
Abstract
Purpose
Hip fracture is common in older patients and is associated with high mortality and functional impairment. The Geriatric Nutritional Risk Index (GNRI) evaluates the risk of malnutrition-related complications, and the Barthel Index (BI) evaluates older patients’ functional status. The study aim was to determine the risk factors for both death and decreased BI within 1 year after hip fracture.
Methods
We retrospectively reviewed the records of 108 patients who were treated for hip fractures in 10 public or private hospitals from February to July 2007. Participating facilities comprised eight public or private hospitals with 200–499 beds, and two private or orthopedic hospitals with 20–199 beds. We evaluated several risk factors for death and lower BI within 1 year after hip fracture.
Results
The mortality rate within 1 year postoperatively for patients who survived inpatient stay was 6.5% (7/108). The proportion of patients with decreased postoperative BI was 43.6% (44/101). Binomial logistic regression analysis showed that several factors, including low GNRI (odds ratio [OR]: 0.80; 95% confidence interval [CI: 0.68–0.93]), were risk factors for death within 1 year. Postoperative delirium (OR: 8.84 [1.52–51.6]), postinjury dementia (OR: 34.8 [3.01–402]), preinjury BI (OR: 1.05 [1.02–1.08]), and preinjury dementia (OR: 6.22 [1.73–22.4]) were risk factors for decreased postoperative BI.
Conclusions
Our findings indicated that lower GNRI was a risk factor for death within 1 year of hip surgery and that delirium and dementia were among the risk factors for decreased BI 1 year after hip fracture.
Introduction
Hip fracture is a common injury in patients of advanced age and results in high morbidity and mortality rates. 1 The incidence rate of hip fracture is increasing and is expected to double by 2040. 2 Additionally, hip fracture is associated with high mortality; mortality within 1 year ranges from 20%–40%. 3
Malnutrition is reportedly associated with poor outcomes following hip fractures.4–6 The Geriatric Nutritional Risk Index (GNRI) was designed to examine the risk of nutrition-related complications in patients of advanced age,7,8 and has been shown to be a significant predictor of prognosis in many diseases, including cancer.9–16 Studies have reported that the GNRI is a predictor of poor outcomes in patients who have undergone orthopedic surgery, including surgery for soft tissue sarcoma, and patients undergoing hemodialysis.17–19
The Barthel Index (BI) is a widely approved and thoroughly evaluated questionnaire that assesses the functional status of older patients.4,5 The BI comprises 10 questions that relate to basic activities of daily living. The BI has been validated for many medical conditions, including stroke, spinal cord injury, heart failure, pneumonia, and hip fractures.5–9
We hypothesized that risk factors existed for both death within 1 year after hip fracture and decreased BI 1 year after hip fracture. The risk factors of mortality following hip fracture surgery have not been well identified. Although some studies have evaluated hip fracture and nutrition, 20 few have used the GNRI. In addition, we believe that it is necessary to evaluate not only mortality but also BI decline 21 in the long term. The aim of this study was to determine the risk factors for both death and decreased BI within 1 year after hip fracture.
Materials and methods
Patient data and settings
We retrospectively reviewed the records of 108 patients who were treated for hip fractures in Kagoshima Prefecture and the neighboring Kobayashi City at 10 facilities from February to July 2007. Participating facilities comprised eight public or private hospitals with 200–499 beds, and two private or orthopedic hospitals with 20–199 beds. To minimize the risk of bias, this was a multicenter study involving hospitals of different sizes.
Inclusion and exclusion criteria
Eligible patients were those with hip fractures at the participating institutions during the study period. The exclusion criteria were as follows: (1) second hip fracture on the contralateral side during the study period (n = 4); (2) patients who died during their hospital stay (n = 10); and (3) declined to participate (n = 43). We also excluded patients with missing data (data not shown). The initial number of eligible patients was 199. After applying the exclusion criteria, 142 patients remained. After excluding patients with missing data, the final number of included patients was 108.
Variables
We assessed the following clinical characteristics, which previous research suggests affect the outcomes of interest.22–25 Data on these characteristics were collected from the patients’ medical records and treated as independent variables: sex, age, height, weight, preoperative albumin concentration, preoperative C-reactive protein concentration (mg/dL), operation type (bipolar hip arthroplasty/compression hip screw; short femoral nail/cannulated cancellous screw; Hansson hook-pin), incidence of postoperative delirium, preinjury BI, 1-year postoperative BI, preinjury dementia, postinjury dementia, death within 1 year following injury, preoperative waiting period, and fracture site (femoral neck/trochanter).
Geriatric nutritional risk index
The GNRI was calculated from serum albumin concentration (g/L) and body weight (kg) using the following formula: GNRI = (1.489 × albumin) + [41.7 × (body weight/ideal body weight)].
The GNRI defines four grades of nutrition-related risk: major risk (GNRI <82), moderate risk (GNRI 82 to <92), low risk (GNRI 92 to ≤98), and no risk (GNRI ≥98). Body weight or ideal body weight was set to 1 when the patient’s body weight exceeded the ideal body weight. 7 A body mass index of 22 kg/m2 was considered an ideal body weight.10,26
Primary and secondary outcomes
The primary outcome in this study was mortality within 1 year after hip fracture. The secondary outcome was decreased BI 1 year after hip fracture, as a marker of functional decline.
Statistical analysis
Data are presented as the mean and standard deviation for normally distributed values, and the median and range for non-normally distributed values. Differences in the variables between the groups were examined using Student’s t test, the Mann–Whitney U test, Fisher’s exact test, and the Cochran–Armitage test. Multivariable stepwise binomial logistic regression analysis was performed. Correlation coefficients were analyzed using Spearman’s rank correlation coefficient. When the correlation coefficients between explanatory variables were >0.6, only the explanatory variable showing the highest correlation with the objective variable was selected. Because of the relatively small number of patients and the large number of explanatory variables, we used a stepwise variable selection method, following a previous study. 27 Statistical analysis was performed using the add-in software BellCurve for Excel (Social Survey Research Information Co., Ltd., Tokyo, Japan).
Ethics approval and consent to participate
The study protocol was approved by the institutional review board of Kagoshima University and the study was performed in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. All patients provided written informed consent for publication of their medical data.
Results
Patient demographic data (n = 108).
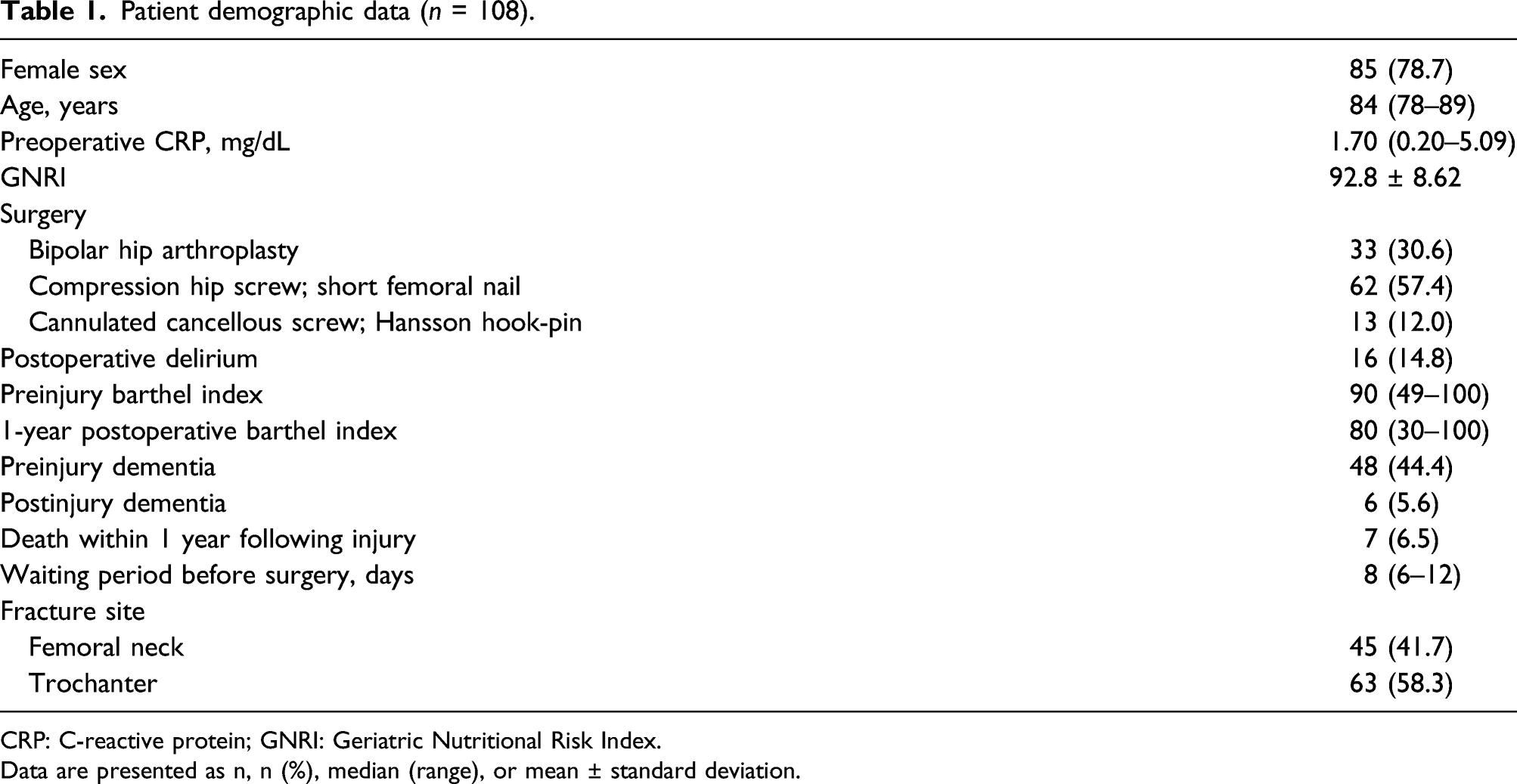
CRP: C-reactive protein; GNRI: Geriatric Nutritional Risk Index.
Data are presented as n, n (%), median (range), or mean ± standard deviation.
Differences in variables between patients who died within 1 year and patients who survived for >1 year.

CRP: C-reactive protein; GNRI: Geriatric Nutritional Risk Index.
Data are presented as n, n (%), median (range), or mean ± standard deviation.
*p < .05.
Binomial logistic regression analysis of risk factors for death within 1 year.

OR: odds ratio; CI: confidence interval; GNRI: Geriatric Nutritional Risk Index.
Coefficient of determination (R2) = 0.365.
*p < .05, **p < .01.
Differences in variables between patients with and without a reduced barthel index within 1 year.

CRP: C-reactive protein; GNRI: Geriatric Nutritional Risk Index.
Data are presented as n, n (%), median (range), or mean ± standard deviation.
*p < .05.
Binomial logistic regression analysis of risk factors for barthel index reduction.

OR: odds ratio; CI: confidence interval.
Coefficient of determination (R2) = 0.283.
*p < .05, **p < .01.
Discussion
Several reports have shown that various factors, including sex, age, and cognitive impairment, increase the risk of mortality after hip fractures.28–30 In the present study, the multivariate analysis showed that only GNRI significantly differentiated between patients who died within 1 year and those who survived. Our findings suggest that improvement of nutritional status may be an effective approach to prevent death following hip fracture. Nuotio et al. 31 reported that malnutrition was associated with mortality after hip fracture. Their finding is consistent with our results; however, they used the Mini-Nutritional Assessment Short Form to evaluate nutritional status. Although more than 70 nutritional assessment tools have been used with different populations, 32 a fully sensitive and specific nutritional assessment tool remains to be developed. 33 The Mini-Nutritional Assessment Short Form comprises six sections: appetite or eating problem, recent weight loss, mobility impairment, acute illness/stress, dementia or depression, and body mass index. 34 In contrast, the GNRI is calculated using blood albumin concentration, height, and body weight. Calculation of the GNRI is an easier and more useful method for retrospective studies in many hospitals because blood albumin concentration, height, and body weight are commonly recorded in medical charts. Delmi et al. 35 reported that complication and mortality rates after femoral neck fracture were significantly lower in patients receiving nutrient supplementation. However, although one systematic review reported that oral multinutrient feeding of non-protein energy, protein, and some vitamins and minerals may reduce unfavorable outcomes (death or complications), as evaluated by five trials, there was no effect on mortality. Four trials examining nasogastric multinutrient feeding showed no evidence of an effect on mortality. 36 Future trials of nutritional intervention are required because the evidence for its effectiveness remains weak. 36
Mental state, prefracture physical and psychosocial functioning, comorbidities, female sex, nutritional status, postoperative pain, length of hospital stay, and complications are previously reported factors associated with patients’ postoperative health status and quality of life. 37 Our multivariate findings showed that delirium is a risk factor for BI reduction. A recent multicenter retrospective cohort study showed that patients with delirium are more likely to have a worse BI after hip fracture. 38 Several studies have shown that delirium is associated with a higher rate of complications and mortality; therefore, preventing delirium is very important.39–41 Notably, these studies evaluated mortality and complications; to our knowledge, no studies have evaluated functional improvement, as in our study. However, some studies have reported interventions to prevent delirium in hip fractures.39,42 Research shows that multifactorial interventions can prevent delirium in patients. 43 One study also showed that use of a proactive geriatrics consultation reduced the development of delirium by more than one-third and reduced the development of severe delirium by more than one-half following hip fracture surgery. 44 It is relatively easy to provide geriatric consultations for hospitalized older people.45,46 Because delirium is not inevitable following hip surgery, interventions that are relatively easily to implement should be used by geriatricians, nursing-based interventionists, lay interventionists, and volunteers.47,48
Our study has several limitations. First, data on fracture types and rehabilitation schedules were lacking. The type of hip fracture and whether the fixation status is good or poor may affect the timing of the start of rehabilitation. Second, we tested relatively few patients and variables; a study with a larger cohort is required to more accurately assess the risk factors. Third, we did not find a strong effect for the classic predictors of mortality, age, and sex (although sex was a significant predictor, the 95% CI was wide). The lack of a strong effect for these predictors may reflect large variability or the relatively small sample size. Because we used only the GNRI to evaluate nutritional status, other nutritional analysis tools should be used to assess patients with hip fracture. Additionally, we did not examine nutritional intake following surgery; patients’ dietary habits should be examined more comprehensively. Finally, it is possible that facility selection and the exclusion of patients with missing data introduced bias.
One of the strengths of our study is that although there are studies evaluating hip fracture and nutrition, few have used the GNRI. The GNRI has been shown to be a strong predictor of several diseases, and is a simple and useful tool. The use of complementary nutritional therapies might improve mortality associated with hip fractures. Another strength is that this was a multicenter study, and the possibility of selection bias was lower than with single-center studies; the 10 participating centers serve a wide area. This study also evaluated long-term functional outcomes, unlike previous studies that have used short-term evaluations. We also evaluated BI decline as well as mortality; no previous studies have evaluated delirium and functional impairment (BI) long term. Although delirium is often discussed in relation to hip fractures, 41 to our knowledge, few reports have discussed delirium and reduced activities of daily living (BI). Nutrition and delirium have been shown to affect mortality and functional impairment (BI); therefore, improved nutrition and delirium prevention are important. Addressing these issues would benefit both patients and physicians. Our findings are generalizable to other populations and settings because hip fractures and delirium affect all older populations worldwide.
Conclusion
Our findings indicated that lower GNRI was a risk factor for death within 1 year of hip surgery and that delirium and dementia were among the risk factors for decreased BI 1 year after hip fracture.
Footnotes
Acknowledgements
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.