
Abstract
This study examined quitting behavior and use of cessation aids (CAs) among Malaysian adult smokers aged ≥18 years (n = 1,047). Data were from the 2020 International Tobacco Control (ITC) Malaysia Survey were analyzed. A total of 79.9% of Malaysian smokers attempted to quit in the past 12 months and 85.2% intended to quit in the next 6 months. The most common CAs were e-cigarettes (ECs) (61.4%), medication/nicotine replacement therapies (NRTs; 51.0%), and printed materials (36.7%); the least common CA was infoline/quitline services (8.1%). Multivariable logistic regression analysis was performed to examine the association between sociodemographic variables and CAs use. Male smokers were more likely to use infoline/quitline services (adjusted odds ratio [aOR] = 3.27; P = .034). Malay smokers were more likely to use infoline/quitline services (aOR = 3.36; P = .002), ECs (aOR = 1.90; P = .004), printed materials (aOR = 1.79; P = .009), and in-person services (aOR = 1.75; P = .043). Most Malaysian smokers wanted to quit smoking. Furthermore, ECs were the most popular CAs, highlighting the need to assess the effectiveness of ECs for quitting smoking in Malaysia.
What We Already Know
Prevalence of smoking among Malaysian adults has plateaued over the past decade.
Most smokers are interested in quitting smoking. However, smoking is a complex behavior that is difficult to break due to nicotine addiction.
Use of cessation aids (CAs) can significantly increase the likelihood of quit intentions and successful quitting; however, the use of these CAs differs by sociodemographic factors.
What This Article Adds
The most common CAs were e-cigarettes (ECs; 61.4%), medication/nicotine replacement therapies (NRTs; 51.0%), and printed materials (36.7%).
Male smokers were more likely to have used infoline/quitline as a CA in their last quit attempt. Malay smokers were more likely to use infoline/quitline services, ECs, printed materials, and in-person services. No difference was found in the use of CAs by age and marital status.
ECs were the most popular CAs, highlighting the need to assess the effectiveness of ECs for quitting smoking in Malaysia.
Introduction
Tobacco smoking imposes enormous costs on global health and well-being. Worldwide, about 1.3 billion people smoke tobacco and more than 8 million people die from smoking each year. 1 In Malaysia, similar to many other Southeast Asian countries, smoking continues to be the leading cause of preventable morbidity and mortality, causing an estimated 27,200 deaths per year. 2 The high smoking rates have remained stable over the past decade. 3 In 2019, 4.8 million Malaysians aged 15 years and older were smokers, with men being much more likely to smoke (40.5%) than women (1.2%). 3
Smoking cessation, ranging from evidence-based recommendations (e.g., NRTs) to globally affordable health care interventions (e.g., brief advice from a health care provider (HCP), telephone helplines, printed self-help materials), 4 is essential in curbing smoking-related morbidity and mortality. Article 14 of the World Health Organization (WHO) Framework Convention on Tobacco Control (FCTC) obligates parties to implement measures that promote tobacco cessation and the treatment of tobacco dependence. 5 Malaysia ratified the FCTC in 2005 and has created national cessation guidelines in accordance with Article 14. 6 Public health clinics offer comprehensive services, including medications and counseling. National anti-smoking media campaign was initiated in 2004 and the nationwide mQuit quitline was revitalized in 2015. 6 Infolines and pictorial health warnings are printed on cigarette packs to discourage smoking. Despite these efforts, the high prevalence of smoking in Malaysia (around 20%) has not changed significantly. 3
Most smokers are interested in quitting smoking.7,8 However, quitting is very difficult, primarily because of the high addictiveness of cigarettes. 9 Among smokers who attempt to quit, only 10% achieve long-term smoking abstinence.7,9 Although numerous high-income countries (HICs) have shown an increase in the use of CAs among smokers, 10 there is limited evidence in low- and middle-income countries (LMICs). 11
In the past decade, ECs and heated tobacco products (HTPs) have become increasingly popular. Smokers who also use these products reported using them in their attempts to quit smoking.10,12,13 But nearly all of these studies have been conducted in HICs; there are almost no studies that have assessed the extent to which ECs and HTPs are being used as CAs in LMICs.
In a study of smokers in 15 ITC countries, including Malaysia, Borland et al 14 found that quit attempt rates and the type of CAs used varied widely, with pharmacotherapy being used more frequently than behavioral support. Other studies have shown that a combination of cessation pharmacotherapy and face-to-face behavioral support increases the effectiveness of cessation programs.15,16 Understanding quitting behavior, characteristics of smokers, and their use of CAs, can assist health practitioners in supporting potential quitters and policymakers in developing more effective smoking cessation programmes. The objective of this study is to examine quit intentions, quit attempts, and the use of various CAs, including ECs and HTPs among Malaysian adult smokers.
Methods
Study Sample
The 2020 International Tobacco Control Malaysia Project (ITC MYS1) Survey was conducted in February-March 2020 among 1,253 adult respondents (1,047 cigarette smokers and 206 non-smokers) aged 18 years and older. Malaysian respondents were recruited from Rakuten Insight’s web panel, which was representative of the population of adult smokers and non-smokers who have internet access. 17 About 88% of Malaysians had access to the internet in 2020. 18 A detailed description of the study is reported elsewhere.17,19 This study on cessation was restricted to the 1,047 current cigarette smokers. Smokers in ITC MYS1 Survey were defined as those who smoked at least monthly and had smoked 100 or more cigarettes in their lifetime. All respondents provided informed consent prior to completing the web survey. The survey received ethical clearance from the Research Ethics Board, University of Waterloo (ORE no. 40825), and the Medical Research Ethics Committee, University of Malaya (MREC ID no. 2019118-8018).
Measurements
Sociodemographic and smoking type variables
Sociodemographic variables were sex, age, marital status, ethnicity, and education. Respondents were grouped into four age groups: 18 to 24, 25 to 39, 40 to 54, and 55+ years for descriptive statistical analysis. Education was grouped into three categories: low (upper secondary and below), moderate (diploma certificate), and high (university and higher). Daily and non-daily (weekly and monthly) smokers were asked about cigarette consumption.
Quitting behavior
Respondents who had ever made any quit attempt were asked, “How many quit attempts have you made in the last 12 months?” This was a continuous variable, and it was dichotomized into “no attempt” versus “any attempt.” To measure intention to quit, respondents were asked, “Are you planning to quit smoking . . ?” and the responses were (1) “Within the next month,” (2) “Between 1-6 months from now,” (3) “Beyond 6 months,” and (4) “Not planning to quit.” Intention to quit was dichotomized to “yes” (within the next month and 1 to 6 months) and “no” (beyond 6 months and no plan to quit).
Use of CAs
Smokers were asked to list the CAs that they had used in their last quit attempt: “Which of the following products and services did you use as part of your last quit attempt?” Response options were “Yes,” “No,” “Refused,” or “Don’t know.” Each of these CAs was recoded as “yes” versus “no” to indicate whether respondents had used it or not, respectively. Non-responses (refused and don’t know) were treated as missing data. The CAs were put into nine categories, that is, (1) medication/NRTs, (2) infoline/quitline services, (3) local in-person services, (4) online services, (5) mobile apps, (6) ECs, (7) HTPs, (8) printed materials, and (9) received advice from a HCP (see Supplemental Table S1). A CA score was constructed by counting the number of CAs a smoker used, resulting in a CA score that ranged from 0 to 9. This was also recoded into a dichotomous variable of 1 = Single CA use and 2 = Multiple CA use (two or more CAs used).
Advice from HCPs
Smokers were asked whether they had received “Face-to-face advice from a doctor or other health care providers such as a nurse, dentist, pharmacist as part of a cessation service in your
Statistical Analyses
Data were analyzed in SPSS Complex Samples Software (Version 23.0) to account for the stratified design and sampling weights. Weighted percentages were calculated with 95% confidence intervals for proportions (Tables 1 and 2 and Supplemental Table S2). Subgroup analyses for CAs were performed by sex, education, age, marital status, ethnicity, smoking status, and quit intention (Table 2). For Table 3, univariable models were used to assess the association between each predictor (independent variable) and each type of CA used (dependent variable). A multivariable logistic model was then fitted to control for sex, age, ethnicity, and education as they are the core variables that were used to construct the survey weights. Results are presented in Table 3 as adjusted odds ratios (aORs) with 95% confidence intervals.
Sociodemographic Characteristics and Smoking Behaviors of Adult Malaysian Smokers (Weighted).
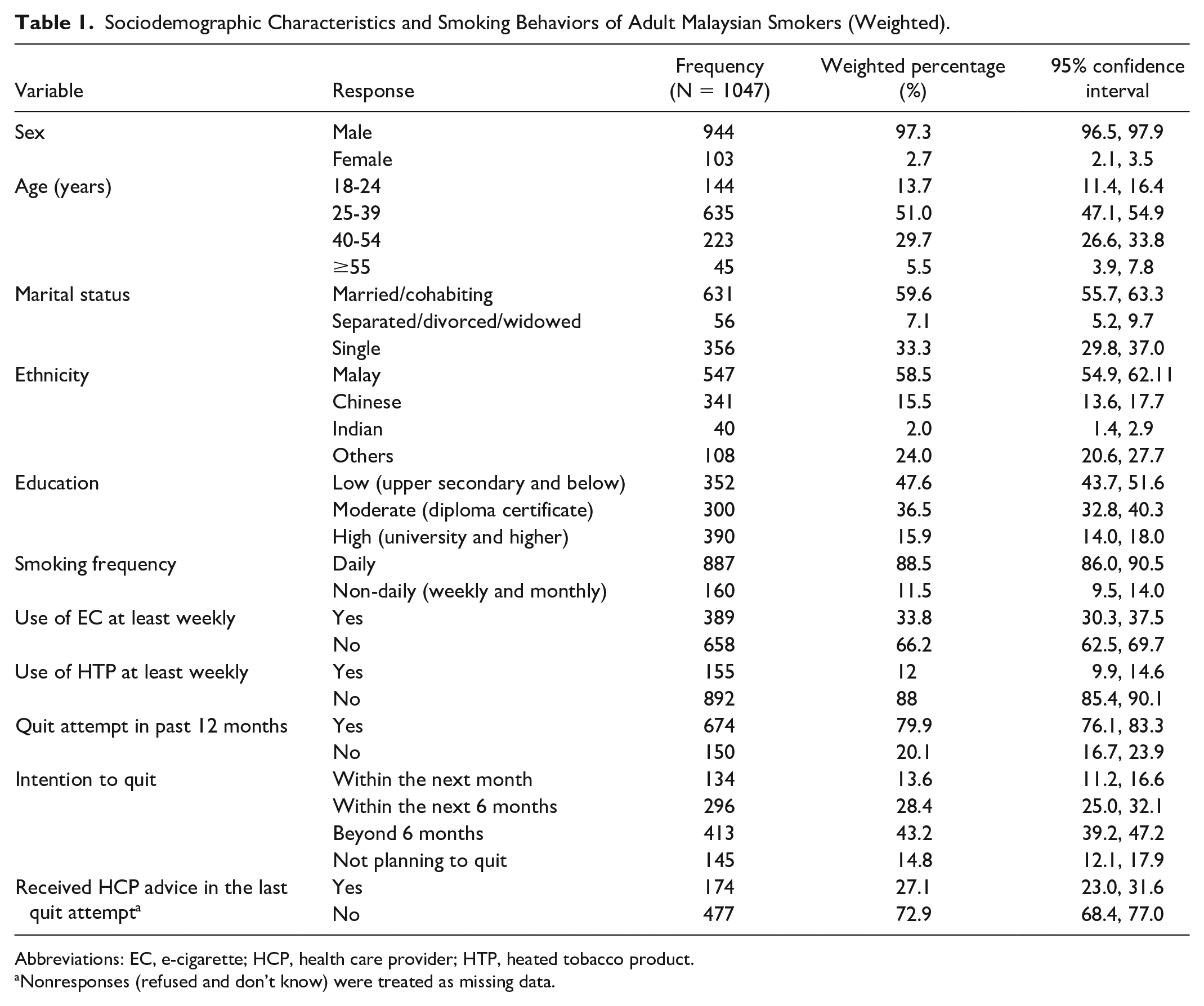
Abbreviations: EC, e-cigarette; HCP, health care provider; HTP, heated tobacco product.
Nonresponses (refused and don’t know) were treated as missing data.
Reported Overall and Stratified Analyses by Subgroups on Reported Use of Cessation Aids Among Adult Smokers in Malaysia Who Reported Having Attempted to Quit in the Past 12 Months (Weighted Results).
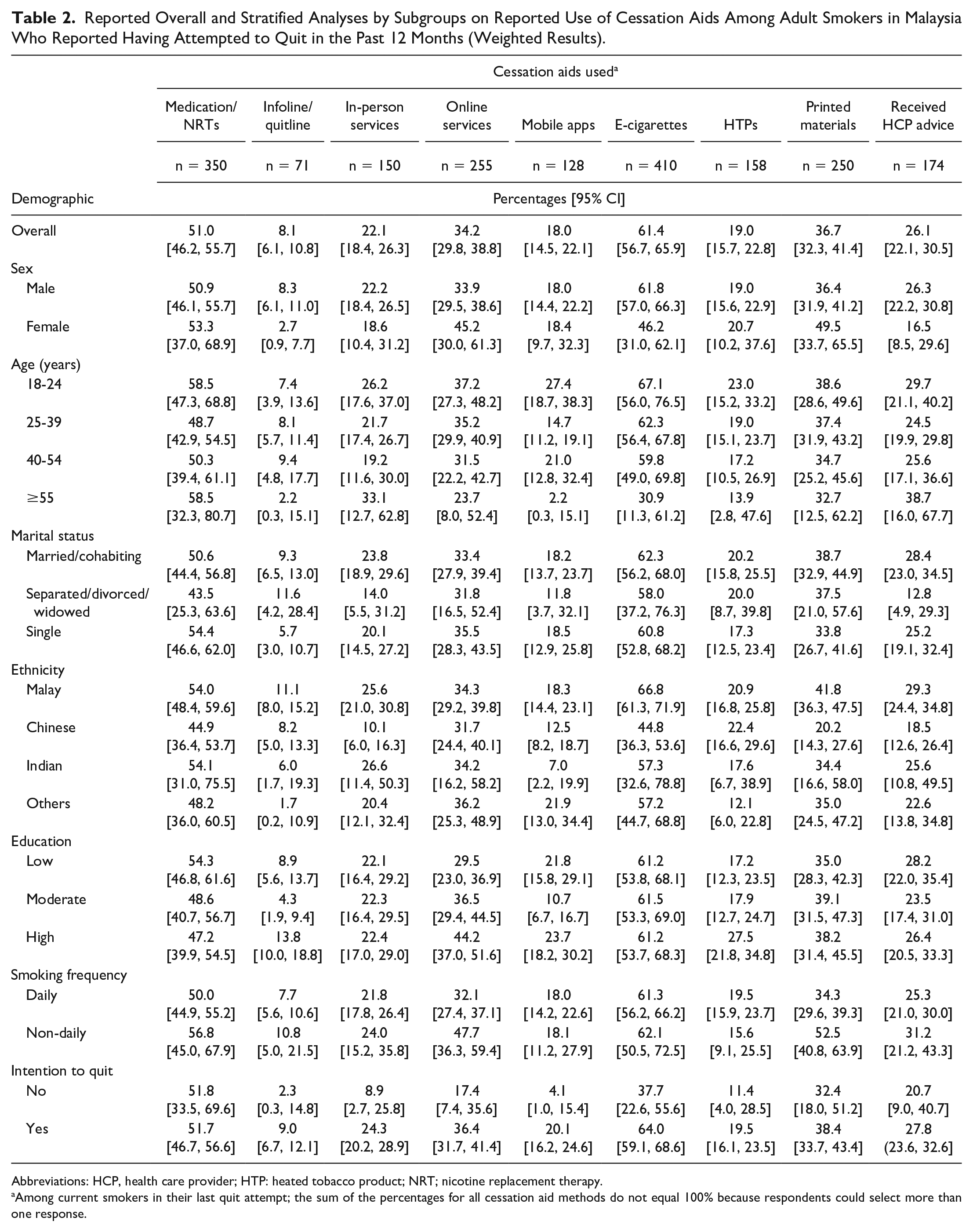
Abbreviations: HCP, health care provider; HTP: heated tobacco product; NRT; nicotine replacement therapy.
Among current smokers in their last quit attempt; the sum of the percentages for all cessation aid methods do not equal 100% because respondents could select more than one response.
Logistic Regression Models of the Association Between Reported Cessation Aids and Sociodemographic Variables Among Adult Smokers in Malaysia.
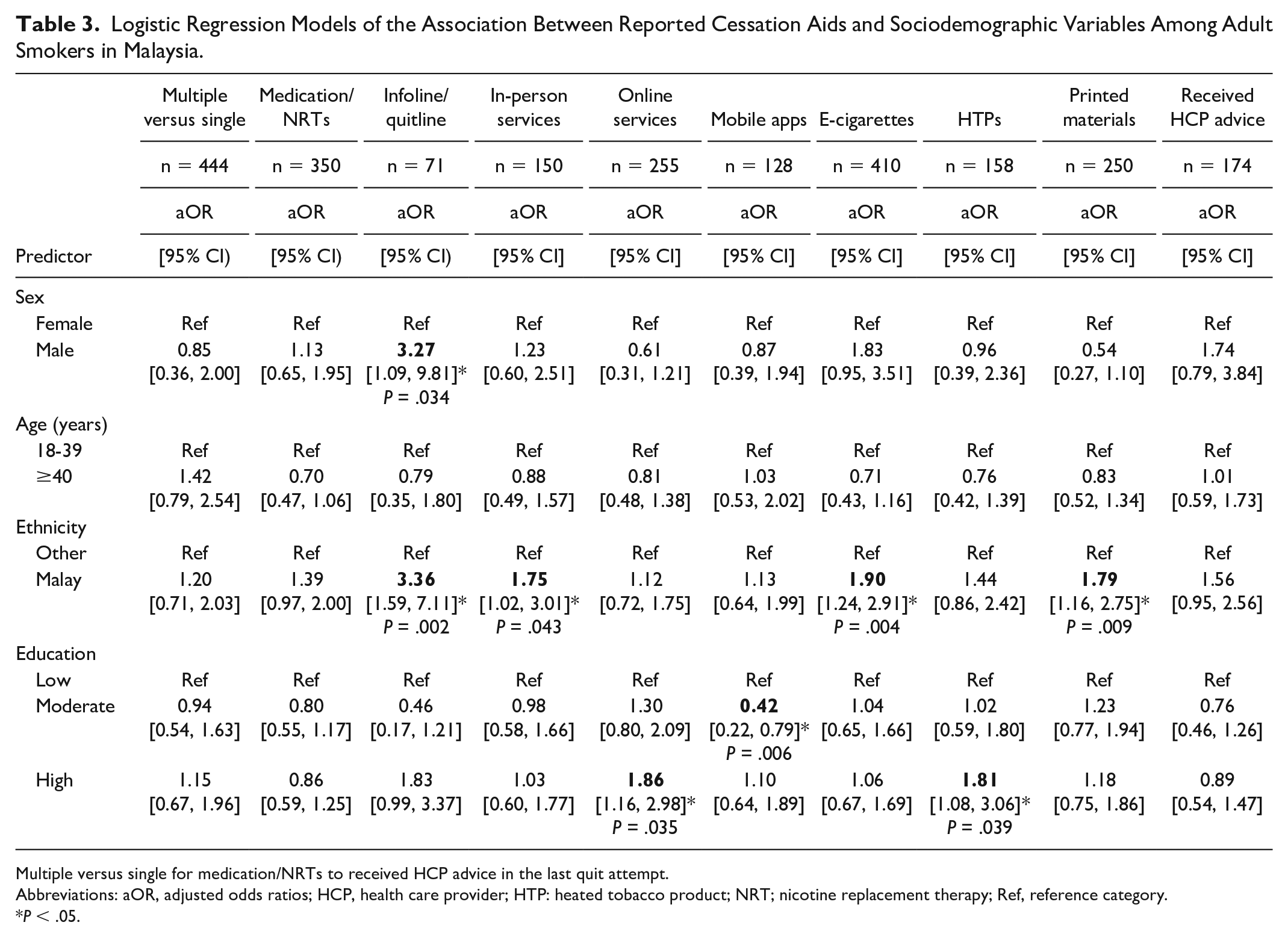
Multiple versus single for medication/NRTs to received HCP advice in the last quit attempt.
Abbreviations: aOR, adjusted odds ratios; HCP, health care provider; HTP: heated tobacco product; NRT; nicotine replacement therapy; Ref, reference category.
P < .05.
Results
Sample Characteristics
Table 1 shows the sociodemographic characteristics and smoking behaviors of adult Malaysian smokers. Most smokers were males (97.3%), aged 25 to 39 years (51.0%), married or cohabiting (59.6%), and of Malay ethnicity (58.5%). About half of the smokers had an upper secondary education, and a quarter had a higher education (such as a university degree). A majority of the adult Malaysian smokers were daily smokers. Most smokers (79.9%) reported making a quit attempt in the past 12 months, whereas 85.2% of smokers planned to do so in the near future. Less than a third (27.1%) of the smokers reported receiving advice from a HCP as part of their last quit attempt.
Quitting behavior
Supplemental Table S2 presents the percentage of smokers who reported having made a quit attempt in the past 12 months and had an intention to quit. Young smokers aged 18 to 24 years, single, Malay, and other ethnicities, and those with a high level of education reported the highest number of quit attempts in the past 12 months. Most smokers reported having a quit intention, with the highest intention reported “beyond 6 months.” In each category, those who reported higher intention to quit within 1 to 6 months were women, aged 25 to 39 years, married/cohabiting, Malay, and those with a high level of education. More than one third (34.6%) of smokers aged 55 years and older reported that they were not planning to give up smoking.
Use of CAs
Table 2 shows the percentages of smokers who reported using CAs (i.e., medication/NRT, infoline/quitline services, local in-person services, online services, mobile apps, ECs, HTPs, printed materials, and advice from HCP) in their last quit attempt. Usage of CAs were further stratified by sex, age, marital status, ethnicity, and education. Most smokers used ECs (61.4%), medication/NRTs (51.0%), and printed materials (36.7%) in their last quit attempt. The least used CA was infoline/quitline services (8.1%).
The EC was the most popular CA among all subgroups except among women (46.2%) and those aged 55 years and older (30.9%). As a CA, HTPs were most frequent among smokers with high education (27.5%) and those aged 18 to 24 years (23.0%). Online services were most popular among female smokers (45.2%) and those with high education (44.2%). Medication/NRT was most popular CA among smokers aged 18 to 24 years (58.5%) and 55 years and older (58.5%), single (54.4%), and those of Malay (54.0%) and Indian (54.1%) ethnicity. Local in-person services were mostly used by smokers aged 55 years and older (33.1%) and those aged 18 to 24 years (26.2%), whereas mobile apps were primarily utilized by smokers aged 18 to 24 years (27.4%) and those with high education (23.7%). Infoline/quitline services were least used overall but were mostly used by smokers with high education (13.8%) and those aged 40 to 54 years (9.4%).
Smokers with a high level of education reported the highest use of the following CAs in their last quit attempt: online services (44.2%), HTPs (27.5%), mobile apps (23.7%), in-person services (22.5%), and infoline/quitline (13.8%).
Sociodemographic factors associated with use of cessation aids
Table 3 presents the results from the logistic regression models. Male smokers were more likely to use infoline/quitline services (aOR = 3.27; P = .034). There were no differences in the use of CAs by age or marital status. Compared with non-Malay smokers, Malay smokers were likely to use infoline/quitline services (aOR = 3.36; P = .002), ECs (aOR = 1.90; P = .004), printed materials (aOR = 1.79; P = .009), and in-person services (aOR = 1.75; P = .043). Smokers with a moderate level of education were less likely to report using mobile apps (aOR = 0.42; P = .006) as a CA, whereas those with a high level of education were more likely to report using online services (aOR = 1.86; P = .035) and HTPs (aOR = 1.81; P = .039) in their last quit attempt.
Discussion
The findings from this study show that a majority of Malaysian smokers are interested in quitting smoking; 79.9% smokers (aged 18+ years) reported having made a quit attempt in the past 12 months, and 85.2% intended to quit smoking, which are among the highest across the 20+ ITC countries. 20 The quit attempt rate is notably higher than the findings from the 2019 National Health and Morbidity Survey (48.9%) 3 (for those aged 15 years and older) and quit attempts reported in other countries such as Australia (77%) 8 and Indonesia (43.8%). 21
As with other regional studies,3,22 Malaysian smokers with lower education warrant more support as they were least likely to intend to quit within the next six months. Improving existing smoking cessation infrastructure is important to meet the high demand for cessation assistance in Malaysia, which is vital for low-equity groups, such as those of low education and income, and also for younger smokers (aged 18-24 years) who reported the highest percentage (90.5%) of quit attempts in the past 12 months. Younger smokers were also more likely to use medication/NRTs, online services, mobile apps, ECs, and HTPs as discussed in further detail below.
Of the 85.2% smokers who intended to quit, 42% planned to quit within 6 months, which is much higher than Mauritius (28%), Mexico (24%), Thailand (19%), the same as Australia (42%), but lower than Brazil (48%). 23 In our study, smokers aged 55 years and older (55.1%) and smokers of Indian descent (58.6%) made fewer attempts to quit smoking. It is essential to provide health information about the risks and benefits of tobacco use to smokers who fit these demographic characteristics.
The use of available CAs in smokers’ last quit attempt was low to moderate except for EC use. This was surprising because smoking cessation clinics in government-funded primary health care centers and hospitals in Malaysia offer many CAs, including medication/NRTs and counseling services. A total of 51.0% of smokers reported using medication, and only 8.1% used infoline/quitline services. Infoline/quitline services have the opportunity to offer cost-effective cessation assistance with wide implementation scope. Despite high internet penetration in Malaysia, 18 these services may not be available to smokers who live in rural areas of the country. Information and communication technology (ICT) infrastructure needs to be made more accessible and affordable to support CAs through mobile apps and online services, apart from infoline/quitline.
The most popular CA by far was ECs, with 61.4% of smokers using ECs to quit smoking. A 2022 Cochrane Group systematic review on the use of ECs for smoking cessation, covering 78 studies (including 40 randomized clinical trials), concluded that there was “high-certainty evidence” that ECs with nicotine increase quit rates compared with NRTs and “moderate-certainty evidence” that ECs with nicotine increase quit rates compared with ECs without nicotine. 24 However, there should be caution in applying the conclusions of this systematic review to Malaysia and other LMICs, given that virtually all of the studies in the review were conducted in HICs.
The very high rate of EC use for quitting among smokers may reflect the general popularity of ECs in Malaysia, 25 but it may also reflect lower awareness or (possibly) lower availability of other CAs, including stop-smoking medications. Usage of ECs to quit was particularly high among young smokers in our study (67.1% for those aged 18-24 years), consistent with the findings of another study 26 where 57.8% university students in Malaysia reported using ECs as a CA. According to another ITC MYS1 study, 91.3% of Malaysian smokers who used ECs daily reported using them to reduce smoking and 87.9% to quit smoking. 27 However, in this study, there was no significant difference between those who had quit intentions and those who did not in the likelihood of their having used ECs at the last quit attempt. A primary motivation for EC use among smokers in Malaysia may be to replace cigarettes but not to quit smoking,13,27 and therefore high prevalence (74%) of dual users of cigarettes and EC has been reported in Malaysia. 28 As ECs have become increasingly popular and normalized in the general population in Malaysia, the role of ECs in smoking cessation in Malaysia needs to be investigated in future studies.
In contrast to the very high popularity of ECs use in quitting smoking, HTPs was one of the least prevalent CAs, with 19.0% of Malaysian smokers who had attempted to quit mentioning HTPs. This is likely due in large measure to the lower prevalence of HTPs (12.0%) compared with ECs (33.8%) among Malaysian smokers, which has also been detected in another ITC MYS1 study. 29 It will be important to track changes in EC and HTP use and their use in attempts to quit in Malaysia over time.
As 26.1% of smokers reported receiving HCP advice in their quit attempt effort, there is potential to enhance this service. The HCPs must be adequately trained to provide effective follow-up cessation services as they are in the best position to advise their patients to quit smoking. 30 It is also important for HCPs to focus and support smokers who do not intend to quit.
This study is the most extensive examination of quitting behavior, quit attempts, intentions to quit, and the use of various CAs, including how those cessation-relevant behaviors and aids vary by important demographic characteristics. An additional strength is the use of standardized quit behavior measures that have been used in 30 other ITC countries; thus, the results from this study can be compared with other similar ITC studies.
This study was also subjected to some limitations. Our study only included current smokers and may have underestimated the number of quit attempts and the use of CAs as successful quitters were not sampled. In addition, this cross-sectional study cannot determine the extent to which the associations among the predictor variables and outcome variables are causal. The study sample comprised a minority of women as a result of the relatively low incidence of female smoking in Malaysia. 3 As a consequence, caution must be exercised when attempting to interpret gender-based results. These limitations highlight the importance of longitudinal studies in the examination of the factors associated with cessation—a conclusion that is not limited, of course, to studies conducted in Malaysia.
Conclusion
A majority of Malaysian smokers want to quit smoking; indeed the percentage of Malaysian smokers who have attempted to quit in the past year (79.9%) and who intend to quit in the next 6 months (85.2%) are among the highest across more than 20 ITC countries. Various cessation methods have been used by Malaysian smokers, with ECs being the most popular. Malaysia needs to make greater efforts to assist its 4.8 million smokers to quit smoking.
Supplemental Material
sj-docx-1-aph-10.1177_10105395231220465 – Supplemental material for Intentions to Quit, Quit Attempts, and the Use of Cessation Aids Among Malaysian Adult Smokers: Findings From the 2020 ITC Malaysia Survey
Supplemental material, sj-docx-1-aph-10.1177_10105395231220465 for Intentions to Quit, Quit Attempts, and the Use of Cessation Aids Among Malaysian Adult Smokers: Findings From the 2020 ITC Malaysia Survey by Ina Sharyn Kamaludin, Lim Sin How, Anne Yee, Susan C. Kaai, Mi Yan, Mahmoud Danaee, Amer Siddiq Amer Nordin, Farizah Mohd Hairi, Nur Amani Ahmad Tajuddin, Siti Idayu Hasan, Anne C. K. Quah and Geoffrey T. Fong in Asia Pacific Journal of Public Health
Footnotes
Acknowledgements
The authors would like to acknowledge and thank all those who contributed to the ITC Malaysia Wave 1 Survey: all study investigators and collaborators, and the project staff at their respective institutions.
Author’s Note
Anne Yee is also affiliated to Clinical School Johor Bahru, Monash University Malaysia, Johor, Malaysia.
Author Contributions
ISK contributed to conceptualization, writing—original draft, formal analysis, and validation; writing—review and editing and project administration. LSH and AY contributed to supervision and writing—review and editing. SCK contributed to writing—original draft, formal analysis, and validation; writing—review and editing; and project management. MY contributed to formal analysis, validation, and writing—review and editing. MD, NAAT, and SIH contributed to writing—review and editing. ASAN contributed to funding acquisition, supervision, resources, and writing—review and editing. FMH contributed to supervision and writing—review and editing. ACKQ contributed to methodology, project administration, and writing—review and editing; and GTF contributed to funding acquisition, methodology, resources, writing—review and editing, and supervision. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GTF has served as an expert witness or consultant for governments defending their country’s policies or regulations in litigation and has served as a paid expert consultant to the Ministry of Health of Singapore in reviewing the evidence of plain/standardized packaging. ASAN has received an unconditional educational grant from Johnson & Johnson Malaysia Sdn. Bhd. All other authors have no conflict of interest to declare. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ITC Malaysia Project was funded by the Malaysia Ministry of Higher Education-LRGS NanoMITe (RU029-2014) and the University Malaya Research University Grant (RU029C-2014 and RU001A-2021) and the Canadian Institutes of Health Research Foundation Grant (FDN-148477). Additional support to GTF was provided by a Senior Investigator Award from the Ontario Institute for Cancer Research (IA-004).
Data Availability Statement
In each country participating in the International Tobacco Control Policy Evaluation Project, the data are jointly owned by the lead researcher(s) in that country and the ITC Project at the University of Waterloo. Data from the ITC Project are available to approved researchers 2 years after the date of issuance of cleaned data sets by the ITC Data Management Centre. Researchers interested in using ITC data are required to apply for approval by submitting an International Tobacco Control Data Repository (ITCDR) request application and subsequently to sign an ITCDR Data Usage Agreement. The criteria for data usage approval and the contents of the Data Usage Agreement are described online (![]() ; accessed July 29, 2022).
; accessed July 29, 2022).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.