
Abstract
Measles remains endemic in Pakistan despite global vaccine efforts to prevent its transmission. This study sought to identify the patterns of measles cases in Pakistan, understand the reasons for its recurrence, and determine the optimal timing for measles vaccine campaigns in Pakistan to be most effective. As such, a time series analysis of the monthly measles incidence in Pakistan from 2014 to 2024, obtained from World Health Organization’s international measles database, was performed to identify temporal patterns in infections. An increasing trend was identified in the monthly measles cases overtime, along with seasonal swings of low occurrences during the summer, with average lows reaching 304 cases, and a rise during the winter months, with average highs reaching 1038 cases. An automated Seasonal Auto-Regressive Integrated Moving Average (SARIMA) model was further applied to forecast the future incidence of measles, which revealed a three-fold increase in measles cases in the next two years, compared with 2023-2024. Low routine vaccine coverage, topped with climate change related migration and subsequent crowding in urban spaces were found to be major contributors to measles transmission in the country. Findings suggest that supplementary vaccination campaigns are essential and if held in August–September, can mitigate the anticipated rise in measles transmission beginning October every year.
What We Already Know
Pakistan is one of the few countries in the world where measles is endemic and frequent outbreaks occur.
The coverage of the measles vaccine remains low in the country.
Pakistan helped millions of children catch up with their measles vaccine through a successful 12-day measles and rubella vaccination campaign in November 2021.
What This Article Adds
An understanding of the temporal patterns in monthly measles cases in Pakistan and optimal timing for measles vaccination to be administered.
A forecast of future trends of measles cases.
A comprehensive understanding of why such patterns in measles cases exist.
Introduction
Measles is a particularly transmissible viral infection caused by a virus that belongs to the Paramyxoviridae family. 1 It spreads between humans through respiratory and airborne exposure, and direct contact with the nasal or oral discharge of the infected person. 1 Although generally harmless and manageable through medications and rest, measles can progress into respiratory failure, encephalitis, or death in rare cases. 1 Therefore, measles is unpredictable and poses a threat to individuals worldwide, especially to those who are pregnant, have a compromised immune system, and children less than 5 years old. 1
Fortunately, measles can be prevented through vaccination, which is recommended for children between the ages of 12 to 15 months for the first dose and between the ages of 18 months up until 6 years for the second dose. 1 For countries like Pakistan where the measles-containing vaccine (MCV) is used, it is recommended to give the first dose to ages 9 to 12 months and the second dose to ages 15 to 18 months. 2 However, population level immunity at a rate of ≥95% is required for preventing disease spread to a level that can eventually reach eradication.3,4 Global vaccination efforts through the World Health Organization’s (WHO) Expanded Programme on Immunization (EPI) have contributed to the prevention of 94 million cases of measles between 1975 and 2024. 5 However, low- and middle-income countries continue to bear the burden of measles infections 6 due to low routine and supplementary vaccine coverage 7 and malnourishment. 8
Pakistan tops as one of five countries in the world where measles remains endemic and annual outbreaks occur. 8 Furthermore, Pakistan has the second most unvaccinated children among nine countries supported by the United Nation International Children Emergency Funds (UNICEF) Regional Office for South Asia. 9 Although a large number of measles vaccines continue to be administered in the country through sporadic large-scale vaccine campaigns, routine vaccinations remain low.4,9 For instance, coverage of measles-containing vaccine 1 (MCV1) and 2 (MCV2) in Pakistan was only 76% and 45%, respectively, in 2017. 10
Since 2021, Pakistan has been witnessing a rise in measles infections. This is attributable to disruptions caused by the COVID-19 pandemic which not only prevented over 40 million children from getting their measles vaccines in 2020, but also more than 36 million children from receiving their routine vitamin A drops, a critical source of vitamin A for malnourished children in the country and an essential component of the body for fighting off infections.8,11 This was in addition to the population’s pre-existing vaccine hesitancy stemming from misconceptions about its effect on fertility and discord with alleged religious beliefs, as well as low health literacy and substandard health care which already contributed to low vaccine rates. 12 Without acquired immunity from vaccines and vitamin A supplementation, children faced high susceptibility to measles infections during the pandemic. 8
Nonetheless, Pakistan employed a massive 12-day measles and rubella vaccine campaign with the support of WHO, Global Alliance for vaccine and immunization (GAVI), and UNICEF in November 2021. 13 This resulted in 90 million children between the ages of 9 months to 15 years getting vaccinated, majority being those who attended school. 13
Despite the efforts of this supplementary immunization activity (SIA) in getting children caught up with their missed measles and rubella vaccines, significant gaps persist: routine vaccinations in the country remain low 4 and SIAs are not timed ideally to offer maximum benefit, especially given that they are time-consuming and resource intensive. 14 As unprecedented events continue to occur overtime, Pakistan will have to be prepared to implement SIAs in the form of vaccine campaigns to get children caught up with missed routine vaccines. Therefore, the overall goal of this study was to identify the optimal timing for measles vaccine campaigns in Pakistan to be most effective. This could be achieved through the following objectives:
Identifying temporal patterns in monthly measles cases in Pakistan from 2014 to 2024 by means of the Seasonal-Trend decomposition using LOESS (STL) algorithm.
Forecasting future trends in measles cases using an automated Seasonal Auto-Regressive Integrated Moving Average (SARIMA) model.
Recognizing possible reasons for current and future temporal patterns in measles cases.
Methods
National monthly measles incidence in Pakistan from January 2014 to December 2024 that were “lab-confirmed, epidemiologically linked, or clinically identified cases” according to WHO’s standard case definition, was acquired from the international measles database. 15 Analysis was delayed till the end of 2025 until all measles case counts for 2024, which were initially missing, were recorded to ensure completeness of data. Descriptive statistics were performed to understand the characteristics of the data. Furthermore, the data was decomposed into its predictable and unpredictable parts based on LOcally Estimated Smoothing Splines (LOESS), using the STL algorithm. A stationary seasonal pattern was explored using STL and visualized. A line plot visualized the average monthly measles case incidences in Pakistan. The year 2018 was excluded from this plot as it not only exhibited unusually higher case counts relative to other years, but its caseload exceeded those from the years right before and after it by a factor of 5 and 16, respectively. This was likely due to large measles outbreaks in Pakistan during that time.16,17 Therefore, the 2018 data was excluded as the seasonal pattern of that year would not be representative for any other year.
A Seasonal Auto-Regressive Integrated Moving Average (SARIMA) (0,1,0)(2,1,0) model was fit to the monthly incidence time series. An Augmented Dickey-Fuller (ADF) test was used to check for stationarity of the time series and confirm the seasonal differencing, prior to model fitting. To meet the normality and homoscedasticity assumptions, a log-transformation was also applied to the time series prior to SARIMA modeling. A QQ-plot and standardized residuals were used to check for model compliance with assumptions. Moreover, plots of the Autocorrelation Function (ACF) and Partial Autocorrelation Function (PACF) of the residuals, and the Ljung-Box test were used to check for autocorrelation between the remaining residuals and subsequently, the fit of the model. Finally, the SARIMA model was back-transformed with bias correction and used to forecast trends in measles incidence in Pakistan over the next 24 months. A timeline of 24 months into the future was chosen as time series are most accurate for short periods of time and therefore, the data analyzed in this paper is most reliable in predicting measles occurrence in the immediate future. All statistical analysis was performed using the forecast package 18 in R 19 and RStudio V. 4.0.2. 20
Results
A total of 132 monthly observations of national measles case counts in Pakistan over the 11-year period from 2014 to 2024 were recorded by WHO. 15 The highest reported monthly incidence of measles during this time in Pakistan was 6567 (May 2018), the lowest was 15 (September 2015), and 821 cases were observed on average.
The STL analysis and plot revealed an increasing linear trend in the data (Figure 1c), accompanied by annual seasonal swings that indicated a higher number of cases during the winter months of each year, and lower incidence in the summer (Figure 1b). Positive and negative spikes were observed in the remainder part, indicating the presence of leftover patterns not captured by the trend and season components (Figure 1d). The line graph of average monthly cases over a period of 11 years, excluding 2018, showed increasing incidences beginning from September and peaking in March (959 cases)and May (1038 cases). From there, the incidences gradually decreased, reaching a low in August (327 cases) and September (304 cases), and then started to rise again beginning October (Figure 2).
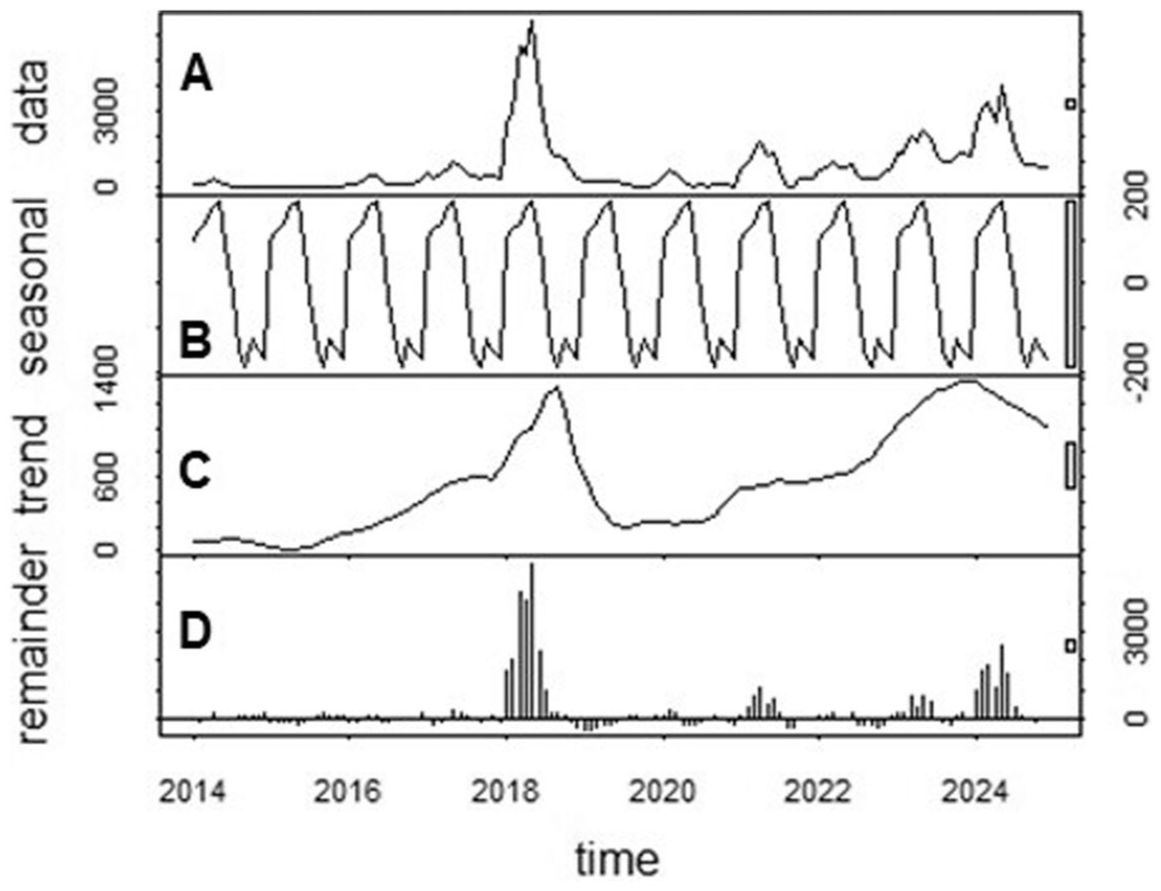
STL decomposition of measles cases in Pakistan from 2014 to 2024. (A) Data: discrete case counts; (B-D) Seasonal, Trend, Remainder: negative and positive deviations from average case counts (centered at zero).
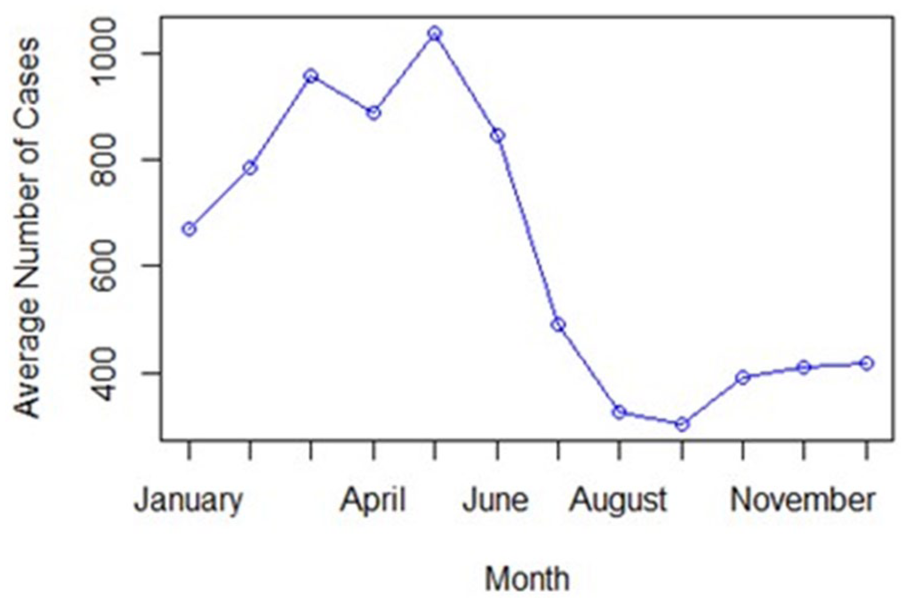
Visualization of the seasonal figure as estimated from monthly averages of measles incidence in Pakistan from 2014 to 2024 (excluding 2018).
Furthermore, a SARIMA (0,1,0)(2,1,0) model was fitted to the data, where the orders d=D=1 were informed by the STL analysis. Seasonal differencing was further confirmed using the ADF test (P = 0.21 > 0.05) which revealed non-stationarity of the time series, prior to model fitting. The orders p, d and P, D were identified by optimizing the Akaike Information Criterion (AIC) using an automated SARIMA modeling approach. The QQ plot of the scaled residuals indicated slight overdispersion of the residuals, suggesting that the model did not deviate too much from assumptions of normality and homoscedasticity. Further, inspection of the Box-Ljung test and the ACF and PACF at a lag of up to 24 months did not indicate a violation of the model’s assumptions.
Finally, measles cases in Pakistan were predicted to steadily increase over the next 24 months according to forecast patterns generated by the SARIMA model (Figure 3), with cases expected to total 123, 881 in 2025-2026. To assess the forecast accuracy of the SARIMA model, the forecast for 2023-2024 based on the 2014 to 2022 data were compared to the observed monthly case incidences. The forecast showed similar seasonal patterns to those observed, however they appeared to under-predict the actual observed values. The resulting root mean squared error (RMSE) suggested that predictions based on the model were off by ~728 cases.
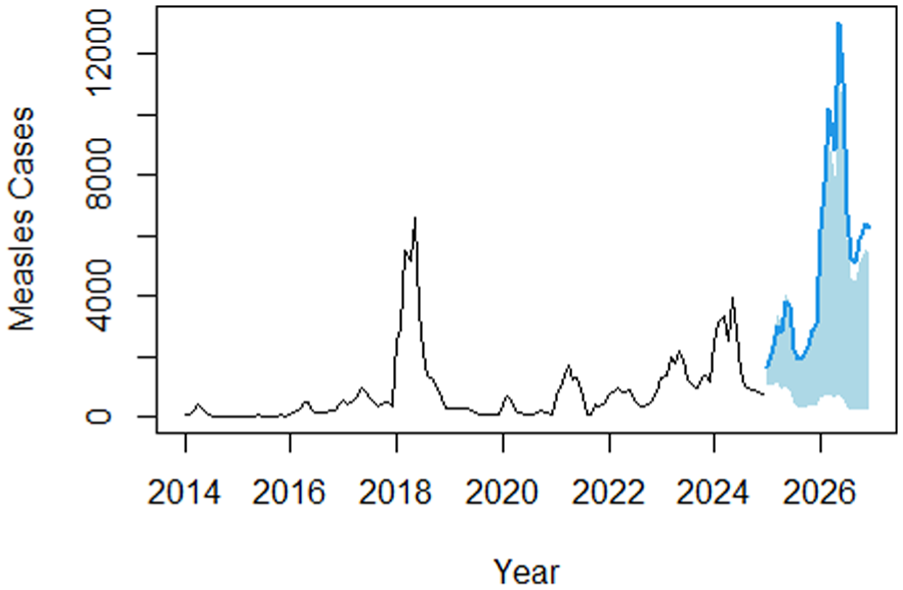
Forecast of measles incidence (number of measles case counts) for the years 2025 and 2026 using a SARIMA (0,1,0)(2,1,0) model.
Discussion
Time series analysis of measles data from Pakistan from 2014 to 2024 showed an increasing trend over the years and a seasonal swing exhibiting higher disease frequency during the winter months, beginning from the end of the year (October) to the middle of the next year (May). Without any interventions, these patterns are predicted to continue for the next two years, with the cumulative incidence increasing from 41 778 cases in 2023-2024 to 123, 881 cases in 2025-2026. This might still be an underestimation as predictions for 2023-2024 using the SARIMA model based on previous data although projected the seasonal pattern correctly, it predicted fewer cases than observed in reality. This was especially the case for 2024, a year otherwise hit by a large outbreak of measles in Pakistan due to low vaccinations combined with increased monsoon rains and scarce resources leftover post-COVID.11,21
Nonetheless, the results of this study are similar to those reported by other researchers who found seasonality present among the 2012-2017 measles cases in Pakistan. 14 They reported increased numbers of measles cases from October of one year into April of the next year and fewer cases between May to September, which coincides with Pakistan’s monsoon season. 14
Rationale for Seasonality in Measles Incidence
The seasonal pattern is arguably related to the annual rural-to-urban migration in Pakistan due to seasonal, occupational, agricultural, educational, and/or political reasons.14,22 In recent years, “climate-induced migration” has become one of the main contributors to domestic migration as a result of recurring floods, droughts, storms, and so on. 22 For instance, harsh winter conditions in the northern part of Pakistan such as in the province of Khyber Pakhtunkhwa and the Gilgit-Baltistan territory force people to find refuge in warmer cities.22,23 Conversely, some rural places are negatively impacted by extreme heat conditions in the wintertime, preventing individuals from being able to grow their winter crops and forcing them to migrate to urban areas. 24 Therefore, it is reasonable for most people to migrate to urban areas during the dry winter months where extreme cold and even heat in some provinces can disrupt agricultural practices and living conditions. Drought conditions in Pakistan’s desert areas during the months of March to June contribute to migration, 25 whereas heat stress in rural areas during the Rabi season from November to March causes migration. 26 Alternatively, some people migrate due to the leftover flooding from the monsoon rains that damage their crops and livelihoods during the summer season.25,27
Therefore, cases of measles are on the rise during the end of the year till the beginning of the next year as many people migrate into compacted urban areas. In fact, 50% of Pakistan’s population is expected to live in urban areas by 2030 due to climate related migration. 25 This will continue to put people at risk of infection as unvaccinated people from rural areas move into urban areas where measles transmission is higher. 7 This may also contribute to missed routine vaccinations among children as they are busy moving around. 6
Crowded spaces are major grounds for infectious diseases like measles to spread as they warrant many people to be in close contact with contaminated respiratory droplets and surfaces. 28 Additionally, measles can stay active in the air and on surfaces for 2 hours, 28 especially in low humidity and temperature settings. 29 This includes school settings and public transportation in Pakistan that are often overcrowded, improperly ventilated, and do not follow proper sanitary practices. 30
Therefore, it can be presumed that measles cases are lower during the summer when the air temperature and humidity is higher and children are out of school. However, the cases rise once children return back to school in September and interact with each other, especially while moving into the colder and less humid months of fall and winter that support the prolonged survival of the measles virus. This is quite likely as the majority of children that got vaccinated during Pakistan’s most recent measles campaign attended school, 13 suggesting that most school aged children miss their routine vaccinations and possibly contribute to measles outbreaks.
Optimal Timing for Measles Vaccine Campaigns
A previous study suggested that vaccine campaigns should occur in November as they can contribute to the prevention of approximately 440 000 more measles cases than can be prevented by a campaign run in January. 14 It also highlighted that the timing of the campaign should depend on the immensity of measles cases from the past year. 14 For instance, these authors suggested that if measles cases were quite high in 2017, the cases over the next year (2018) can be expected to be lower due to natural immunity and therefore, a vaccine campaign held later that year such as in November would be more effective in preventing an outbreak during the 2020 period when sufficient time has passed. 14
Unlike the previous study, we propose that vaccine campaigns should be held in August and September. This is because measles symptoms occur 7 to 21 days following infection. 1 Therefore, increased measles cases in October in Pakistan suggest that people may be getting exposed 1 to 3 weeks in advance in the previous month of September. Additionally, the measles vaccine takes about 2 to 3 weeks to produce antibodies in a person and protect them from infection. Therefore, if people are getting infected in September, vaccines administered in August and early September can elevate population immunity before students return to school and families migrate into crowded urban spaces, factors which have seemed to increase community transmission of the virus in the past. Additionally, since the two doses of the vaccine are recommended to be spaced by at least one month, 2 the months of August and September are suitable. While we have tried our best to propose what we deem as ideal timings for vaccine administration, we acknowledge that it is difficult for the country to access people in rural areas and therefore, opting for November and later months for vaccinations instead, when people have already moved into urban centers may be more feasible.
Limitations and Future Recommendations
A limitation of this study was the use of automated modeling which resulted in a SARIMA model that may be open to improvement. However, in a surveillance system, automated disease modeling is necessary to monitor and forecast a plethora of diseases simultaneously. Additionally, removing the 2018 dataset from the analysis may have potentially biased the results as it fails to represent the occurrence of a real epidemiological event. Thus, future predictions made using a model trained on “stable” case counts may not have been accurate in predicting future measles events, especially those that may be unexpected and/or extreme. This study also used measles case incidences from across Pakistan as a whole, whereas an analysis of individual provinces or territories may exhibit more insight into the temporal patterns of measles. Future studies should look at the measles incidence in individual provinces that may be disproportionately affected by climate change and might require differently timed vaccine campaigns.
More practical recommendations for the Pakistani public health system is to focus flood efforts not only on water clean-up activities but also on protecting health facilities by preventing physical barriers to their access, as well as the loss and destruction of paper-based patient health records. 21 The inability to access health centers and loss of medical records after a flood hinders people’s ability to seek care and receive vaccinations, as well as the system’s ability to identify those eligible for measles vaccination, respectively. 21 With the new gained knowledge about climate-induced migration, measles vaccine efforts should be integrated with disaster and climate preparedness.
Sporadic SIAs should continue to be prioritized in Pakistan as measles is expected to grow over the next 2 years. This can be done through public health efforts of educating the population on the importance of vaccines and collaborating with religious and community leaders to debunk widespread vaccine misinformation in the country. 12 Tracking children’s vaccine status in Pakistan is another important element to mitigate measles. 7
Moreover, SIAs for measles vaccinations should not only be prioritized for children in Pakistan, but also for adults, especially for those in high-risk areas such as crowded schools, buses, and workplaces. Finally, in addition to measles vaccinations, other routine vaccines for endemic illnesses in Pakistan such as those for polio and hepatitis should also be timed effectively.
Conclusion
In conclusion, measles poses an ongoing challenge to people in Pakistan as routine vaccine coverage remains low and extreme weather events due to climate change persist and push people into highly compacted urban settings. High rates of measles transmission and resulting caseloads during the winter and low caseloads in the summer months that have been witnessed since 2014 are expected to continue into 2026. Increased contact among children at the start of the school year and during urban migration events in the colder and dryer season is likely the cause of seasonal swings in measles cases in Pakistan. Therefore, in order for vaccine campaigns to be effective, they should be offered during the months of August and early September to offer maximum benefit and for the two doses to be spaced out by a month as recommended by WHO. These should be further combined with public health efforts of educating the population on the importance of vaccines, challenging widespread vaccine misinformation, improving vaccine tracking systems in the country to increase routine immunization, and prioritizing high-risk areas for vaccine administration.
Supplemental Material
sj-docx-1-aph-10.1177_10105395251415250 – Supplemental material for Time Series Forecasting of Measles Incidence in Pakistan, 2014–2024
Supplemental material, sj-docx-1-aph-10.1177_10105395251415250 for Time Series Forecasting of Measles Incidence in Pakistan, 2014–2024 by Aruba Adnan and Olaf Berke in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations and Informed Consent Statements
This article does not contain any studies with human or animal participants.
Consent for Publication
Not applicable.
Author Contributions
Aruba Adnan: Conceptualization, Methodology, Formal Analysis, Investigation, Data Curation, Writing – Original Draft.
Olaf Berke: Methodology, Resources, Data Curation, Supervision, Writing – Review and Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available in the World Health Organization Immunization Data Repository, https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fimmunizationdata.who.int%2Fdocs%2Flibrariesprovider21%2Fmeasles-and-rubella%2F404-table-web-epi-curve-data.xlsx%3Fsfvrsn%3D5922ebf7_6&wdOrigin=BROWSELINK.
Supplemental Material
Supplemental material for this article is available online.