
Abstract
The COVID-19 pandemic has led to severe restrictions on society worldwide, and social restrictions can lead to poor physical and oral health. This study investigated the association between oral disease symptoms and changes in lifestyle due to COVID-19. A multivariate logistic regression analysis was used to analyze data from the 2021 Korea Youth Risk Behavior Survey (N = 54 848). It showed that most households’ economic conditions as “did not change at all” (adjusted odds ratio [aOR] = 1.00), “no change” (aOR = 1.10), “slightly worsened” (aOR = 1.21), and “very worsened” (aOR = 1.24). Information in a with “did not change at all” (aOR = 1.00), “no change” (aOR = 1.13), “slightly worsened” (aOR = 1.15), and “very worsened” (aOR = 1.18) economic conditions experienced heightened gingival pain and bleeding. In conclusion, the COVID-19 pandemic has caused a change in lifestyle and worsened socioeconomic status. In addition, as lifestyle changed and socioeconomic status declined, symptoms of deteriorating dental health emerged.
What We Already Know
COVID-19 is a new infectious disease that has a profound impact on daily life.
Emerging infectious diseases have an adverse impact on the oral health of communities.
What This Article Adds
Among the total participants, 21.2% and 19.1% experienced tooth pain and gingival pain and bleeding, respectively.
A lot of research is being conducted on how to cope with body health in COVID-19 pandemic; however, there is less research conducted on how to cope with oral health.
Introduction
The coronavirus disease 2019 (COVID-19) outbreak is a global emergency, as it has caused significant disruption owing to its rapid spread and high mortality rate. The number of people infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19, has rapidly increased worldwide.1,2 Virtually all the Organizations for Economic Cooperation and Development (OECD) countries have been severely affected by the virus, and as part of the response to COVID-19, strict restrictions on social and economic life have been introduced, including social distancing and total lockdown. 3
Social distance, quarantine, and facility use restrictions have been implemented to prevent the occurrence and spread of COVID-19 pandemic. Furthermore, the restriction on work and school attendance has led to the introduction of telecommuting and online learning. 4 This closure and activity restriction increases psychological stress and deteriorates mental health. 5 Moreover, it negatively impacts the household economy.6,7
Lifestyle changes due to the COVID-19 pandemic have caused stress, affecting health directly or indirectly. Directly, it can cause physiological changes in bodily functions such as the nervous, endocrine, and immune systems. 8 Indirectly, stress can cause health problems by negatively affecting health-related behaviors such as smoking, drinking, exercise, and the use of medical services. 9 In addition, psychological stress is associated with oral diseases through impaired immune system function, increased stress hormones, increased caries-causing bacterial counts, and poor oral health.10,11 A previous systematic review has suggested a potential association between psychological stress, dental caries, and periodontitis. 12
Furthermore, the health inequality caused by the COVID-19 pandemic has significantly affected the vulnerable group. 13 Low socioeconomic conditions, stressful environments, low dental care use rates, and undesirable oral health–related behaviors have been reported as risk factors for toothache. 14 Higher health inequality was reported among those who lost income during the COVID-19 pandemic. 15 Moreover, people with poor socioeconomic status may not be able to afford the costs associated with good oral health, such as dental expenses, and previous research has shown that the lack of resources limits dental services. 16
However, limited studies have been conducted to identify lifestyle changes and symptoms of oral diseases caused by the COVID-19 pandemic. Therefore, this study aimed to identify the effect of lifestyle changes caused by COVID-19 on oral disease symptoms and the relationship between the main factors of lifestyle change and oral disease symptoms.
Methods
This study followed the Strengthening of the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 17
Data Source and Study Population
This study used data from the 17th Korea Youth Risk Behavior Web–based Survey (KYRBS) 2021, conducted by the Ministry of Education, Ministry of Health and Welfare, and Korea Centers for Disease Control and Prevention (KCDC). The KYRBS is an annual cross-sectional survey that collecting health information from Korean adolescents. The KYRBS selected 800 sample schools (400 middle and 400 high schools) using stratified cluster sampling to represent a nationally representative sample. The survey collected health information using an anonymous, self-administered online method. In the 2021 survey, 59 426 adolescents were selected. Among them, 54 848 participated (response rate = 92.9%). The KYRBS protocol was approved by the Institutional Review Board of the KCDC (2021-06EXP-02-P-A), and informed consent was obtained from all participants before they participated in the study. Further details can be found in studies conducted by Kim et al 18 and Bae et al. 19
General Characteristics
Identification of general characteristics included the following: (1) gender (male, female); (2) grade (middle school 1, 2, 3; high school 1, 2, 3); (3) household income (high, middle, low); (4) academic achievement (high, middle, low); (5) type of residence (living with family, living with relatives, living alone, dormitory, childcare facility); (6) father’s education (middle school, high school, college); and (7) mother’s education (middle school, high school, college).
Life Changes Due to the COVID-19 Pandemic
Changes in health behavior and household economy due to COVID-19 pandemic included the following: changes in physical activity (decrease, no change, increase); skipping breakfast (decrease, no change, increase); alcohol consumption (decrease, no change, increase); smoking (decrease, no change, increase), depression (decrease, no change, increase); household income change (did not change at all, no change, slightly worsened, very worsened).
Symptoms of Oral Disease Within the Last 12 Months
Oral disease symptoms, such as tooth pain, gingival pain, and bleeding, were examined. Tooth pain was evaluated as follows: “Did you have a sore, throbbing, or painful tooth in the last 12 months?” (“Yes” or “No”). In addition, gingival pain and bleeding were identified by asking, “Have your gums been sore or bled in the past 12 months?” (“Yes” or “No”). Finally, patients who answered “Yes” to both questions were identified as having experienced tooth pain, gingival pain, or bleeding symptoms.
Statistical Analysis
SPSS 26.0 (IBM Corp, Armonk, New York), a statistical analysis program, was used to analyze the collected data. The study used frequency and percentage to express changes in life due to the COVID-19 pandemic, the experience of oral disease symptoms, and the general characteristics of the study participants. A chi-square test was conducted to determine the ratio of those experiencing oral disease symptoms according to the characteristics of life changes caused by the COVID-19 pandemic and the participants’ general characteristics. Finally, a binomial multiple logistic regression analysis was performed to determine the characteristics of oral diseases related to lifestyle changes caused by the COVID-19 pandemic.
Results
Participant Characteristics
In total, the number of participants was 54 848. Among them, 51.7% were male and 48.3% were female. There were 17.0%, 17.8%, and 16.2% participants in grades first, second, and third middle schools grades, respectively. In addition, there were 15.6%, 16.6%, and 16.8% participants in the first, second, and third high school grades, respectively. As for the family economic status, there were 37.1%, 31.0%, and 31.9% participants in the upper, middle, and lower categories, respectively, and in terms of academic performance, there were 40.1%, 49.0%, and 10.9% participants in the upper, middle, and lower categories, respectively.
Oral Disease Symptoms (Tooth Pain, Gingival Pain, or Bleeding) Based on General Characteristics
Table 1 describes the symptoms of oral disease based on general characteristics. The results—24.7% of females experienced dental pain and academic performance (high [19.4%], average [22.4%], and low [27.4%])—were statistically significant (P < .001).
Oral Disease Symptoms by General Characteristics.
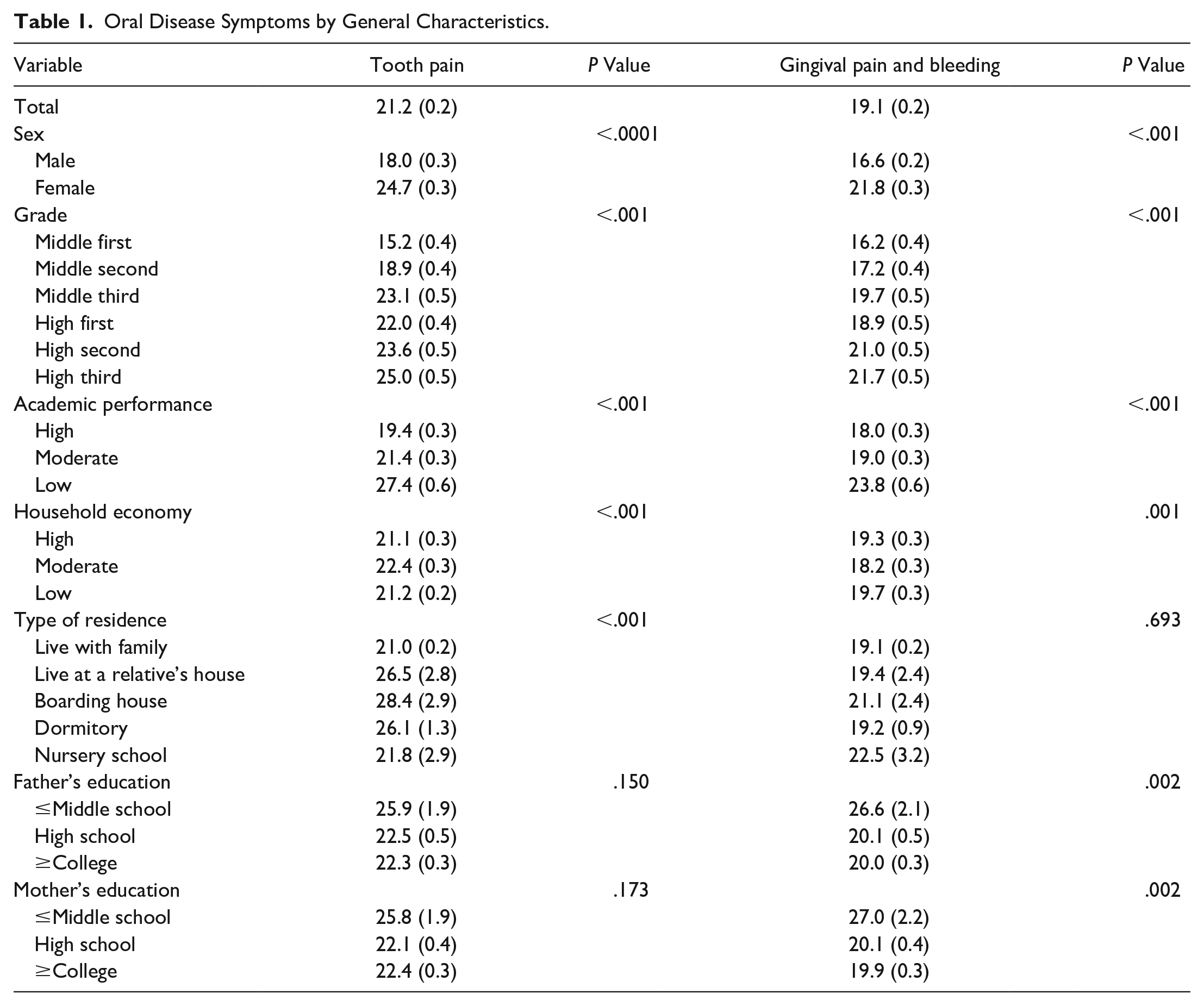
According to general characteristics, the rates of gingival pain and bleeding among males and females were 16.6% and 21.8%, respectively, and the rates of high, average, and low academic performance were 18.0%, 19.0%, and 23.8%, respectively. Furthermore, results on (add phrase) sex (P < .001), grade (P < .001), academic performance (P < .001), household income (P = .001), fathers’ education (P = .002), and mothers’ education (P = .002) were statistically significant.
Oral Disease Symptoms (Tooth Pain, Gingival Pain, or Bleeding) Base on Life Changes Due to the COVID-19 Pandemic
Table 2 describes the rates of oral disease symptoms experienced based on lifestyle changes due to COVID-19. The dental pain experience rate when physical activity “increased,” “no change,” and “decreased” was 17.8%, 18.1%, and 24.6%, respectively. Other results include skipping breakfast—increased (23.0%), no change (20.6%), and decreased (23.0%); drinking—increased (27.6%), no change (21.3%), and decreased (19.7%); smoking—increased (28.4%), no change (21.4%), and decreased (19.3%); depression—increased (28.2%), no change (17.2%), and decreased (16.9%); household economic status—very worsened (25.7%), slightly worsened (23.8%), no change (21.2%), and did not change at all (18.3%). The overall results showed statistically significant differences (P < .001).
Oral Disease Symptoms Based on Life Changes Due to COVID-19.
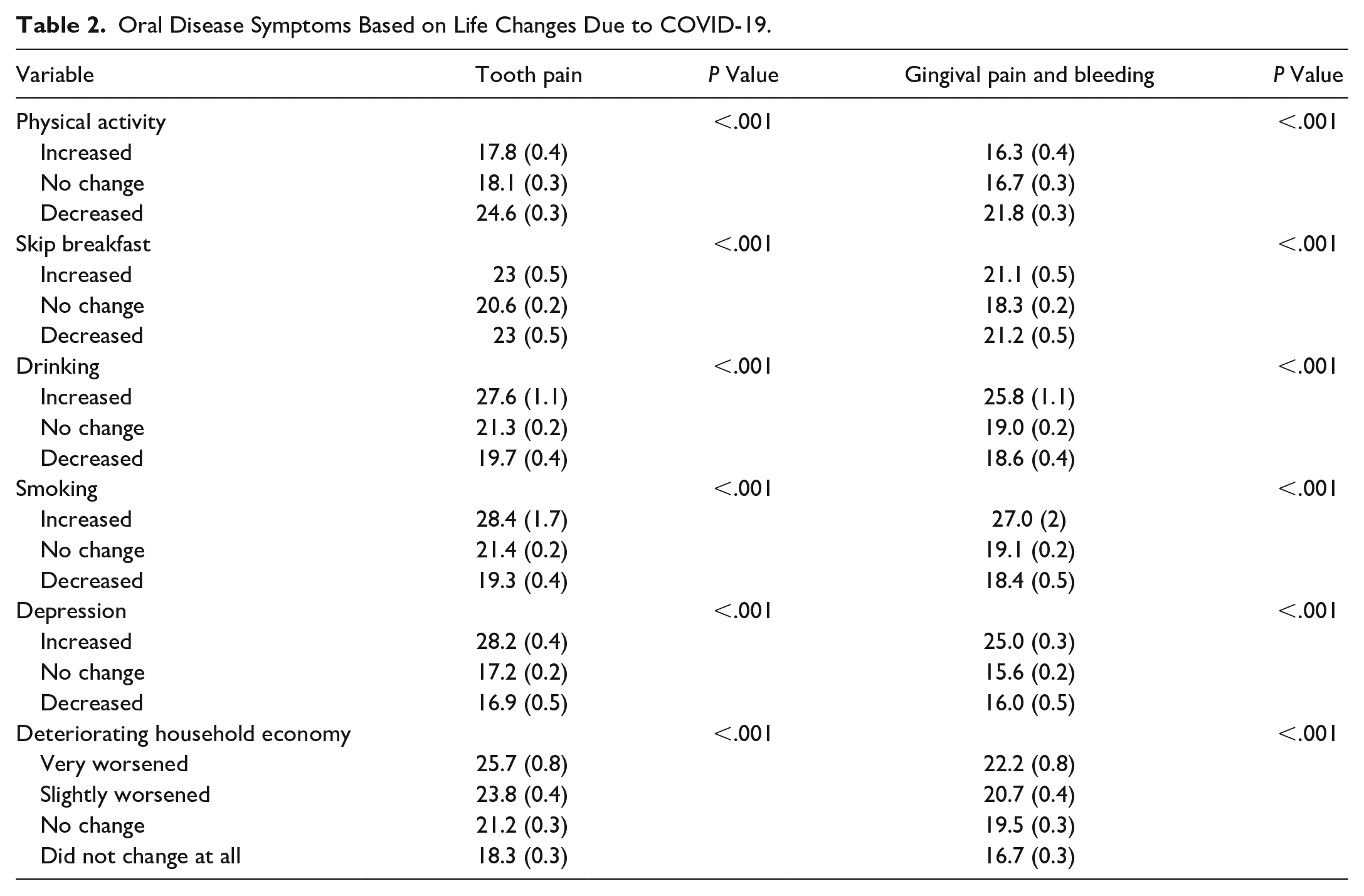
Gingival pain and bleeding experience rates were 16.3%, 16.7%, and 21.8% when physical activity increased, remained unchanged, and decreased, respectively. Other results include skipping breakfast—increased (21.1%), unchanged (18.3%), and decreased (21.2%); alcohol—increased (25.8%), no change (19.0%), and decreased (18.6%); smoking—increased (27.0%), no change (19.1%), and decreased (18.4%); depression—increased (25.0%), no change (15.6%), and decreased (16.0%). Household economic status displayed deterioration: very worsened (22.2%), slightly worsened (20.7%), no change (19.5%), and did not change at all (16.7%). All these results exhibited significant statistical differences (P < .001). Household economic status displayed disparities: 22.2% experienced a “very worsened” status, 20.7% faced a “slightly worsened” status, 19.5% observed “no change,” and 16.7% did not change at all, all of which exhibited significant statistical differences (P < .001).
Correlation Between Life Changes Caused by the COVID-19 Pandemic and Oral Disease Symptoms
Table 3 presents the logistic regression analysis results on the relationship between life changes and oral disease symptom experiences due to COVID-19.
Correlation Between Life Changes Caused by COVID-19 and Oral Disease Symptoms.
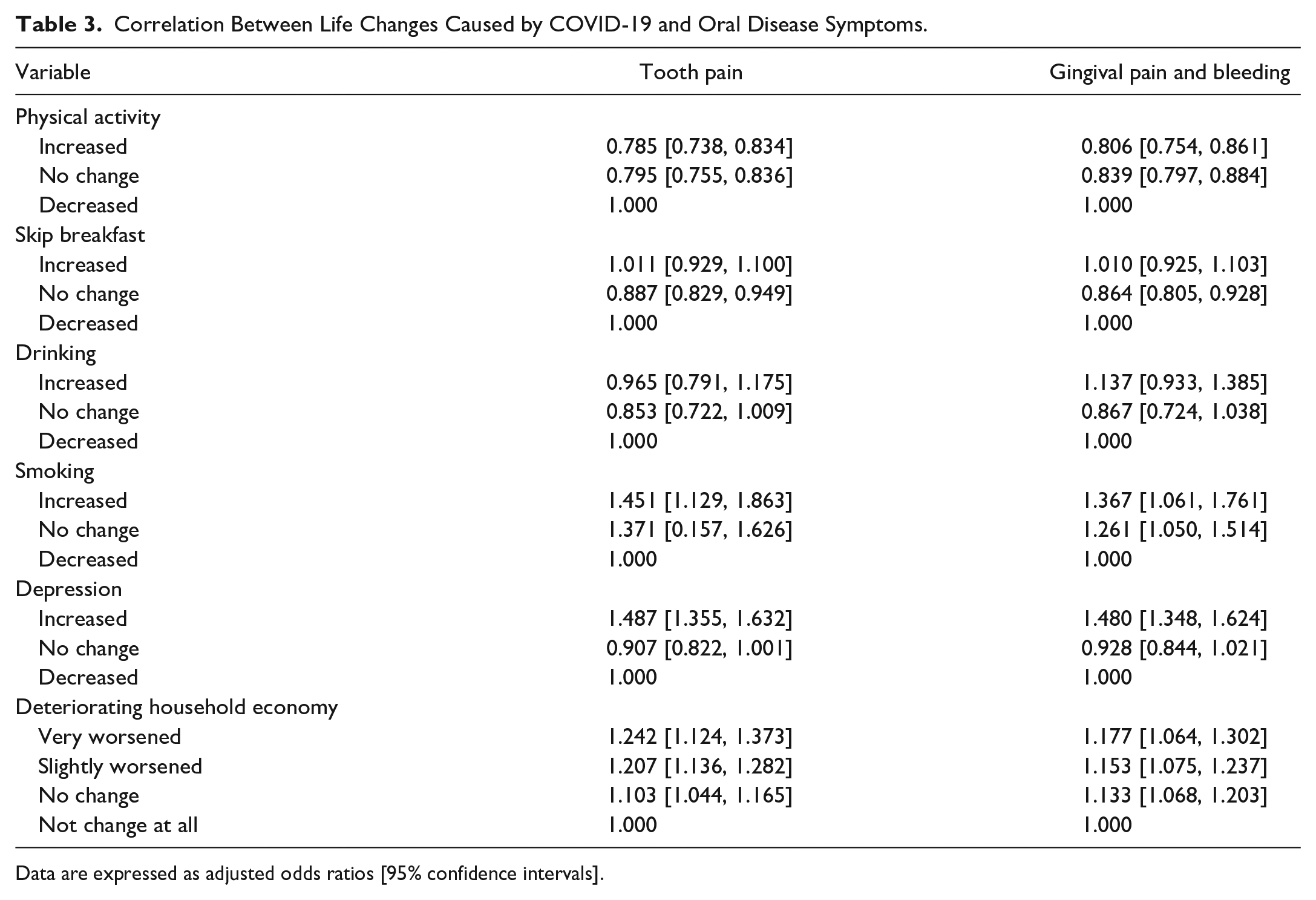
Data are expressed as adjusted odds ratios [95% confidence intervals].
The results of logistic regression analysis (adjusted sex, grade, academic performance, household economic status, and residence status) were significant as moderating variables to identify life changes are related to the experience of tooth pain. Tooth pain was less experienced when physical activity increased (aOR = 0.79, 95% confidence interval [CI] = [0.74, 0.83]) than when it decreased. However, more tooth pain was experienced when depression increased compared with when it decreased (aOR = 1.49, 95% CI = [1.36, 1.63]). Moreover, the results showed that the household’s economic condition “did not change at all” (aOR = 1.00), “no change” (aOR = 1.10, 95% CI = [1.04, 1.17]), “slightly worsened” (aOR = 1.21, 95% CI = [1.14, 1.28]), and “very worsened” (aOR = 1.24, 95% CI = [1.12, 1.37]). Tooth pain was experienced when the household’s economic status worsened. A logistic regression analysis determined the relationship between life changes caused by COVID-19 and gingival pain and bleeding using sex, grade, academic performance, household economic status, father’s education, and mother’s education as moderator variables, and the results were significant. The experience of gingival pain and bleeding was higher when depression increased (aOR = 1.48, 95% CI = [1.35, 1.62]) compared with when it decreased. In addition, the household’s economic condition “did not change at all” (aOR = 1.00), “no change” (aOR = 1.13, 95% CI = [1.07, 1.20]), “slightly worsened” (aOR = 1.15, 95% CI = [1.08, 1.24]), and “very worsened” (aOR = 1.18, 95% CI = [1.06, 1.30]). More gingival pain and bleeding were experienced when the household’s economic condition worsened.
Discussion
Various strategies, including social distancing and contact tracing, have been implemented worldwide to prevent the outbreak and spread of COVID-19 worldwide. Pandemics of emerging infectious diseases are known to cause health problems not only for patients but also for the entire community. It can also cause various life changes, such as deteriorating the family economy. These changes have directly or indirectly contributed to dental problems. Therefore, this study aimed to determine the impact of lifestyle changes caused by COVID-19 on the experience of oral disease symptoms.
In this study, 21.2% of the participants experienced dental pain during the COVID-19 pandemic, whereas 19.1% experienced gingival pain and bleeding. These results are consistent with the findings of previous studies that examined dental conditions during the COVID-19 pandemic. COVID-19 patients have reported a high prevalence of taste dysfunction, xerostomia, salivary gland disease, inflammatory reactions of the tongue, recurrent herpetic stomatitis in the palate with a sore throat, and blisters on the inner mucosa with exfoliative gingivitis. Furthermore, necrotic gingival papillae with unexplained gingival hemorrhage, ulceration of the tongue, erythematous lesions of the buccal mucosa of the lips, and erosion have also been reported. 20
These results suggest that COVID-19 can cause a variety of oral health problems. As a result of the prolonged COVID-19 pandemic, communities may experience severe long-term oral health consequences, and policymakers and oral health service providers should strive to continuously monitor oral health and provide subscriptions to support those in need.
In this study, tooth pain, gingival pain, and bleeding symptoms were significantly higher with increased depression. These results are consistent with previous studies that found that people undergoing depression have a higher risk of experiencing an oral disease. Psychological factors such as loneliness or social isolation are significantly associated with poor oral health-related quality of life and the development of oral health disease symptoms. 21 In addition, these results are similar to previous studies that claimed an increase in anxiety and depression during the COVID-19 pandemic may increase the prevalence of orofacial pain and temporomandibular disorders in the future. 22
Furthermore, the participants in this study experienced more symptoms of tooth pain, gingival pain, and bleeding when household income decreased compared with before the COVID-19 pandemic. This finding is similar to a study that found the negative economic impact of the COVID-19 pandemic may increase dental pain. 14 Since the start of the COVID-19 pandemic, dental visits have been postponed due to several patient-related factors. It was found that lower household income has a significant impact on visits to the dentist. 23 Moreover, the COVID-19 pandemic has greatly affected people’s economic situation. 23 Therefore, deteriorating household income triggered by the COVID-19 pandemic can contribute to postponed dental visits. This postponement might potentially result in toothaches and bleeding gums, indicative of dental issues. Nevertheless, due to the cross-sectional nature of this study, additional research is imperative to establish causal links between COVID-19-related life changes and dental ailment symptoms. Furthermore, it is necessary to study oral health problems according to various life changes caused by the COVID-19 pandemic.
This study has a limitation in using KYRBS data. The KYRBS collected health information in a self-reported manner. Thus, social desirability might have caused underestimation of life changes and dental disease symptoms.
Conclusion
This study explored diverse elements, including general traits and life alterations, that may influence dental ailment symptoms such as tooth pain, gingival discomfort, and bleeding after the COVID-19 pandemic. Findings reveal heightened rates of depression and reduced household income in the aftermath of the pandemic. Moreover, a notable association emerged whereby instances of toothache, gum pain, and bleeding symptoms were more prevalent amid decreased household income. The outcomes of this study offer valuable insights into the transformation of life circumstances and oral health practices in the face of emerging infectious diseases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.