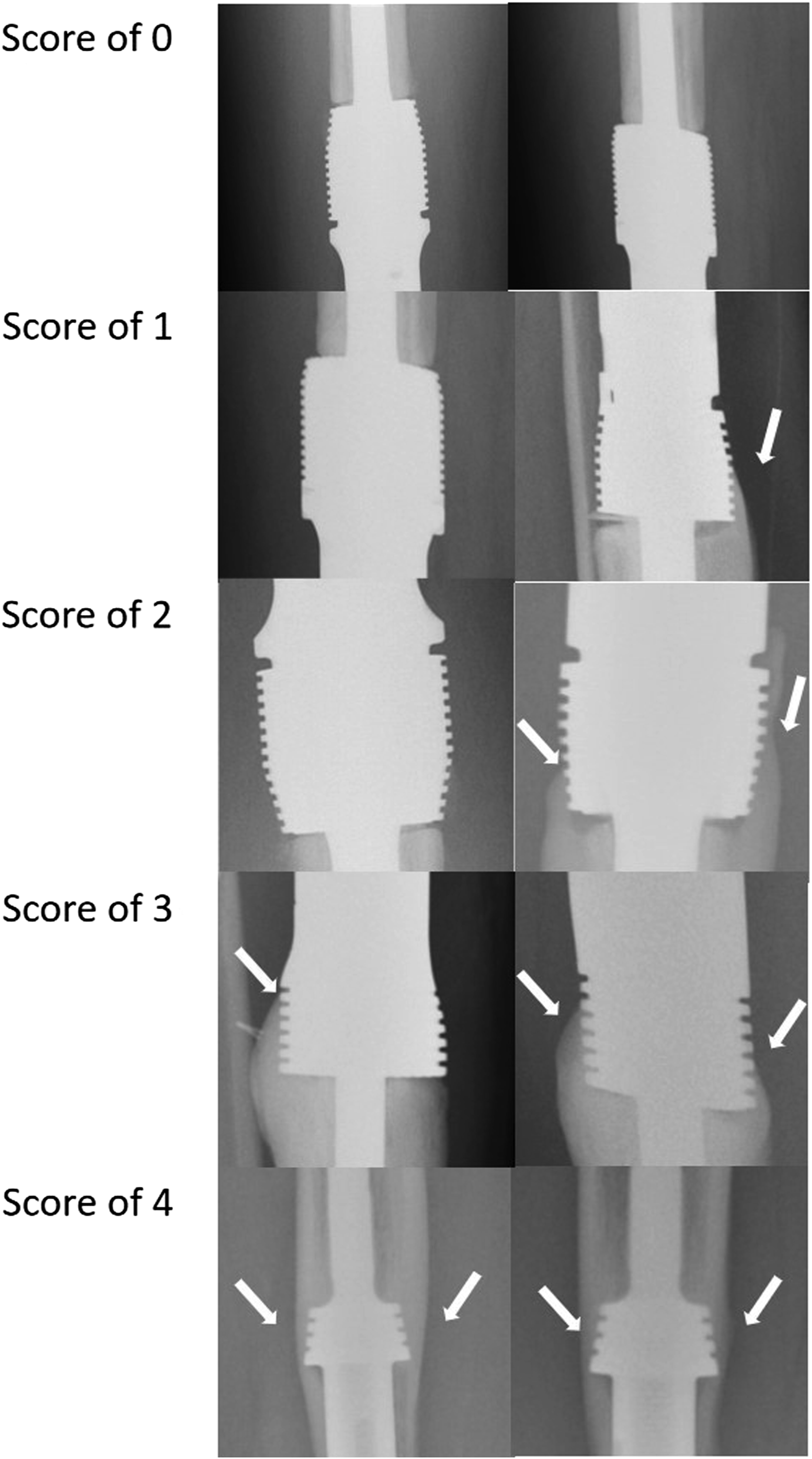
Clinical examination and plain radiographs of the operated sites were done at each visit. We investigated the secondary outcome, the risk factors leading to Type 2 failure, by measuring the stem size, remaining bone length, stem length, bone-stem ratio, Extracortical Bone Bridge Ingrowth (EBBI), and the ratio of the resected bone length (RBL) to the entire bone length (EBL) Figure 2(a) and (b). All the above parameters were measured by post operative imaging within 3 = months operatively except for entire bone length which was taken as the imaging done just before the operation and EBBI was measured according to the radiograph taken at the last follow up. Bone stem ratio was the ratio between the diaphysis (measured at the bone implant junction) and the stem size. The same orthopaedic surgeon performed all radiographic measurements. The stem size was recorded according to the diameter of the used endoprostheses. An EBBI score of 0–four was used to quantify the bone growth on the HA-coated or porous collars at bone-implant junctions Figure 3.
19
An EBBI score of 1 was assigned if bone growth was present at one of four regions at the bone-implant junction on the anteroposterior and lateral views of the plain radiographs. Scores 3 to 4 were categorized into Group A, and scores 0 to two into the Group B. Bone stem ratio was attained by measuring bone diaphyseal width and the diameter of the stem.
11
A, B. The risk factors for the implant failure were investigated by measuring on the postoperative plain radiographs of the implant the parameters that include (a) stem size (*), bone (#)-stem (*) ratio, Extracortical bone bridge ingrowth (arrowhead), and (b) and the ratio of the resected bone length (RBL) to the entire bone length (EBL). Shows the EBBI score of 0–4. By assessing the osseointegration at the bone-implant junction, an EBBI score of 1 was assigned if bone growth (arrows) was present at one of four regions at the bone-implant junction on the anteroposterior and lateral views of the plain radiographs.
Endoprosthetic survivorship was calculated with Kaplan-Meier analysis starting from the date of surgery, while any modes of failure were classified as the endpoint. Cases without failure were censored at either patient’s death or the date of the last assessment. T-test was used to compare any differences between the means of parameters of the surviving and failure group. A p-value of <.05 was considered statistically significant in all tests performed with SPSS software (Version 23).
Results
Kaplan-Meier statistics showed an overall 86.6% mean implant survival of 14.0 years (95% CI 12.6–15.3 years) for endoprosthesis surviving without Type II failure (aseptic loosening). Two-year, 5-year, and 10-year survival rate was 97.3%, 91.2%, and 86.6%, respectively. There was an overall 66.2% mean survival of 12.3 years (95% CI 10.5–14.0 years) for endoprosthesis that did not need revision for any reason. Two-year, 5-year, and 10-year survival rate for the latter group was 94.7%, 85.4%, and 66.2%, respectively (Figure 4). A mean MSTS score was 29.6 (28–30) out of 30 at the last follow up of the patients. At the last follow-up, no complications were noted for 29 (76.3%) out of the 38 patients. For the nine cases with complications, 3 (7.9%) were Type 2 failure, 4 (10.5%) were Type 3 failure, and 2 (5.2%) was Type 4 failure. Of the 38 patients, five patients died with four due to the progression of the disease with distant metastasis and one due to uncontrollable gastrointestinal bleeding (Table 2). Shows Kaplan Meier curve with revision as endpoint. Censoring for patients alive without event occurrence at last follow up. Results.

Primary outcome
For the 3 cases with Type 2 failure, one patient underwent revision of the prosthesis and had a functional and painless limb after that. Time to revision for this case was 2 years and a cemented hydroxyapatite coated implant was used. For the other two patients, there was occasional mild mechanical pain. Plain radiographs did not show a further progression of loosening during his follow up. No loosening was noted at the epiphyseal fixation in all joint-saving or extendable, joint-saving endoprostheses.
For the 4 cases with Type 3 failure, including two stem fractures, one bushing wear, and one anti-rotation peg dislodgement, all the patients underwent revision surgery with a good functional outcome. Mean time to revision for this case was 9 years and 11 months and 3 cases used cemented hydroxyapatite coated implant whereas the remaining case was a cementless hydroxyapatite coated implant. For the 2 cases with type 4 failure, no major prosthesis revision was done. Superficial debridement was done for one case whose infection did not extend into the prosthesis, and a good outcome was noted postoperatively with a course of antibiotics. For the other case, an above-knee amputation was needed due to uncontrolled infection.
Secondary outcome
There was no statistical difference between the non-failure group and the failure group in terms of stem size, remaining bone length, stem length, bone-stem ratio and the ratio of RBL to EBL. Radiological results of EBBI showed statistical difference wbetween the failure and the non-failure group (mean; 3.59 vs 1.33, p = .0007). (Table 2)
Extracortical bone bridge ingrowth score was also compared between the porous group and hydroxyapatite coated surface group and also between cemented and cementless stem with no difference noted in both arms.
Discussion
Endoprosthetic reconstruction is the mainstay of treatment following the resection of bone sarcoma in limb-salvage surgery. In our centre, most of our patients present in early stage and more than 90% of them undergo limb sparing surgery with our paradigm shifting from biological reconstruction to prosthetic reconstruction since 2003. This study echoes our early results suggesting young patients with bone sarcoma could achieve excellent limb function with minimal mechanical complications. 16
Comparison of previous study with our study (DF: distal femur; PF: proximal femur; WF: whole femur; FD: femoral diaphysis; PT: proximal tibia; Tib: tibia; PH: proximal humerus). This table denotes the age, number of cases, site, follow up duration, types of failure and survivorship of implant not needing any kind of revision.

Extracortical bone bridge ingrowth
Osseointegration at the bone-implant junction is essential for a stable biomechanical environment and also improves longevity of the stem fixation.
20
Thus, survival of the endoprosthesis was correlated with the radiological scores of EBBI. It was found that there was a statistically significant difference between Group A (scoring 3 or 4) and Group B (scoring 0 to 2). This segregation was made because 50% of bone growth was needed for adequate stress distribution at the implant collar and bone growth. In the original study, 25% was suggested as just adequate ex vivo, but in physiological conditions, there would be further factors affecting the stress such as soft tissue and muscle pull; thus, 50% was taken as the dividing figure.
23
For Group A, there was only one failure case (type II), and the mean survival time was 95.5% at a mean survival time of 14.57 years (CI 95%). For Group B, there were eight failure cases noted (2 type II, 4 type III, 2 type IV), (4 EBBI score 0, three EBBI score 1, 1 EBBI score2), and the mean survival time was 45.5% at a mean survival time of 8.02 years (CI 95%) (Figure 5). It suggested that a lower radiological score of EBBI might lead to an increased failure rate and as seen from the group B results, any EBBI score of less than two which is less than 50% is not desirable Our results concurred with the previous studies about the importance of a sufficient bone formation at the bone-implant junction.
17
Shows Kaplan Meier curve for Group A and B. The two curves show the survivorship of each group with Group A: EBBI score 3–4; Group B: EBBI score 0–2.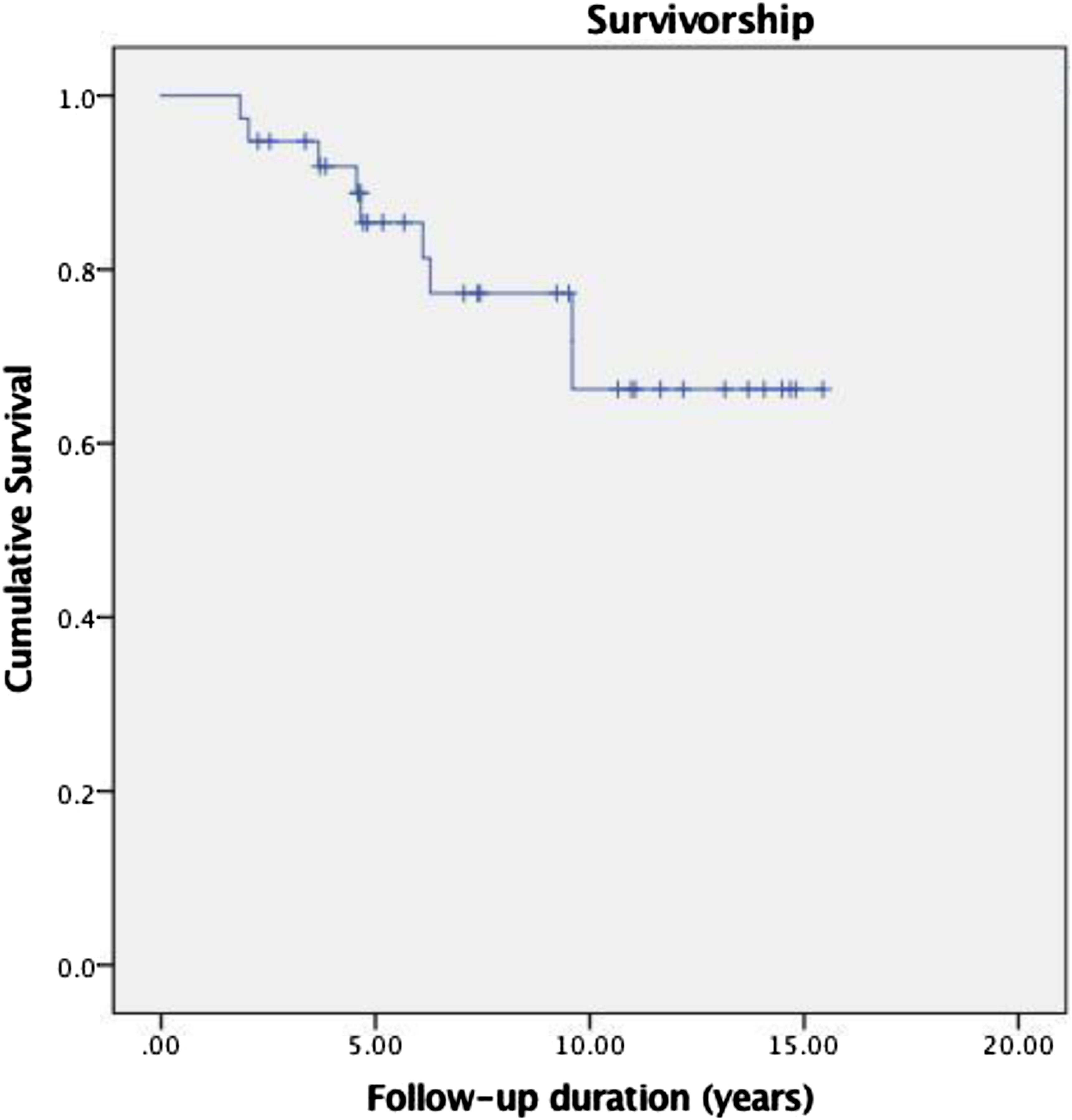
Furthermore, it was reported that fractures of intramedullary stems tend to occur if the stem diameter was less than 12 mm. 24 In our study, there was no difference between the stem sizes of both failure (N = 9) and non-failure (N = 29) groups. However, the mean diameter was only 9.41 mm in the non-failure group. Given there is no increased failure despite a stem diameter smaller than 1 mm, our results suggested that the EBBI predicts the failure rate but not the stem size. As for the remaining bone length, the mean was 217.55 mm in the non failure group and 229.78 mm in the failure group which showed no significant difference (p = 0.61). There was also no difference noted in the stem length with the non failure group of 114.31 mm and the failure group of 112.33 mm (p = 0.50).
Factors leading to successful EBBI formation such as cementation and whether it is porous or hydroxyapatite coated were also compared with no difference seen. However, it is worth noting that for the porous group and hydroxyapatite coated, there is only no statistical difference marginally (p = 0.056). This may be accounted by the high healing potential in the paediatric population. It may be ideal if longer follow up and a larger patient group can be further recruited to differentiate whether a genuine difference exists.
Infection
Other than EBBI, endoprosthetic infection was another critical factor in governing the failure rate. Infection itself may cause failure and may also cause poor EBBI infection as infection disrupts the local biology and affects bone growth. In the two Type four failure cases, one case resolved with simple debridement and antibiotics. In the other case, it resulted in above-knee amputation ultimately. Strict infection control measures had been applied intraoperatively. However, there was persistent sinus discharge from the wound after the operation which may have caused chronic infection. Moreover, there was raised eosinophilic count in the early stages but not neutrophilic counts suggesting a possible sinus formation due to metal allergy, with a secondary bacterial infection. For this patient, the C-reactive protein and the white cell count were normal. The raised eosinophilic count returned to normal after removal of the metal implant.
Endoprosthetic infection after limb salvage surgery ranged from 4.6% −28.6%.9,10,25–28,30,31 Tsagozis et al. had also suggested a high complication rate (76%) after the extendible endoprosthetic replacement of the proximal tibia. 32 It was accounted that infection cases were due to non-invasive implants. In our study, various factors like accurate preoperative planning, standardized antibiotic regime, custom endoprostheses for optimal soft tissue tension whenever the off-the-shelf implants did not fit to the bone reconstruction, EBBI with the modern implant design and biological augments at the bone-implant junction, and meticulous wound closure all contributed to the low infection rate.
Bone-stem ratio
Bergin et al. 11 reported that a higher bone-stem ratio would predict aseptic failure since the implant durability was related to the stem adequately filling up the intramedullary canal. Our results showed no difference in the bone-stem ratio between the two groups as our patient group was of paediatric population while there were no age limitations in Bergin’s study. We postulate that after successful EBBI formation, the whole bone collar construct shares the loading stress instead of localizing at the bone-implant interface. This would indirectly improve the overall strength and stability of the overall construct and result in lower failure rate. Thus, EBBI may be a more important prognostic factor for successful survivorship of an endoprosthesis in paediatric population.
Cementation
Cementation was previously proposed as important in maintaining the longevity of the implant. In our study, six cementless cases (mean bone stem ratio 2.87, mean stem length 86.7 mm) out of the 38 did not show failure at the lastest follow-up assessment. Thus, we believe that other factors may be playing a more critical role in providing structural stability for the endoprosthesis. As long as the cemented or cementless fixation can provide the initial stable biomechanical environment, the subsequent osseointegration of implant with EBBI may ensure implant longevity.
Musculoskeletal Tumor Society
Musculoskeletal Tumor Society was 29.6 overall. The score was obtained from 29 patients with the other patients excluded due to revision. It is seen that the patients enjoyed a good outcome after surgery in the successul cases. The main deduction usually came from the function category. As most of these patients had hobbies or sports demanding high function of the lower limb, they often find it hard to return to their preoperative level after operation and thus points were usually deducted fromt the function category.
Limitations
Our study had several limitations. It was a retrospective study and observational in basis. No randomization had been done. Second, no control group could be allocated. For the assessment of the EBBI, the only radiological assessment was done as the histological analysis was not possible. This may mask that some implants may have had good radiological evidence of osseointegration, but direct osseous ingrowth had not occurred. It is believed that with good osteointegration, there will be less micromotion and less chance of loosening and thus contribute to mechanical support initially. However, with time, particle wear may still cause loosening. Also, there were mixed implant types, and the duration of follow-up was not long enough for some. Lastly, a larger sample size may be needed to differentiate differences in other factors.
Conclusion
Our results showed that with the modern design of tumor endoprostheses, paediatric patients with lower extremity sarcoma could achieve good long-term results with 10-year-implant survival of 86% without aseptic loosening and an excellent limb function with a mean MSTS score of 29.6. EBBI is the most critical factor governing the aseptic loosening. We hope our readers may pay attention to EBBI in the future when predicting or monitoring for potential failure cases. Also, the results may provide a reference for surgeons managing Asian paediatric primary bone sarcomas. Contrary to the past findings of smaller stem diameter leading to a higher failure rate, our findings suggested that despite smaller body builds in Asians, the use of a stem with a smaller diameter is not contraindicated as long as an EBBI is ensured.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.