
Abstract
Keywords
Introduction
The posterolateral rotatory instability (PLRI) was proposed by O’Driscoll SW in 1991. This type of instability produces pain and disability of the involved elbow while performing pivot activities, such as rising from a chair or pushing up. Insufficient lateral ulnar collateral ligament (LUCL), a component of the lateral collateral ligament (LCL), is the underlying pathology of PLRI and is frequently a consequence of elbow dislocation.1,2,3 However, the etiologies from atraumatic events were also reported. Multiple corticosteroid injections or repetitive abnormal forces on the LCL, like chronic crutches usage, are common examples.1,4,5
History-taking and physical examination provide paramount information for diagnosis.1,2 The posterolateral drawer test and lateral pivot-shift test are the most useful diagnostic maneuvers. The lateral pivot-shift test is 100% sensitive in anesthetized patients, but only 38% sensitivity is revealed in conscious patients. 6 Moreover, in atraumatic PLRI, with subtle or occult instability, even lower sensitivity (16.6%) is reported. 7 The provocative tests, such as the push-up test, chair-rise test, and pivot-shift apprehension test, are also helpful in the diagnosis (83% sensitivity).7,8 Nevertheless, the provoked symptoms during the tests may be interfered with by pain from other causes, and it also depends on the examiner’s experience.
Likewise, imaging modalities, such as plain film or MRI, have limitations. Since they are static investigations, and the LUCL is obliquely arranged to the MRI’s axis, hardly observed under the MRI, they can lead to a false negative result.9,10 Simple stress radiograph may be a dynamic modality, but it cannot evaluate the rotational instability found in PLRI. Using the knowledge about biomechanics, while the pivot-shift-deforming force is applied to the PLRI elbow, the forearm is externally rotated on the distal humerus, causing posterolateral subluxation of the radial head and external rotation of the ulnar on the trochlea. This phenomenon can be seen directly during arthroscopy as a widening of the ulnohumeral gap of more than 2 mm. 4
Aiming to find a preoperative diagnostic tool, a cadaveric study 11 measuring the lateral ulnohumeral gap difference; the same gap as the mentioned arthroscopic test was performed. In the completely-cut-LCL elbow, more than 4 mm difference was revealed between resting and stress positions. This ultrasonographic test is an interesting preoperative test, but it can only be applied to diagnose atraumatic PLRI, which is more difficult to diagnose than gross instability. However, some cadaveric study limitations, such as the preservative technique or the status of elbow before death, are questionable issues. Consequently, we conduct the sonographic posterolateral rotatory stress test to examine the ulnohumeral gap difference in healthy volunteers. The hypothesis of this study is the normal ulnohumeral opening gap difference is less than 2 mm, as in the previous arthroscopic report. 4
Material and Method
This study was approved by the review board and ethics committee of Srinakharinwirot University with approval NO. SWUEC-404/2563F. All participants provided written informed consent before anticipating. A total of 21 participants (9 males and 12 females) who presented at HRH Princess Maha Chakri Sirindhorn Medical Center, Srinakharinwirot University between May and June 2021 were recruited for this study. The inclusion criteria were (1) volunteers aged 20–60 years old, (2) no history of trauma around the elbow, and (3) no history of chronic elbow pain or current elbow symptoms. The exclusion criteria were (1) previous deformity of the elbow, (2) history of previous injection or surgery around the elbow, (3) positive posterolateral rotatory drawer test, pivot shift apprehension test, or chair-rise and push-up tests, and (4) hyperlaxity syndrome according to the Beighton’s score of 4 or more.
After recruitment, the sonographic posterolateral stress test was conducted. The participants were examined using the hockey-stick ultrasound probe transducer of Aixplorer® ultimate start guide, SuperSonic™ Imagine ultrasonography, 1–20 MHz. The author performing the intervention is a sports medicine specialist in the orthopedics department, NM.
Outcome measurement
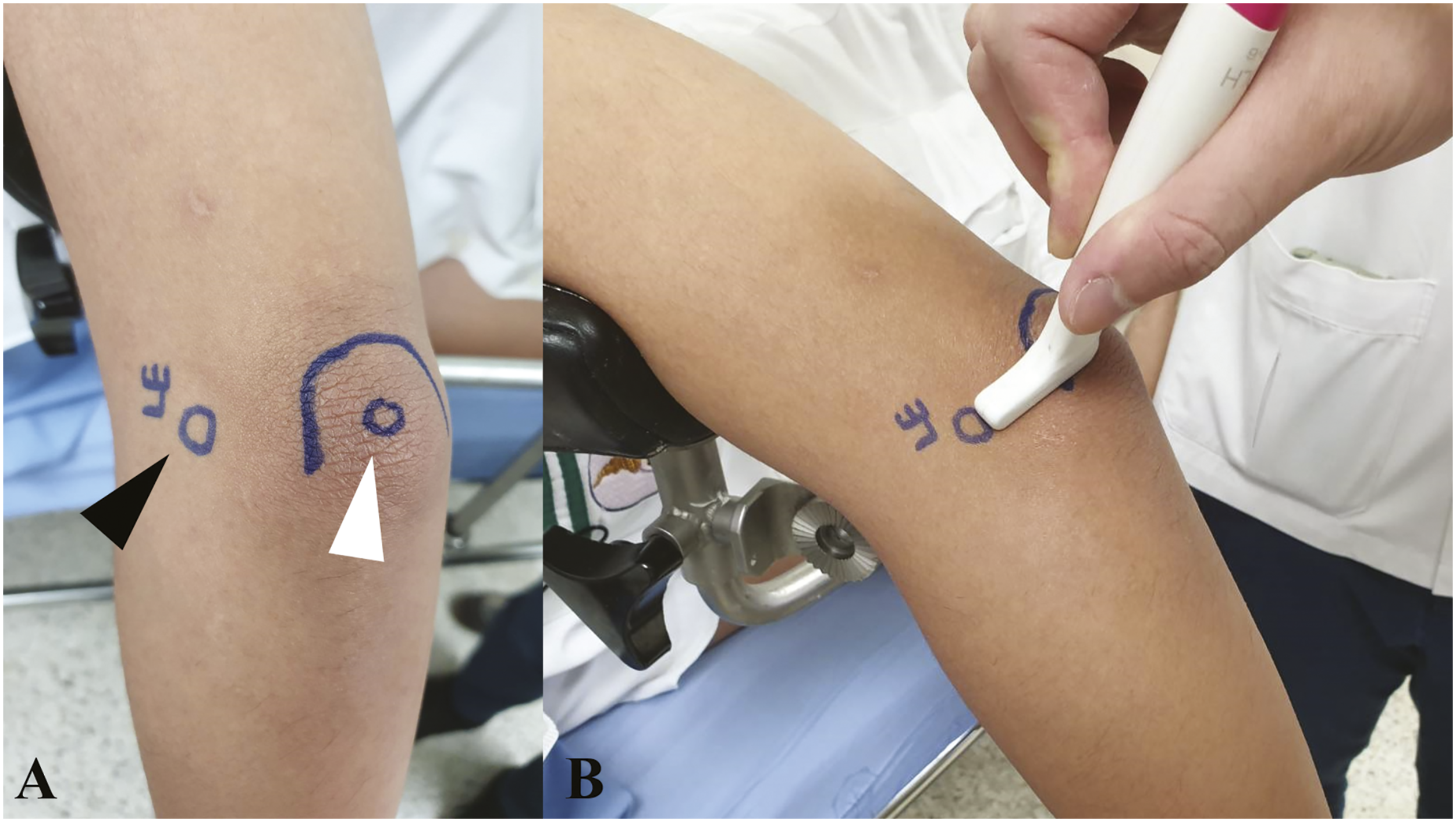
To begin with, participants were asked to be in a lateral decubitus position. Then their left elbow was placed on the armrest support in 30-degree elbow flexion and neutral rotation (Resting position) (Figure 1). Proceeding that, the ultrasound probe was placed on the lateral epicondyle, 1 cm distal to the olecranon process and perpendicular to the longitudinal axis of the ulnar (Figure 2). Without the application of supination force, an image was taken representing the resting ulnohumeral gap (Figures 3(a) and (c)). The participant was set in the left lateral decubitus position to examine his left elbow. An assistant stabilized the participant’s arm to prevent external rotation of the shoulder during forced-forearm supination. The examiner used his left hand to control the participant’s forearm position. (A, B) An ultrasonographic probe was applied at the longitudinal axis between the lateral epicondyle (Black arrowhead) and 1 cm distal to the olecranon tip (White arrowhead). (A) “Resting position” ultrasonographic picture. The resting ulnohumeral gap was measured (Yellow double arrow). (B) “Stress position” ultrasonographic picture. The stress ulnohumeral gap was measured (Red double arrow). (C) Bone model demonstrating the ulnohumeral gap during resting position (Yellow arrowhead). (D) Bone model demonstrating the ulnohumeral gap during stress position causing external rotation of the ulnar on trochlea (Red arrowhead).

Next, the author used another hand to apply a supination force on the elbow, and the assistant helped stabilize the arm to prevent shoulder external rotation during forceful forearm supination (Stress position). Force was gradually applied to the volunteer’s forearm until resistance was felt and no further motion was seen in the sonograph. An ulnohumeral gap picture was taken showing the stress ulnohumeral gap (Figures 3(b) and (d)).
Completing the examination in resting and stress positions is equal to 1 cycle. A total of 3 cycles were repeated with a resting period of 5 minutes between cycles. Using the electronic calipers of an ultrasound machine, the ulnohumeral gap or distance was measured between the most hyperechoic edges of humerus and olecranon in millimeters (Figure 3(a) and (b)). The mean resting ulnohumeral gap, mean stress ulnohumeral gap, mean ulnohumeral gap difference, and intraobserver reliability in each cycle were then calculated. Similarly, the participant’s right elbow was then examined using the same methods.
If participants experience pain or muscle cramping during the procedure, the test will be halted. Then they will be symptomatically treated and will not be included in the statistical analysis.
Statistical analysis
The statistical analysis was done using IBM SPSS version 26 software and Microsoft Excel. The demographic data included consists of age, gender, height, body weight, body mass index, dominant hand, and Beighton’s score. Age, height, body weight, and body mass index were shown as mean, standard deviation, and median. Gender, dominant hand, and Beighton’s score were presented as frequency and percentages. The means of ulnohumeral gap in resting position, stress position, and ulnohumeral opening gap difference were calculated and presented in millimeters. The intraclass correlation coefficient (ICC) was used to calculate the intraobserver reliability between each cycle. The sample size was estimated from the study, “The sonographic posterolateral rotatory stress test for elbow instability: a cadaveric validation study”. With the parameters; 80% power, 95% confidence interval, p-values < 0.05, more than 0.8 of expected ICC, and 10% drop out rate; 40 elbows were required. We used two-way random models, a single rating, and the same levels of agreement for the calculation of agreement. The level of agreement was stratified as follows; 0 to 0.20 representing a slight agreement, 0.21 to 0.40 as fair agreement, 0.41 to 0.60 as moderate agreement, 0.61 to 0.80 as substantial agreement, and a value above 0.80 represents perfect agreement. The Paired t-test was used to compare the means of ulnohumeral gap in resting position, stress position, and ulnohumeral opening gap difference between males and females.
Results
Demographic data of participants.

Means of ulnohumeral gap in resting position, stress position, and ulnohumeral opening gap difference between males and females.

*Values are given as mean and standard deviation. p-value < 0.05 analyzed as statistically significant.
Intraobserver reliability (N = 42).

ICC = Intraclass correlation coefficient
Discussion
At the present, several modalities including history-taking, physical examination, and imaging are used together to diagnose atraumatic PLRI and are then confirmed by arthroscopy intraoperatively. Under elbow arthroscopy, patients with atraumatic PLRI have ulnohumeral gap widening while performing passive forearm supination. Chanlalit and Dilokhuttakarn 4 reported a positive drive-through sign and ulnohumeral joint space widening of more than 2 mm when force was applied to supinate the forearm during elbow extension in the atraumatic PLRI cases.
As an adjunct to preoperative diagnosis, MRI is one effective modality, providing a non-invasive preoperative diagnosis of PLRI. However, it only provides static imaging causing difficulty in assessing rotational movement and an obliquely-oriented ligament like the LUCL.9,10 Batlle et al. 9 reported that up to 23% of the LUCL was incompletely visualized under MRI, and it was visible in only 78% of healthy volunteers.
Ultrasonography is another non-invasive choice for preoperative investigation.12,13 One major advantage of ultrasonography is the provision of dynamic imaging allowing real-time assessment of the elbow upon motion. A subtle subluxation or occult instability may be observed during movement and may be detected under ultrasonography. Camp et al. 11 reported that the sonographic posterolateral rotatory stress test can detect an increase in the posterolateral ulnohumeral laxity, the same way an increased ulnohumeral gap widening sign was seen under arthroscopy. The results showed that the mean sonographic ulnohumeral distance was 3 mm in resting position and 4 mm under posterolateral rotatory stress; therefore, the mean sonographic ulnohumeral opening gap difference was 1 mm in an intact elbow. After a complete cut of the LCL, the gap difference was raised > 4 mm. Nevertheless, their study has some limitations. First, since it is a cadaveric study, the prior condition of the elbow before death is unknown. Second, the preservative method might alter the status of the ligaments. Lastly, the results may not represent the subtle subluxation found in atraumatic PLRI.
The purpose of our study is to report the outcomes of normal ulnohumeral opening gap difference between elbow at resting and stress positions, under forceful supination to the forearm, while performing ultrasonography in healthy volunteers. The results show that the overall means of ulnohumeral gap in resting and stress positions are 2.55 ± 0.69 mm and 3.16 ± 0.80 mm, respectively; and the mean ulnohumeral opening gap difference is 0.61 ± 0.32 mm. There is no statistically significant difference between males and females. Recently, Robertson et al. 14 reported ulnohumeral gap measurement using a different maneuver. The result of ulnohumeral gap difference, median laxity of 0.8 mm (0.4–1.1 mm) is similar to our study. In this study, the operator applied external rotational force to the proximal forearm with the same hand used for ultrasonographic probe placement while the other hand fixed the arm. However, there might be difficulty assessing patients with large forearms or muscular features. Our maneuver was adapted from arthroscopy and external rotation force was applied through the distal forearm. The flat shape of wrist makes it easier for the operator to apply supination force. Furthermore, a longer lever arm provides a better mechanical advantage during the maneuver.
From our result and Robertson et al.
14
studies, we found that the ulnohumeral opening gap difference is less than 2 mm in healthy volunteers, similar to the study by Chanlalit and Dilokhuttakarn.
4
From our experience, the patients who were diagnosed with atraumatic PLRI mostly had a positive sonographic posterolateral rotatory stress test with more than 2 mm ulnohumeral opening gap difference (Figure 4). The ability to compare with the contralateral side is another advantage of this test. If the contralateral side shows a negative test, the positive test on the symptomatic side likely indicates that instability is the cause of the symptom rather than the patient’s joint laxity. (A, B) Positive sonographic posterolateral rotatory stress test in atraumatic posterolateral rotatory instability elbow. (A) The resting position in atraumatic posterolateral rotatory instability elbow. (B) The stress position in atraumatic posterolateral rotatory instability elbow. (C, D) The same patient’s asymptomatic contralateral elbow. (C) The resting position in the asymptomatic elbow. (D) The stress position in the asymptomatic elbow.
The limitations of this study are that the ultrasonography is operator-dependent. The experience of the examiners indirectly determines the results. From our study, the level of agreement for intraobserver reliability is substantial to perfect agreement (ICC=0.61–0.9), but our study is single-operator, so the interobserver reliability and validity of this test should be further investigated. During ultrasonography, participants may resist our force, or they might experience pain or muscle cramping. Furthermore, as this study has a small number of participants, increasing the number of samples and re-evaluating the data using a subgroup analysis based on participants’ age may help improve the plausibility.
In conclusion
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Srinakharinwirot University.