
Abstract
It has become something of a truism, that within various athletic subcultures pain and injury are regularly normalised as ‘part of the game’. One clear consequence which flows from this empirical reality is that athletes often need medical care in various forms. Recent developments in the gendered structuring of sport means that sportswomen are increasingly centred within this process. Yet, there is a broad consensus from sportswomen and academics alike that access to medical support and the availability of associated resources in women's sport is inadequate. Based on interviews with 17 women located in the United Kingdom, we cast new light on how medical support and care appears to be structured across various women's amateur sports. Two key findings are highlighted, firstly, that the majority of medical support was via first aid kits, which is problematic in their inconsistent restocking, and the availability of someone trained to use them. And, secondly, that there was a DIY approach to medical care which we explore via a discussion of athlete-to-athlete ‘team-doctoring’ – wherein sportswomen provided medical advice, care and treatments to each other. Our analysis of these two findings shows how medical care might be inconsistent, compromised and otherwise poor in quality, especially when viewed through the lens of critical scholarship about the sociology of sports medicine. This has specific consequences for the sports women we spoke with, and wider implications for our understanding of amateur sportspeople generally.
Performance sport and medicine
Findings from five decades of scholarship demonstrates the persistence of athletic subcultures in which bodies are routinely broken down and damaged as an accepted ‘part of the game’ (AlHashmi and Matthews, 2022a; Atkinson and Young, 2008; Hoch, 1972; Nixon, 1992; Smith, 1983). Such a finding has become something of a truism within critical studies of sport, and normative cultural expectations about how ‘real athletes’ should behave are central in sustaining these behaviours (see Matthews and Maguire, 2019 for a discussion). As Hughes and Coakley (1991) put it over 30 years ago, ‘the idea is that athletes never back down from challenges in the form of either physical risk or pressure, and that standing up to the challenges involves moral courage’ (p. 309). Such understandings are learned and embodied by athletes as they spend time playing their sports. This ‘cultural encoding’ of the body resonates with Nixon's (1992) argument that sporting environments are often dominated by ‘cultures of risk’ wherein an individual's ability to tolerate pain and injury is valorised. As such, ideas circulate in these sporting spaces that enable the normalisation of physical suffering and personal sacrifice (Hardwicke et al., 2024b; Liston et al., 2016; Matthews, 2021a; Matthews and Channon, 2016). Several consequences proceed from this; an obvious one being that athletes regularly need medical support in various forms, especially those playing at levels of sport where enhancing performance and winning are the main focus.
Waddington (2000) frames this process using the concept of medicalisation – whereby medical knowledge, care and treatments have gained increasing prominence as powerful features of social life. His analysis of sports medicine illustrates how athletes, especially those in high level sport, have become defined as a distinct population, akin to the chronically ill, in that they require medical care, ‘not because they necessarily have a clearly defined pathology but… simply because they are athletes’ (Waddington, 2000: 121). Not only have sports ‘insiders’ accepted the process of medicalisation but they have actively sought to increase their access to medical interventions, and with them various forms of surveillance, in the search for improvements in performance and competitive success (Edwards and McNamee, 2006; Malcolm, 2017; Waddington, 1996, 2000). Perhaps unsurprisingly then, numerous sports worlds, especially those with a commercialised and performance-orientated focus, are now also medicalised spaces wherein authority, control and power are often tied to medical expertise.
Critical scholarship exploring the sport and medicine nexus has highlighted the conflicts of interest that emerge between doctors, coaches and athlete-patients as a result of the mediating effect of social relations and the ‘culture of risk’ (Malcolm, 2006; Partridge, 2014; Waddington and Smith, 2008). Such work provides valuable insights into how relationships between athletes and care providers might impinge on the ability of medical practitioners to provide effective care, that is, to prioritise health outcomes over sporting performance. In this regard, researchers have found problematic consequences that flow from the structuring of such relations in rugby (Malcolm, 2006), football (Malcolm et al., 2017; Waddington and Roderick, 2002), combat sports (AlHashmi and Matthews, 2022a; Channon et al., 2021), and various other sports (Safai, 2003, 2004; Walk, 1997, 2004). Clearly, then, there are several overlapping issues within the provision of medical support associated with sporting participation, and performance-orientated sport specifically. In particular, we are interested in problems that flow from how social relationships between athletes, coaches, medical professionals and other sporting ‘insiders’ shape the medical knowledge and care received in amateur sporting spaces (taken here to mean participation at local, regional leagues/competitions or non-professional university teams). In this article, we focus specifically on how amateur sportswomen experienced, thought about, and interacted with each other in relation to medical care.
Women, performance sport, pain, injury and medicine
On the face of it, the expansion of accessibility, participation, media coverage and financial investment in certain women's sports marks out broadly positive and progressive shifts in gendered social relations and reflects changes in the traditionally uneven balance of power between the sexes (see Bowes and Culvin, 2021, for various examples). And, in parallel, sportswomen are increasingly embedded in sporting cultures of risk and they prescribe to, and embody, similar performance oriented and health compromising ideas as their male counterparts (Charlesworth and Young, 2004; Hardwicke et al., 2024a; Pike, 2005; Waldron and Krane, 2005; Young and White, 1995). Therefore, we argue here, that following women's long and complex history in various sports (Hargreaves, 1994), recent developments in the gendered structuring of sport – especially in the United Kingdom where our work takes place – means that sportswomen are increasingly placed within such performance-orientated sporting spaces that have faced consistent critical commentary from sociologists of sport. Here, the paradox of such ‘progress’, as defined in terms of the recent spurt in women's participation in sports in the United Kingdom, is the associated exposure to the ‘sport ethic’ (Hughes and Coakley, 1991), and the normalisation of sports-related pain and injury impacting on all athletes (see Hardwicke et al. (2024b) for a recent discussion around this point). This means that, through the increases in participation and progression of performance demands, sportswomen are having similar deleterious physical and psychological experiences as sportsmen (see the tragic story of rugby player Siobhan Cattigan for a recent example, cited in Atkinson, 2022).
And it is important to note here, that such clear experiential similarities, should not be confused with sameness. In that regard, as Charlesworth and Young's (2005) work provides a conceptual counter point: Women's experiences of sports involvement are not only often very different from those of their male counterparts, but are also likely to be unique in their own right, differing from one female to another, both between and among sports. (p. 91)
Within research focusing on, or related to, such medical care there is a broad consensus around the inadequate treatment and support across various levels of sport (Charlesworth and Young, 2004, 2005; Pike, 2005; Thing, 2004). In particular, Charlesworth and Young's (2005) work on sportswomen in English universities revealed that athletes often managed their injury experiences by talking through their ‘pain stories’ amongst each other as a coping strategy. According to the athletes this was largely due their lack of access to adequate and trustworthy specialist advice. Similarly, in her research on rowers in the United Kingdom, Pike (2005) argues the limited access to medical support led some sportswomen to be involved in a “culture of shared decision-making” (p. 213) characterised by exchanges of advice between teammates who had been through similar experiences with pain and injury.
When taken together these findings, especially in relation to the limited access to medical care, lead to a logical conclusion which Pike (2005) captures: It was apparent that, in the absence of available medical support, some of the club rowers took advice from within what Nixon (1992) termed the ‘sportsnet’, or network of personnel involved in the sporting subculture. Such advice was not always adequate, often being offered by those with a vested interest in the injured athletes continuing to participate with pain and injury. (p. 206)
Team-doctoring
‘Team-doctoring’, as first proposed by Safai (2003), is an idea that seeks to account for ‘the process whereby apparent medical knowledge is (mis)understood, recommended, transferred, interpreted and developed within a somewhat coherent team’ (AlHashmi and Matthews, 2022a: 153). Drawing on theoretical details from medical sociology and the study of lay medicine, and via interviews with male and female athletes in various combat sports, AlHashmi and Matthews (2022a, 2022b) develop team-doctoring as a useful way to frame how ideas about medicine and medical treatments might be shared among teammates and athletes in the absence of formally qualified personnel. Building on the well-developed body of research exploring pain, injury and risk in sport, a foundational premise of this work is that within sporting spaces, and especially those where medical support is absent or lacking, we might reasonably expect that coaches and athletes will develop and pass on knowledge about how to mitigate, manage, and negotiate sport-related pain and injury. While often experienced by athletes as useful, such advice and care is likely to be infused with a performance orientation to the body as well as incorrect, empirically unsupported ideas, and even mythical notions about how to treat injuries and bring about a return to ‘health’ (AlHashmi and Matthews, 2022a, 2022b; see also Matthews et al., 2023, discussion of myths in sport).
AlHashmi and Matthews (2022a) argued that within combat sports the process of team-doctoring is dependent on coaches’ lay expertise in sports medicine, wherein athletes often thought their coaches were able to help them manage certain injuries and return to training and competition. Here, the focus of such ‘medical advice’, ‘treatments’ and ‘protocols’ was most commonly shaped by athletes’ desire to continue within their sport – to ‘play on’ – and to prioritise performance rather than maintaining their overall health. Such lay expertise, in various forms, became a central feature of how athletes ‘cared’ for themselves and each other. And, importantly, this can form the basis from which athletes ignore, challenge or reject professional medical advice when it was available (AlHashmi and Matthews, 2022a, 2022b; Hardwicke et al., 2024b; Matthews, 2021a).
AlHashmi and Matthews (2022a) acknowledged that their data were heavily coach-led and concluded that athlete-to-athlete interactions in ‘team doctoring’ required further empirical investigation. Charlesworth and Young's (2004) and Pike's (2005) research on sportswomens’ experiences of pain and injury provide some evidence of such interactions. However, these works were largely focused on how sportswomen responded to the ‘culture of risk’ (Nixon, 1992) and the limitations of medical care within their sports, rather than on the intricacies of social relationships and how the lack of formal medical support was mitigated by a team-doctoring culture. It appears, then, that the concept of ‘team-doctoring’ may hold some potential for helping to explore such details and athlete-to-athlete interactions. It is this particular focus which we take up in this article.
We were axiologically drawn to research the experiences of amateur sportswomen due to our personal (pro)feminist leanings and sensitivity to gendered dimensions of sport. We focus on how various cultural traditions and structural features associated with sport might place women in situations where they risk their health, damage their bodies and hinder their recovery from injury. Our empirical aim was simple: speak with women to build upon the scholarship of AlHashmi and Matthews (2022a, 2022b) Charlesworth and Young (2004, 2005), Pike (2005) and Safai (2003) to help better understand amateur sportswomen's experiences. In particular, attention is directed towards how, and in what ways, these women might do medical care together. To that end, we detail findings around amateur sportswomen's access (or lack thereof) to medical support and their experiences of working together to manage the pain and injury commonly associated with their sports participation. In the context of the critical scholarship on the sociology of sports medicine, these findings show how sportswomen's medical care is inconsistent, compromised, and otherwise poor in quality, and they also have implications for amateur sport more broadly. In exploring these experiences we also further develop the inchoate concept of ‘team-doctoring’ which appears to speak well to the lives of the sportswomen within this study.
Methodology
We approached the project by drawing on foreshadowing theoretical tools from a broadly social constructionist position, largely influenced by symbolic interactionist theory (Blumer, 1969). This, for us at least, means that a process of seeking to understand how people live within, and construct the world around them, was tentatively foregrounded as an initial focus. We have a particular focus on social relationships because of their importance in the production of frames of reference used by people to make sense of the world. Building on that start point, we were drawn to the topic within this article because of broad findings from (pro)feminist inspired scholarship that highlights how women regularly suffer the consequences of inequality, as reflected in social relations in sport and the uneven distribution of power, prestige and status. And our symbolic interactionist leanings mean we are also keenly focused on medicine and medical care as forms of, potentially harmful, social practice. This results in us exploring how relationships shape, and are in turn shaped by, various forms of medical knowledge and power relations embedded in the process of medicalisation. This position is informed by our reading of the extant literature discussed above, as such, it contextualises the remainder of this article, and in particular our axiological and methodological ways of approaching, empirically contacting and epistemologically grasping something of sportswomen's experiences in the world.
Each author has diverse experiences within sport, both academically and personally, and while an understanding of these would helped situate the work, the need for brevity dictates that we limit ourselves to a discussion primarily of the first author's background. DF is a white British woman living in the East Midlands of England. She has a background in both high-performance sailing and field hockey. As an active participant in both sports, she has experience of competing and training at various levels. These experiences were useful for the completion of this research, especially in terms of recruiting participants through friendship groups and extended networks, as well as being able to share some similar experiences with participants. With that said, the ‘closeness’ she has to some of the experiences meant there was a need to reflect upon taken-for-granted assumptions embedded in her analysis. Including the development of a more ‘critical eye’ through which to view and interpret women's accommodations to risky ways of behaving. The co-authors took the role of ‘critical friends’ and their approach held much in common with by Appleton's (2011) discussions. The main issue here was managing DF's ‘insiderness’. Some details of this process are outlined below in relation to how the analysis developed over time, empirically and theoretically.
After institutional ethics were granted, 17 women (defined here as people eligible to participate in women's sport) were interviewed: two were ‘in person’ interviews, and 15 were conducted online by DF, and recorded, with the consent of interviewees, using video conferencing software. They were recruited via an online survey about women's involvement in sport which DF advertised on various social media platforms. The interviews ranged in length from 20 to 47 min and were transcribed verbatim within 48 h. All identifying features were removed or modified and pseudonyms are used here in reporting the findings. Basic biographical information is provided in Table 1.
Biographical information of participants.
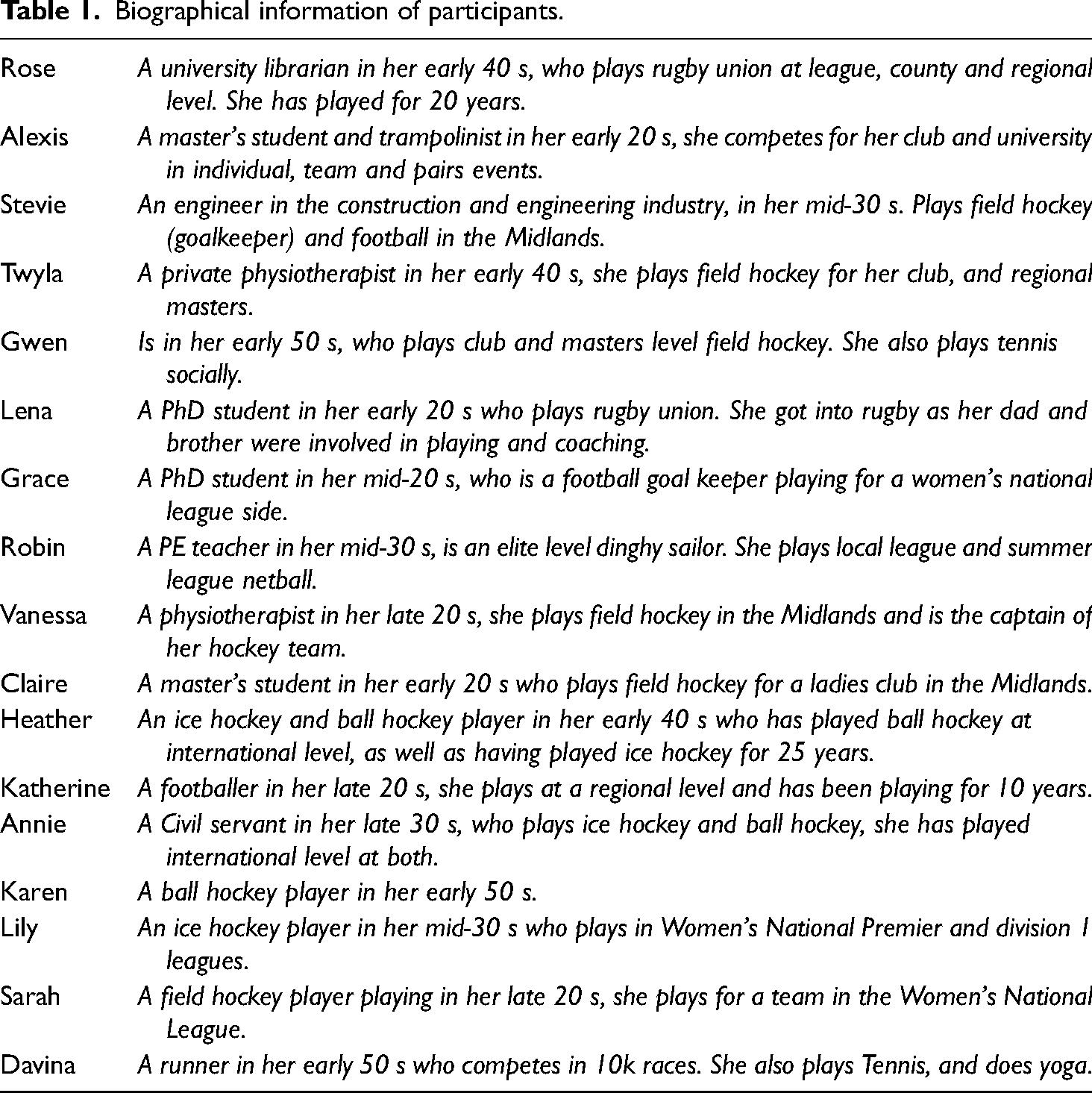
The interviews focused on women's health, sporting participation and medical care/support. While a broad semi-structured interview schedule was constructed, DF quickly developed a conversational style that flowed quite ‘naturally’ from some of the experiences and understandings she shared with the interviewees. This process allowed her to gently guide conversations towards medical care, injuries, pain, treatments and recovery. Given our proceeding comments around the preponderance of pain and injury in sport, it was no surprise that all 17 readily shared interesting, dramatic and sometimes worrying stories around such phenomena.
The sample were white, British, mostly university educated women, who, using Savage et al.'s (2013) discussion of social class, would likely fall into the ‘established’ or ‘technical’ middle-class bracket. This is obviously not a representative sample and therefore we do not use it to speak to the experiences of all amateur sportswomen. However, we believe it does align with a significant group of such women and, as such, the experiences of our interviewees, especially when discussed in relation to existing literature, provide us with an empirical and logical foundation upon which we make some broad but tentative analytical conclusions.
Our process of analysis was informed by Blumer's (1969) discussion of ‘sensitising concepts’; Prus (1996) captures this idea neatly when he said that: Blumer uses the term sensitising concepts to refer to these tentative, analytical notions. Sensitizing concepts suggest subsequent lines of inquiry and assessment, but in each case the researcher has the obligation of making the concept match up with the circumstances at hand rather than making the data fit the concept. (p. 132)
After an initial broad process of analysis that drew on points of departure from the extant literature, DF focused attention on terms and ideas specifically related to health, injury, medicine, treatment and the like. Several key empirical details became apparent and prompted further reading. These included: issues around access to various forms of medical care, the levelness of women's sports teams/leagues, the communication of medical knowledge, individual and group sport social dynamics, concussion and anterior cruciate ligament (ACL) injuries, female-specific health and wellbeing, including menses and the contraceptive pill, and the notion of ‘sisterhood’. DF built on her existing knowledge by conducting a review of literature on these and connected topics. This reading informed the refinement of our analysis and speaks to our dedication to the two way interaction between theory and evidence. This led to the grouping of data into two parts: (1) that which was insufficiently evidenced and required further consideration and data collection and (2) that which we felt was robust enough to form the basis for some important initial findings, that is to say, the data provided a relatively clear and coherent empirical basis from which important observations could be substantiated.
Based on this latter data grouping, and in collaboration with the research team, DF and CRM led a process wherein a coherent analytical and empirical frame was built, around which this article is presented. The goal here was to place the data in dialogue with existing work in the field as a means of advancing knowledge, in some small but significant way; in this case, our understanding of sportswomen's experiences of medical care, and the implications for medical care in amateur sport more broadly. DF refined this frame and produced a first draft. At this point the remaining authors helped shape and sharpen the analysis by encouraging clarification over the use of concepts and data. The findings that follow outline the ‘do it yourself’ (DIY) nature of amateur sportswomen's medical care and that of ‘team doctoring’.
Amateur sportswomen's access to medical support – first aid and DIY
The sportswomen in this study spoke of their broad alignment with the performance-orientated approach to sport as described in Hughes and Coakley's (1991) classic work on men's sport wherein they develop the notion of ‘the sports ethic’ (see also Berg et al., 2014). Similar findings have been highlighted in research that precedes our work (Charlesworth and Young, 2004; Pike 2005; Waldron and Krane 2005; Young and White, 1995). Perhaps the obvious outcome of this was that the women in our sample described a series of run-of-the-mill sporting injuries and pain – lacerations requiring stitching, black eyes, various impact injuries, twisted ankles and the like – that were a regular part of their participation. Alongside these stories were more dramatic accounts of serious injuries (defined by interviewees in a functional sense as resulting in time away from training/competing and some long-term physical consequences). These included concussion (mild traumatic brain injury), broken leg bones and injuries to ligaments. In this regard, the sportswomen's experiences shared much in common with the picture painted by literature on men's sport. It is these similarities, and their connection with medical care, that are our focus in this section.
The medical support that flowed from such physical damage revolved largely around access to first aid. This often included a coach, a fellow player or someone employed by the venue where the sportswomen were training or competing. Davina, who competed for a local amateur running team, described this basic level of access to medical support in matter-of-fact terms, and rationalised this by stating that she was ‘not elite enough’. Of course, regardless of the financial constraints that are associated with amateur sport, first aid can be adequate in a number of unserious medical situations, but several intertwined issues presented themselves to us upon a deeper reading of the social dynamics at work here. “…a first aid bag and that's it” - “It's sort of do it yourself.”
Alongside the stocking of first aid kits, and the quality of medical resources in them, the sportswomen also highlighted the absence of personnel to use such kits effectively. Sarah (Field Hockey) explained that ‘[there's a] first aid kit that no one really knows how to use’. Similarly, Lena and Claire stated: I think definitely we need more like medical staff on site or someone that's fully first aid trained. I don't even think my coach was first aid trained, so he was just going off intuition and ‘cause he was a rugby player just goes off what he knows. (Lena, Rugby) And, uhm, when you're playing there's just someone who has a first aid bag and that's it. Like there's just nothing, which I don't think is ideal, because then you've got nobody. [Some] people are first aid qualified, but if someone got a broken leg like I'm not qualified, I obviously can do something but … I feel like there should be somebody there that is specifically able to sort those situations out. (Claire, Field Hockey)
Thus, the provision of first aid appeared to be ‘more miss than hit’. In that regard, first aid kits provided the sportswomen, coaches and others connected to the team something that, if properly maintained, could be used, if someone was properly qualified, to give medical care and that in certain situations might work. The number of caveats and qualifications in that sentence marks out some layers of the problem here – that the provision of a basic first aid kit is insufficient medical support for many of the more serious but not uncommon sporting injuries, and this is especially the case with substandard stocking and in the absence of someone who is trained to us such equipment effectively.
The following examples further illustrate this issue: Uhm, I think we were playing [opposition team], and one of the [their] girls got smacked in the jaw, with a stick, and it definitely fractured her jaw. And there was no, uhm, they didn't have a first aid kit with them. And luckily we did, but then there was no one there to be able to provide her first aid, and we just had to call 999 and wait, wait for them. And you know, she really needed better medical care than that, I think. But then, there isn't any set up for that, in league hockey. (Twyla, Field Hockey) Uhm but when I was knocked out… Luckily we had a first aid person. On the side-lines. She wasn't great, to be honest. She didn't think she really knew exactly what she was doing and I think she was still training. But yeah, she came in and sort of helped out… I don't think she gave the best advice like she didn't, she didn't say don't go out [to play]. I didn't go out but she's like, she didn't say don't go out, she didn't say go to hospital if you feel this sort of stuff. (Claire, Field Hockey) As for the head injury, I didn't receive any specific care, because there wasn't any qualified first aiders on site. So, it was more of a self-sufficient thing, [we’re] gonna stop the bleeding and then we went to the hospital later on and they just glued it and butterfly stitched it. (Robin, Sailing) “…It's sort of help yourself…” Uhm, there's a first aid kit on the side of the pitch, but it's sort of help yourself… Maybe because of my professional background [as a physiotherapist] I would know how to treat [basic injuries]. (Twyla, Field Hockey) Actually hockey players are really good at first aiding themselves because rinks don't have good provision. (Heather, Ice and Ball Hockey)
Sportswomen, medical care and athlete-to-athlete team-doctoring
Usually, medical care is provided in a context where medical professionals advise and treat patients in a formal setting. In the amateur sporting spaces we explore here, it appears that ‘medical’ care was more-often-than-not provided by teammates to other teammates. The following examples from sportswomen who became designated as ‘go to’ care givers are illustrative: But you know I became known as the mobile pharmacy and I had a big box of painkillers and plasters. And you know, and all sorts of bandages in my bag. And you know if they needed anything they'd come see me. Sounds awful, actually. (Alexis, Trampolining) I’ve never done as much first aid in my life as I have at hockey. You know from anything from looking at a cut because they've cut their finger, from, I don't know…a dislocated shoulder, concussion. I've never treated so much first aid as I have done being a hockey player, you know. (Heather, Ice and Ball Hockey)
At other times teammates that provided care did have formal first aid training, as is the case with Vanessa who played field hockey: Well, I am the first aider for the team so if I get injured, we’re in trouble, but for the rest of the team, if it's soft tissue stuff then I’ve got a first aid kit and I’m first aid qualified. We can do kind of soft tissue stuff with Steri-Strips and cleaning wounds, but then obviously we’d bundle people off to hospital to get them checked. “We rely on other participants being medically trained”
As Rose remarked above, the sportswomen tended to feel lucky when they had this ‘unofficial’ access to someone with medical training beyond that of basic first aid. Furthermore, sometimes these teammates were described in celebratory terms. Take the following examples: [Teammate] at hockey got smashed, a ball smashed in her face and I think Vanessa [physiotherapist] treated her with stitches on the pitch side. That's just ‘cause Vanessa is trained. If she didn’t play then [injured teammate] wouldn’t have had that treatment. (Stevie, Field Hockey) We did have a paramedic on our team for a while, which was great. Obviously, off the books unofficially, she was like, yeah, that needs to go [to the hospital], no, you’re fine. That was brilliant. And then we swapped her for an A and E nurse, [who we had] for a while ‘cause her daughter was playing and she's like yeah, no that needs to go [to hospital]. (Heather, Ice Hockey and Ball Hockey)
These forms of athlete-to-athlete team-doctoring were not limited to the sportswomen's own teammates. In some cases, the opposition was called upon to provide medical care to injured players: We don’t have medical students obviously, but normally every other team we play has a medical student on it. They sort of help you, but we never really had anyone that was fully first aid trained. (Lena, Rugby) I know there are clubs who, yeah, one of their players happens to be, you know, a physio or whatever outside [of sport] and you see them running on and taking that role halfway through a game. There was one team that you know the goalkeeper will run up the other end. Take a glove off you know [so she could deliver some medical treatment]. (Grace, Football) But quite often or not, there's going to be a medic on one of the trampolines, like on one of the trampolining teams, so they’ll often get a medic over to, you know, just have a quick assessment and normally that's the case. (Alexis, Trampolining)
Our research design has not enabled us to tease out the reasons for the apparent prevalence in our sample of medically qualified personnel who were connected to women's sports teams. However, we expect that within a larger sample of sportswomen, patterns around the social class and educational backgrounds (particularly the importance of university sport) associated with different sports may well play a role in this process. What is clear, however, is that this phenomenon is one which the sportswomen in our sample readily acknowledged was a normal part of their training and competition.
It appears, then, from our data, that athlete-to-athlete team-doctoring, which takes various forms in terms of the types of medical knowledge and qualifications of those concerned, might be a more central organising feature of amateur women's sports. As briefly highlighted earlier, there are quite clear issues connected to medical support and care being structured in this way. Pike (2005), referring to Adler and Adler's work (1991) on deviancy, captures this well: The chance of health care originating within the sports network is high, as athletes are likely to be absorbed in a sporting subculture which supports and reinforces risk-taking, often as a direct response to the wider non-sporting community which labels such behaviour as ‘deviant’ (p. 6).
Previous research has highlighted that the process of team-doctoring is focused on maintaining sports performance rather than on restoring or enhancing health and wellbeing (AlHashmi and Matthews, 2022a, 2022b; Safai, 2003). It is reasonable to suggest that the women in this study were not overly concerned about whether the medical support they received was ‘official’, based on medical qualifications, or from the opposing team. Put simply, they just needed enough ‘doctoring’ to get them through the game or on to the next training session. While the existing literature on medical care in sport would raise some criticisms of this, the sportswomen themselves always described the availability of someone with even basic medical qualifications in positive terms. Of course, this makes sense from their position because of the DIO approach to medical support which they had largely accepted as normal in their sport.
Some tentative conclusions
As an initial exploration, based on a limited sample, into the medical care practices and relational interactions between sportswomen involved in amateur sports in the United Kingdom, we have described how the paucity of formal medical care has resulted in a ‘make do’ approach to first aid. We have highlighted two key features of the structuring of medical support and care which appear, from our data at least, to be important features of these sportswomen's experiences, which also point to implications for understanding the central features of amateur sport more broadly. That is, (1) first aid is the main form of medical support on offer and there appear to be issues in the stocking of these kits and presence of first aid trained personnel. And (2) much of the medical care was delivered via team-doctoring, wherein teammates, with various degrees of medical knowledge and qualifications, would advise and treat their fellow teammates or others from inside the broader network of people connected to their sports. We make these conclusions confidently as an important feature of our sample's experiences in sport. However, the obvious constraints of our sample, in combination with the absence of a wider and current evidence base in relation to women's medical care in sport means that we offer only tentative implications from our findings.
We have specifically focussed on the experiences of women in this article. We were drawn to this in part because of our (pro)feminist proclivities, our academic and personal interests in sport and our reading of feminist and gender studies scholarship on sport. We broadly agree with Parsons et al.’s, (2021) call for a ‘gendered environment approach’ to women's injuries in sport. Yet our data speak to issues of underfunding and lack of resources in amateur sport more broadly. While gender might play a more or less important role in all people's lives, empirically it appears, in this dataset at least, that the paucity of resources, and/or the lack of motivation to direct them towards athletes’ medical care, were the clearest issues faced by the sportswomen we spoke with. Of course, this could be connected to gender issues in terms of the symbolic and material undervaluing of women's sport, but more research, especially that which takes a comparative approach, would be needed for us to make such a claim. With that in mind, we do not offer these findings as highlighting a distinctive problem for sportswomen in a general sense. Rather, we tentatively claim they speak more broadly to the ways that sportspeople, who operate in spaces where medical support is not readily accessible, might find themselves circulating ‘medical’ knowledge and delivering ‘medical’ care amongst themselves. And, as such, we call for further work to examine this in relation to the experiences of other populations.
We also take Charlesworth and Young (2005: 91) statement around similarities and differences between women's and men's experiences in sporting spaces very seriously. What we have shown here are the similarities. On the whole, we have highlighted how the experiences of these amateur sportswomen broadly align with the findings of malestream scholarship on the sociology of pain and injury in sport – that athletes often sacrifice their bodies and focus on performance largely over and above their short- and long-term health. In this way, sportswomen's attempts to ‘patch themselves up’, advise each other on managing injuries and sometimes deliver treatments, matches the physical sacrificing that Hughes and Coakley (1991) highlighted was a key feature of performance-orientated sport. Nonetheless, we think it is reasonable to expect that women might seek out same-sex teammates with whom to discuss specific women's health related matters – think for example of issues that might be connected to menses and pregnancy – especially in sports which are still dominated by men in important ways (e.g., see Thorpe (2016) for a broad discussion around women's experiences of amenorrhoea). The contouring and content of such conversations deserve future study and would most likely highlight that despite women increasingly finding themselves playing sport ‘like the boys’, there are important biological and sociological factors which means their experiences are likely to be foundationally different in both amateur and professional sport.
These caveats being made, let us reiterate the main contributions of this work. Due to the increasing significance of sport in many women's lives, and the cultural expectations embedded in performance sport there are increasing opportunities for women to participate in the harmful, risky behaviours that dominate most performance-orientated sporting spaces (For a recent discussion around this in relation to equality in brain damage, please see Hardwicke et al., 2024a). We concur with others who have shown that seeking basic medical care from teammates can be a central feature of the way that pain and injury are normalised as ‘part of the game’ (AlHashmi and Matthews, 2022a, 2022b; Charlesworth and Young, 2005; Liston et al., 2016; Pike, 2004, 2005; Safai, 2003). In particular, Pike (2005) argues that: …the practice of health care support from within the sportsnet is compromised when those advising the ill or injured are themselves immersed in the same sporting social network, since it is often in their interests to have athletes return to sports participation as quickly as possible. (p. 6)
We have, then, presented partial insights into medical support and care in amateur women's sport. Previous work on this topic provides theoretical and some empirical details of this phenomenon (Charlesworth and Young, 2005; Pike, 2004, 2005). Here we widen and update the empirical support for these claims and we have strengthened recent theoretical contributions on ‘team-doctoring’ as discussed by AlHashmi and Matthews (2022a, 2022b). This is an important step in further understanding the medical provision (or lack thereof) which is commonplace in amateur women's sport, and perhaps amateur sport more broadly. This paper highlights the ways in which women used, shared and acted on ‘medical’ knowledge to help each other survive the routinised physical rigours of playing their sports. As such, we have added to what we believe to be an overwhelming body of research that clearly demonstrates how involvement in performance-orientated sport can break down, damage and sometimes destroy bodies as an accepted ‘part of the game’ (Atkinson and Young, 2008; Hoch, 1972; Matthews, 2021a; Matthews and Channon, 2016; Matthews and Maguire, 2019; Nixon, 1992; Smith, 1983). We encourage scholars to focus further attention towards this area as a means of developing, critiquing and advancing these initial observations.
Footnotes
Acknowledgements
This article has been through various iterations and reviewed in various excellent journals. We would like to thank all the reviewers and editors who offered thoughtful and considered guidance. And we would like to thank the women who gave their time to speak to DF, your generosity sits at the foundation of our attempts to make sport safer, more enjoyable and equitable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.