
Abstract
Previous studies supported the association between insomnia symptoms and suicidal ideation in patients with mental or psychological diseases. This study aimed to examine the associations between insomnia symptoms, general self-efficacy, and suicidal ideation among community-based adult population. Standardized questionnaire was distributed to 2051 community-dwelling adults in Lishui district of Jiangsu Province in China, to assess their socio-demographics, insomnia symptoms, general self-efficacy, and suicidal ideation. Multiple binary logistic regression or linear regression and mediation analysis with bootstrap resampling method were performed. Results showed that the weighted prevalence of lifetime suicidal ideation was 6.38%. Insomnia symptom was associated with higher odds of suicidal ideation after adjusting for sociodemographics and mental health status (odds ratio [OR] = 2.85, and the OR of insomnia symptom with suicidal ideation decreased but remained significant after additionally adjusting for general self-efficacy (OR = 2.62). Participants with insomnia symptom were also significantly associated with lower general self-efficacy (β = −0.96), whereas higher general self-efficacy was associated with a lower odds of suicidal ideation (OR = 0.92). In conclusion, general self-efficacy was associated with both insomnia symptom and suicidal ideation among the community-dwelling adult population.
What We Already Know
Insomnia and suicidal ideation are common complaints among people with mental disorders.
Insomnia symptoms are associated with suicidal ideation in people with psychiatric disorders.
Self-efficacy has been previously reported as associated with multiple variables and suicidal ideation.
What This Article Adds
Suicidal ideation is a health threat prevalent among Chinese community-based population, especially during the COVID-19 pandemic.
Insomnia symptom is associated with higher odds of suicidal ideation, even in community populations.
General self-efficacy is associated with both insomnia symptom and suicidal ideation.
Introduction
Suicide leads to considerable numbers of deaths and disabilities worldwide, with an estimated report of up to 800 000 human lives lost due to suicide each year. 1 Although people do not always progress from ideation to suicidal behavior, suicidal ideation is highly common in countries including China,2,3 and it has been demonstrated in association with subsequent completed suicide in both psychiatric and nonpsychiatric populations. 4 Therefore, adequate identification and assessment of individuals potentially having suicidal ideation is essential to inform suicide prevention. In particular, evidence from both adolescent and adult samples has noted that elevated symptoms of anxiety, depression, insomnia, psychosis, and stress are key indicators in relation to suicidal ideation, 5 indicating the necessity of more focused research into the link between suicidal ideation and psychological-related problems such as insomnia.
Previous literature documented that insomnia was associated with suicidal ideation in patients with psychiatric diagnoses (e.g., patients with depression, posttraumatic stress disorder, panic disorder, or schizophrenia). 6 Research on the association between insomnia and suicidal ideation among the general population are still scarce and with inconsistent conclusions. For instance, one study indicated that insomnia was associated with suicidal ideation independent of mental health problems, 7 whereas another study suggested that insomnia affected suicidal ideation exclusively through mental health problems. 8 Besides, both insomnia and suicidal ideation are common complaints among people with mental disorders.2,9 -11 Insomnia usually co-occurs with mental disorders, 9 and researchers have found that sleep problems in people with psychiatric disorders would relate to adverse outcomes such as reduced social functioning 10 and quality of life. 11 Suicidal ideation was also common in psychiatric patients, and a nationwide survey in China reported that people with preexisting mental disorders presented a high prevalence (41.6%) of suicidal ideation. 2 It is thus interesting and important to consider the potential confound of mental health when studying issues related to insomnia and suicidal ideation.
General self-efficacy refers to the broad beliefs people hold about their overall ability or competence in responding to multiple domains of stressful or challenging demands in life. 12 General self-efficacy has been reported to be associated with both insomnia symptoms 13 and suicidal ideation. 14 Besides, a recent study presented self-efficacy as associated with both family support and suicidal ideation. 15 The above knowledge indicates that general self-efficacy can very likely be associated with both insomnia symptoms and suicidal ideation as well, which is yet neglected in previous research and warrants investigation.
The coronavirus disease 2019 (COVID-19) pandemic, a major threat to the public globally in recent years characterized by rapid transmission and high contagiousness, has posed additional and profound negative impacts on general population’s daily life and well-being. Presumably triggered by stressors such as fear of infection, quarantine and social distancing, employment instability and other pandemic-related environmental changes, higher prevalence of sleep disturbances, mental problems (e.g., anxiety and depression), and even suicide has been reported during the infectious disease outbreak. 16 Given such background, to more comprehensively unveil the profile of suicidal ideation and its associated factors during the COVID-19 pandemic is thus of particular importance for future suicide prevention policy-making under public health emergencies. Therefore, this study aimed to estimate the prevalence of suicidal ideation and to examine the associations between insomnia symptoms, general self-efficacy, and suicidal ideation among community-dwelled adults in China during specifically the COVID-19 pandemic.
Methods
Data Source
Lishui, located in southwest of Jiangsu Province, is predominantly semirural with a population of around half a million and an area of 1067 square kilometers. Of the total residential population in Lishui, there were approximate 50.2% males and 22.4% people aged 60 years and older, which was comparable with the national estimates of 51.2% males and 18.7% people aged 60+ years from the Seventh National Population Census of China. 17 We employed data from the Lishui Household Mental Health Survey, which was carried out during the period of September to November 2021. The survey used a two-stage design and stratified random sampling scheme with probability proportional to size across all administrative regions in Lishui, to obtain a representative sample of noninstitutionalized adults aged 18 years and over. Within each administrative region (town), sampling strata were randomly selected based on subordinate natural administrative areas (communities). Within each stratum, random sampling was carried out with probability proportional to population size. The sampling interval (ie, the total population divided by the number of communities) was defined using the most up-to-date population estimates and address information from the Bureau of Civil Affairs and Public Security in Lishui. This procedure identified eight towns, 25 neighborhood communities, and 2000 residential households. Allowing for possible nonresponse, we randomly selected one or two eligible adults from each household, and 2200 individuals were ultimately drawn. With a response rate of approximately 93.2%, the survey finally comprised a total of 2051 study participants residing in Lishui for at least 6 months. Trained interviewers used a structured questionnaire to collect data concerning sociodemographics, health-related behaviors, health status, and so on. The survey protocol and survey questions were approved by the Leading Group of Jiangsu Provincial Survey on Mental Health. The sampling scheme was reviewed by experts from the Jiangsu Provincial Center for Disease Control. Strict quality control measures were carried out from the design of the electronic questionnaires to the checking of the returned data as well as from the drafting of sampling frame to the field implementation during the survey. All study participants provided consent to participate in the study. This study was approved by the Institutional Ethics Committee of Zhongda Hospital Affiliated to Southeast University (No. 2021ZDSYLL211-P01).
Measurements
Suicidal ideation
We defined suicidal ideation as binary, that is, yes or no, according to the affirmative response to the question “Did you seriously think of trying to kill yourself at any time in the past, regardless of whether you would actually do it at that time?”
Insomnia symptom
We used the seven-item Insomnia Severity Index 18 to evaluate the nature and symptoms of any sleep disturbance. Each of the seven answers was rated on a 5-point Likert scale, and they were added up to get a comprehensive score for interpreting severity of insomnia. Cronbach alpha coefficient for the scale of insomnia was 0.91 in this study, indicating an excellent internal consistency. We defined respondents without clinically significant insomnia as having a total score of 0 to 7 points, whereas the others more or less experienced sleep disorders. For sensitivity analysis, we further used a total score of 14 as the cut-off for moderate-and-severe insomnia of clinical significance.
General self-efficacy
General self-efficacy was assessed using the 10-item Generalized Self-efficacy Scale (GSES) 19 to evaluate respondents’ beliefs about their capability to cope with life’s demands. Each of the 10 answers was rated on a 4-point Likert scale, and they were added up to get a comprehensive score. The total score ranged between 10 and 40, with higher scores indicating more confidence in their reactions for successful outcomes. In our study, the Cronbach alpha coefficient for general self-efficacy was 0.90, which indicated excellent internal consistency.
Mental health problems
Mental health problems were assessed based on anxiety and depression in this study. We identified people having anxiety symptoms using the 7-item Generalized Anxiety Disorder Scale, based on a total score of greater than or equal to 10 points. People having depressive symptoms were identified based on a combined use of the two-item Patient Health Questionnaire (if the total score was 2 points or more) and the nine-item Patient Health Questionnaire (if the total score was 10 points or more), given that such approach had a similar sensitivity but higher specificity than the use of either instrument alone. 20 Participants with either anxiety or depression were defined as having mental health problems, or otherwise no. Psychometric validation of the Chinese versions of aforementioned insomnia, general self-efficacy, anxiety, and depression survey instruments demonstrated acceptable sensitivity and specificity in symptom detection. 21
Control variables
The following variables were chosen as covariates: age group as 18 to 34, 35 to 59, or 60 years and above; sex as female or male; residence as urban or rural; marital status as currently married or others (including unmarried, divorced, widowed and others); manual workers as yes (including farmers, workers, and service staff) or no; education attainment as primary school and below, secondary school, or college and higher; frequency of physical exercise as at least 1-day per week or none; smoking history as yes (including current and past smokers) or never; alcohol drinking as regular drinker or nondrinker; life satisfaction as high (self-reported extremely, very, quite satisfied) or low (self-reported fairly, completely not satisfied); self-rated health as good (self-reported excellent, great, good) or poor (self-reported fair, poor); having chronic pain as yes or no; and above-average monthly personal income in the past year as yes (≥3000 CNY) or no (<3000 CNY). Apart from models adjusting for previous confounders, we additionally considered mental health problems as a covariate.
Statistical Analysis
We used STATA Version 16.0 svy package for all data analysis. All survey data were entered into a custom-designed database and weighted back to the general population aged 18 years and over in Lishui using standard weighting procedures. Weighted numbers with proportions for categorical variables and mean values with standard deviations for continuous variables were calculated to describe the characteristics of the study population. We used a series of weighted multiple logistic or linear regression models to estimate the associations among insomnia symptoms, general self-efficacy, and suicidal ideation, with results presented as adjusted odds ratio (OR) and 95% confidence interval (CI) for binary outcome or adjusted β and 95% CI for continuous outcome. The above associations were modeled hierarchically, through firstly adjusting for all predefined covariates and then additionally controlling for the covariate of mental health problems.
The sequential regression models of general self-efficacy can be carried out as follows: (1) the main independent variable (X, insomnia symptom) is significantly related to the outcome variable (Y, suicidal ideation); (2) the independent variable (X) is significantly associated with the focal variable (M, general self-efficacy); and (3) the focal variable (M) is significantly related to the outcome variable (Y) when the independent variable (X) is controlled. Afterward, we employed Bootstrap resampling method with 2000 replications for mediation test. The bias-corrected bootstrap CIs of indirect effect was assessed, and we considered the indirect effect as significant if its upper and lower bound of the 95% CI did not straddle zero. We used the STATA linktest to examine the model specification and found no indication of model mis-specification. A P-value less than .05 was considered statistically significant.
We further carried out a series of sensitivity analyses. We examined the association of moderate-severe insomnia with suicide ideation. According to the responses to the question “In general, how well are you sleeping?,” we also modeled sleep quality instead of insomnia as another indication of presence (i.e., “fair” and “poor” responses) or absence (i.e., “excellent,” “great,” and “good” responses) of sleep disturbance.
Results
This study included 2051 participants and covered a weighted number of 374 000 persons. A weighted 6.38% of study participants had experienced suicidal ideation. Table 1 shows the baseline characteristics of participants according to suicidal ideation. Relative to their comparator group, a higher proportion of individuals with suicidal ideation reported mental health problems (33.98% [8108 of 23 861] vs 5.13% [17 962 of 350 139]) and experienced insomnia (56.51% [13 484 of 23 861] vs 17.35% [60 749 of 350 139]). Participants with suicidal ideation were less likely to report high life satisfaction (33.95% [8101 of 23 861] vs 50.30% [176 120 of 350 139]) or good self-rated health (34.66% [8270 of 23 861] vs 67.29% [235 609 of 350 139]) than those without suicidal ideation. They also reported lower general self-efficacy scores than their counterparts (26.21±5.27 vs 28.92±4.41).
Participant Characteristics in the 2021 Lishui Household Mental Health Survey.
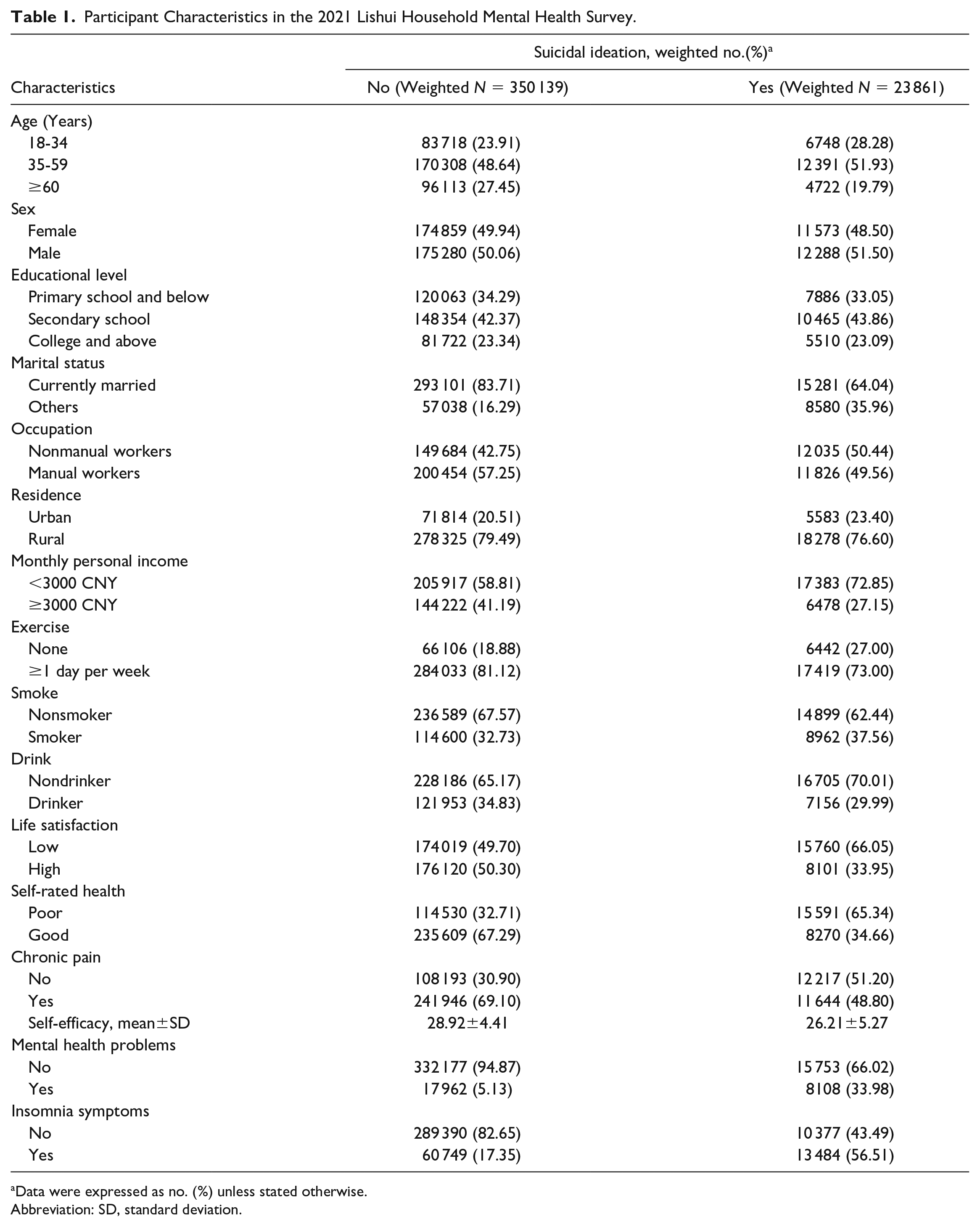
Data were expressed as no. (%) unless stated otherwise.
Abbreviation: SD, standard deviation.
Table 2 presents the results on a series of regression models describing the associations among insomnia symptom, general self-efficacy, and suicidal ideation. Participants reporting insomnia symptoms were significantly associated with increased odds of suicidal ideation (OR = 4.25, 95% CI [2.66, 6.80]; see Models A: X on Y) and decreased level of general self-efficacy (β = −1.11; 95% CI [−1.90, −0.32]; see Models A: X on M), after controlling for covariates including age, sex, education, marital status, occupation, residence, income, exercise, smoke, drink, life satisfaction, self-rated health, and chronic health. The OR of insomnia symptom with suicidal ideation decreased but remained significant after additionally adjusting for general self-efficacy (OR = 3.88, 95% CI [2.49, 6.04]; see Models A: X+M on Y), whereas higher general self-efficacy was associated with lower odds of suicidal ideation (OR = 0.90, 95% CI [0.89, 0.96]; see Models A: X+M on Y). The above results remain virtually consistent when models additionally adjusted for covariate of mental health problems (see Models B).
The Associations Among Insomnia Symptom, General Self-Efficacy, and Suicidal Ideation (N = 2051).
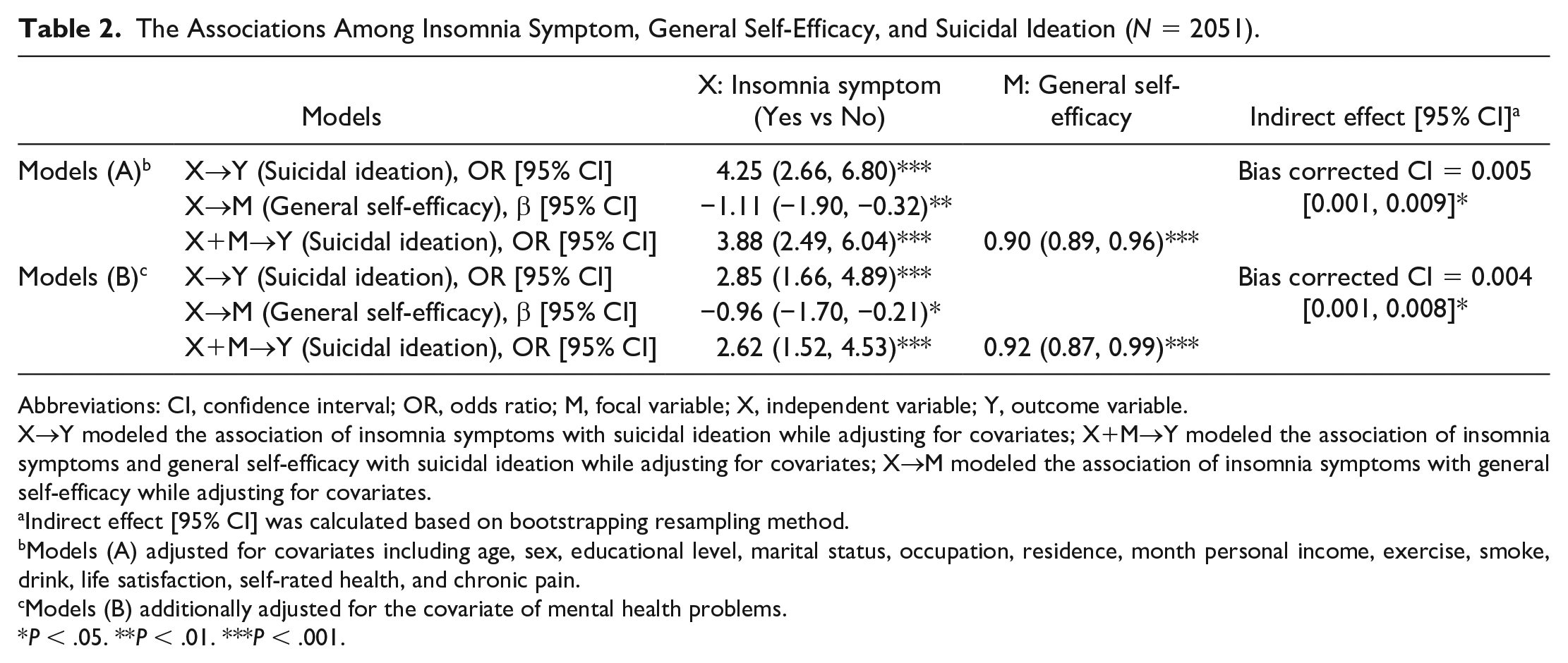
Abbreviations: CI, confidence interval; OR, odds ratio; M, focal variable; X, independent variable; Y, outcome variable.
X→Y modeled the association of insomnia symptoms with suicidal ideation while adjusting for covariates; X+M→Y modeled the association of insomnia symptoms and general self-efficacy with suicidal ideation while adjusting for covariates; X→M modeled the association of insomnia symptoms with general self-efficacy while adjusting for covariates.
Indirect effect [95% CI] was calculated based on bootstrapping resampling method.
Models (A) adjusted for covariates including age, sex, educational level, marital status, occupation, residence, month personal income, exercise, smoke, drink, life satisfaction, self-rated health, and chronic pain.
Models (B) additionally adjusted for the covariate of mental health problems.
P < .05. **P < .01. ***P < .001.
Table 2 also presents that insomnia symptom showed the significant association with suicidal ideation through general self-efficacy (95% bias-corrected bootstrap CIs for its corresponding relative indirect effects did not overlap zero, in both models adjusting for covariates with and without mental health problems), which indicated that general self-efficacy was associated with insomnia symptoms and suicidal ideation.
In sensitivity analysis, we examined the separate association of moderate-severe insomnia (Table 3) and sleep quality (Table 4), as two alternate indicators for sleep assessment, with suicide ideation. Moderate-severe insomnia was found to be significantly associated higher odds of suicidal ideation while adjusting for aforementioned covariates (OR = 3.75, 95% CI [2.30, 6.11], Model 1 in Table 3) and when additionally adjusted for mental health problems (OR = 1.90, 95% CI [1.05, 3.43], Model 2) or general self-efficacy (OR = 3.42, 95% CI [2.07, 5.65], Model 3). The OR for moderate-severe insomnia on suicidal ideation was no longer significant with simultaneous adjustment for general self-efficacy and all covariates including mental health problems (see Model 4). Poor sleep quality was also significantly associated with an elevated odds of suicidal ideation when we adjusted for other covariates with and without general self-efficacy (OR = 2.04, 95% CI [1.17, 3.56], Model 1 in Table 4; OR = 1.95, 95% CI [1.10, 3.48], Model 3 in Table 4). Similarly, the association between sleep quality and suicidal ideation was nonsignificant once the mental health problems was additionally put into the model (Model 2 and Model 4 in Table 4).
Sensitivity Analysis on the Association of Moderate-Severe Insomnia Symptom With Suicidal Ideation (N = 2051).
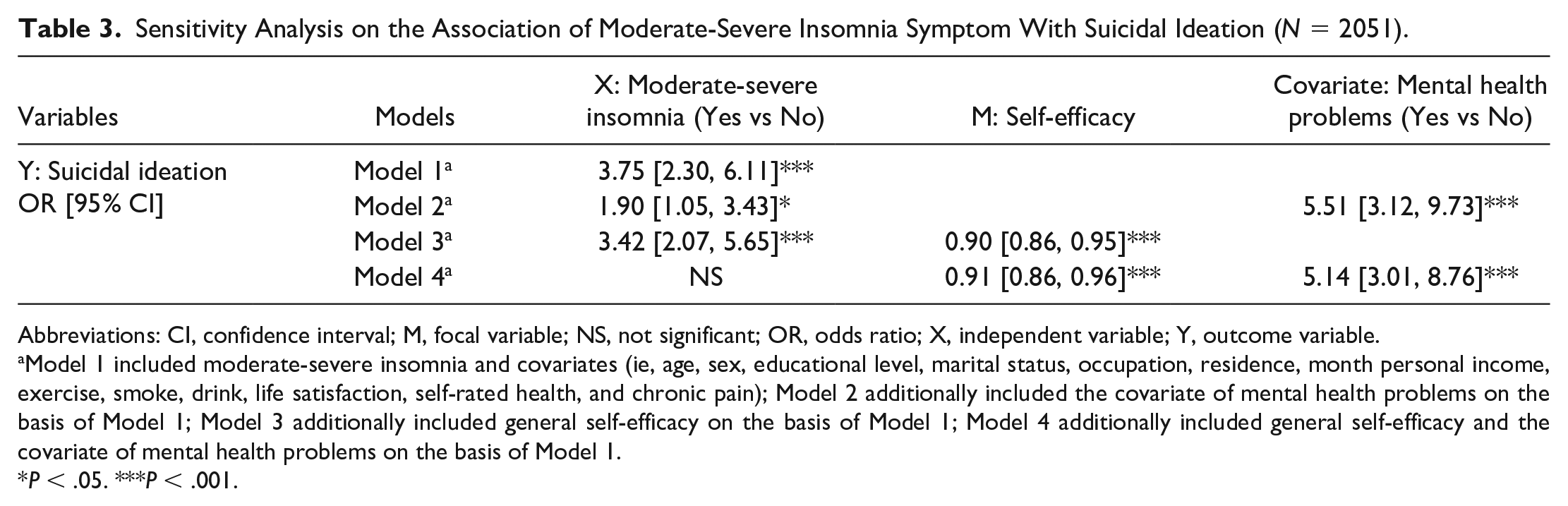
Abbreviations: CI, confidence interval; M, focal variable; NS, not significant; OR, odds ratio; X, independent variable; Y, outcome variable.
Model 1 included moderate-severe insomnia and covariates (ie, age, sex, educational level, marital status, occupation, residence, month personal income, exercise, smoke, drink, life satisfaction, self-rated health, and chronic pain); Model 2 additionally included the covariate of mental health problems on the basis of Model 1; Model 3 additionally included general self-efficacy on the basis of Model 1; Model 4 additionally included general self-efficacy and the covariate of mental health problems on the basis of Model 1.
P < .05. ***P < .001.
Sensitivity Analysis on the Association of Sleep Quality With Suicidal Ideation (N = 2051).
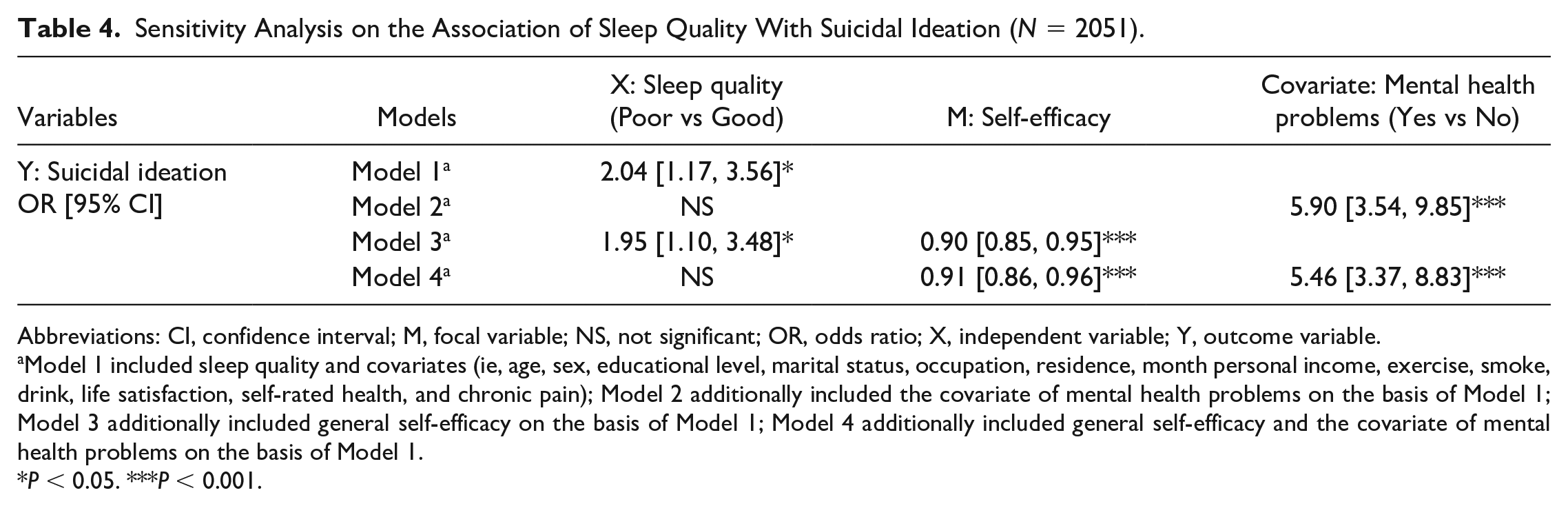
Abbreviations: CI, confidence interval; M, focal variable; NS, not significant; OR, odds ratio; X, independent variable; Y, outcome variable.
Model 1 included sleep quality and covariates (ie, age, sex, educational level, marital status, occupation, residence, month personal income, exercise, smoke, drink, life satisfaction, self-rated health, and chronic pain); Model 2 additionally included the covariate of mental health problems on the basis of Model 1; Model 3 additionally included general self-efficacy on the basis of Model 1; Model 4 additionally included general self-efficacy and the covariate of mental health problems on the basis of Model 1.
P < 0.05. ***P < 0.001.
Discussion
This study observed a prevalence rate of suicidal ideation, during the pandemic of COVID-19, among Chinese community-based population as 6.38%. This prevalence was indeed an increment compared with the previously reported prevalence of 3.9% in the general Chinese population before the COVID-19 pandemic, 3 implying that suicidal ideation is becoming an increasingly common health threat particularly when people are confronted by unexpected catastrophe such as COVID-19.
Our study indicates that insomnia symptom remains associated with higher odds of suicidal ideation in community-based populations after adjustment for mental health problems. This is generally consistent with recent studies, which have revealed that insomnia symptoms increase the odds of suicidal ideation with adjustments including depression.7,22 Our study further expanded the population likely to be affected by the above association to include a broader group of community-based adults. In contrast, another literature documented that mental health problems were associated with both insomnia and suicide. 8 Discrepancies in findings may be due to that they defined insomnia based on a single question, 8 while we measured insomnia symptoms with a standardized tool of Insomnia Severity Index Scale. Insomnia is becoming an increasingly prevalent, persistent, and disturbing concern worldwide, especially against the context of accelerated changes in modernized life styles and the threat of COVID-19 pandemic.2,22 In view of such background, this study provides new insights into the importance of alleviating insomnia symptoms to reduce intentional or unintentional harms, though future research with appropriate prospective design to examine the potential causal relationship between insomnia and suicidal ideation is still warranted to further verify our findings.
Furthermore, our study revealed the association of general self-efficacy with insomnia symptoms and suicidal ideation. We speculated that individuals’ suicidal ideation can be directly associated with insomnia symptoms, as well as indirectly associated with insomnia symptoms through general self-efficacy. Such findings are consistent with past research, which have reported that worse insomnia symptoms are associated with lower general self-efficacy, 13 that people who have lower general self-efficacy are more susceptible to suicidal ideation, 14 and that self-efficacy would perhaps relate increased family support to decreased suicidal ideation. 15 Our study further contributes to the existing knowledge in that previously relatively little was understood regarding general self-efficacy in association with both insomnia symptoms and suicidal ideation. There were other literature focusing on the specific aspect of self-efficacy such as health self-efficacy 23 and coping self-efficacy, 24 but their role in explaining mechanism of suicidal ideation still requires targeted research in the future.
To the best of our knowledge, this is one of the first studies to examine the association of general self-efficacy with suicidal ideation and insomnia symptoms severity. This study to identify the potential mechanism represents an important step toward a more comprehensive understanding of how suicidal ideation develops and maintains, as well as offers opportunities for designing and implementing appropriate intervention or treatment strategies (such as cognitive behavioral therapy 25 and occupational therapy) 26 to reduce insomnia and associated suicide. Moreover, this study suggests that general self-efficacy is a vital factor in understanding an individual’s risk for suicide and represents a possible intervention target for ameliorating potential suicidal risk. Research concerning suicide-prevention education suggests that individuals can acquire skills and self-efficacy beliefs that enable them to stick to healthful behaviors when faced with potential suicidal risks. 15 Policy-makers and relevant stakeholders shall adopt appropriate counseling programs or targeted interventions to promote general self-efficacy and thereby reducing suicidal ideation. Public health implications of this study include that given the invisibility and stigma of suicidal ideation, increased awareness and concerted efforts toward intervening in its modifiable associated factors such as reducing sleep difficulties and improving general self-efficacy may be the more palatable approach to early prevent and control potential suicidal risk. It is imperative for public health practitioners, clinicians, social workers, and other relevant stakeholders to proactively react on suicide-associated threats, especially when the burdensome mental and suicidal problems are increasingly prevalent in the current society facing accelerated urbanization and unpredictable pandemics.
However, there are several limitations to consider when contextualizing these findings. First, we collected the data using cross-sectional methodology, preventing us from confirming a causal relationship for the results. There is possibility of a bidirectional relationship between insomnia and suicidal ideation or between insomnia and self-efficacy, so that interpretation of the role of general self-efficacy in association with both insomnia symptoms and suicide ideation should be interpreted with cautions. Although researchers supported the exploration of mediation analysis with cross-sectional data8,15,27,28 its use in cross-sectional surveys cannot be used to imply causation. Despite limitations in data, this study is novel and meaningful in that it can help generate hypotheses and provide implications for larger and in-depth research in the future to investigate the potential causality between insomnia symptoms and suicidal ideation. Second, there may be other potential confounders that could bias the present findings, for example, disease conditions (such as diabetes mellitus 29 and gambling use) 30 were reported to be associated with sleep and mental health. Future studies can be better designed to consider these omitted potential confounders and further corroborate the findings. Finally, self-report measures did not ensure accuracy of the responses, warranting further longitudinal or experimental studies with objective measurements.
Conclusion
To conclude, this study has found that insomnia symptom remains associated with higher odds of suicidal ideation after adjusting for sociodemographics and mental health status of participants. We also observe that participants with insomnia symptom are likely to have lower general self-efficacy, and higher general self-efficacy is associated with lower odds of suicidal ideation. These findings reinforce the importance of early identification and treatment of suicidal ideation among community-dwelling adult populations, especially during pandemics, and emphasize the priority or potential benefits of eliminating insomnia symptoms and improving general self-efficacy. Future randomized controlled trials are warranted for causality confirmation.
Footnotes
Acknowledgements
The authors sincerely appreciate the efforts of postgraduate students for collecting the data as well as all the participants from Lishui District involved in this study.
Author Contributions
YL conceived and designed the study and drafted the manuscript. WD advised on the study design and data analysis. GMX, DW, MXY, and MY advised on the study design. LJF advised on planning of the study and revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Education of China (grant no. 1125000172, 5725002302); the National Social Science Foundation of China (grant no. 23CGL072); the Fundamental Research Funds for the Central Universities (grant no. 2242021R41104, 2242021S40011, 3225002002A1, 2242020R10007); the Lishui Health Commission (grant no. H2021140029), and Jiangsu Provincial Department of Science and Technology. The sponsors had no role in the design, methods, subject recruitment, data collections, analysis, and preparation of the manuscript.