
Abstract
The aim of this study is the comparison of 2 studies looking at the barriers to access of diabetes care and medicines in the Philippines and Vietnam. These studies used the Rapid Assessment Protocol for Insulin Access. Diabetes care is provided in specialized facilities and appropriate referral systems are lacking. In Vietnam, no problems were reported with regard to diagnostic tools, whereas this was a concern in the public sector in the Philippines. Both countries had high prices for medicines in comparison to international standards. Availability of medicines was better in Vietnam than in the Philippines, especially with regard to insulin. This affected adherence as did a lack of patient education. As countries aim to provide health care to the majority of their populations through universal coverage, the challenge of diabetes cannot be neglected. Trying to achieve universal coverage in parallel to decentralization, national and local governments need adapted guidance for this.
Introduction
“Diabetes is a major threat to global public health that is rapidly getting worse,” 1 and Asia will see the largest absolute increase from 66 993 000 to 99 401 000 estimated individuals with diabetes between 2007 and 2025. 2 Diabetes and other chronic conditions have now replaced communicable diseases as the most common causes of morbidity and mortality, with Asian countries having witnessed this “epidemiological transition” in a very short period of time. 3 This change in the burden of disease affects the functioning of health systems in moving from acute to chronic care. 4 In 2008, it was reported that the shift of the leading causes of morbidity from communicable to noncommunicable diseases (NCDs) occurred in Vietnam. 5 In the Philippines, NCDs account for 6 of the top 10 causes of mortality. 6 This shift in burden is also linked to problems in delivery of care, with a study including the Philippines and Vietnam finding that more than half of the people with diabetes receiving care were not well controlled. 7
To address this change in disease burden and also identify the barriers to chronic care, a clear assessment of the health system is needed. It has been suggested that diabetes can be used as a tracer condition for the proper functioning of health systems and its ability to manage chronic conditions, 8,9 and therefore it was decided to assess the barriers to access to diabetes medicines and care in the Philippines and Vietnam.
The International Diabetes Federation estimates that the prevalence of diabetes in adults in the 20 to 79 age group for Vietnam is 2.5% and in the Philippines 6.5%. 2 Local studies have shown prevalence rates of 2.7% and 4.4% 10 in urban areas in Vietnam, and the second National Diabetes Survey in the Philippines in 2002 11 found diabetes prevalence rates in the 20 to 65 age group to be 5.3% in the capital city and 4.8% in urban and rural areas. Besides this disease burden, diabetes is also a financial burden with cost estimates in 2007 for the Philippines and Vietnam being US$775 million and US$320 million, respectively. 2 It is estimated that these figures will increase to US$2.3 billion and US$1.1 billion for each country by 2025.
The Philippines and Vietnam are aiming to achieve universal health insurance coverage 12 -17 and have decentralized 18,19 the management of health to lower levels of the country’s administrative structure. The Philippines is ranked 102 and Vietnam is ranked 114 out of 182 on the UNDP’s Human Development Index. 20 They have similar domestic population size with approximately 86 million people. Gross national income per capita (in US dollars) is equal to US$3430 in the Philippines and US$2310 in Vietnam. The Philippines (male 68, female 71) has a lower life expectancy than Vietnam (male 72, female 75). Of total government expenditure, 6.4% was spent on health in the Philippines and 6.8% in Vietnam, with out of pocket health expenditure being higher in Vietnam, 86.1%, versus 80.3% in the Philippines of total expenditure on health. 21
The objective of the article is to analyze the results of 2 studies carried out in the Philippines 22,23 and Vietnam 24 looking at the barriers to access to diabetes care and medicines and suggest recommendations that may be applicable to other countries in Southeast Asia facing similar challenges.
Methods
The Rapid Assessment Protocol for Insulin Access (RAPIA) 25 was developed by the International Insulin Foundation and is structured as a multilevel assessment of the different elements that influence the access to diabetes care (see Table 1). The RAPIA draws on the principles of rapid assessment protocols, which have been used extensively to assess services for communicable diseases, including malaria, tuberculosis, and sexually transmitted diseases, for the purpose of developing interventions. 26 -29 This methodology does not statistically analyze the health system by using representative samples but has as its aim to assess in a short time the situation with regard to diabetes care in a given country in order to provide different stakeholders recommendations for action.
Levels of the RAPIA 25
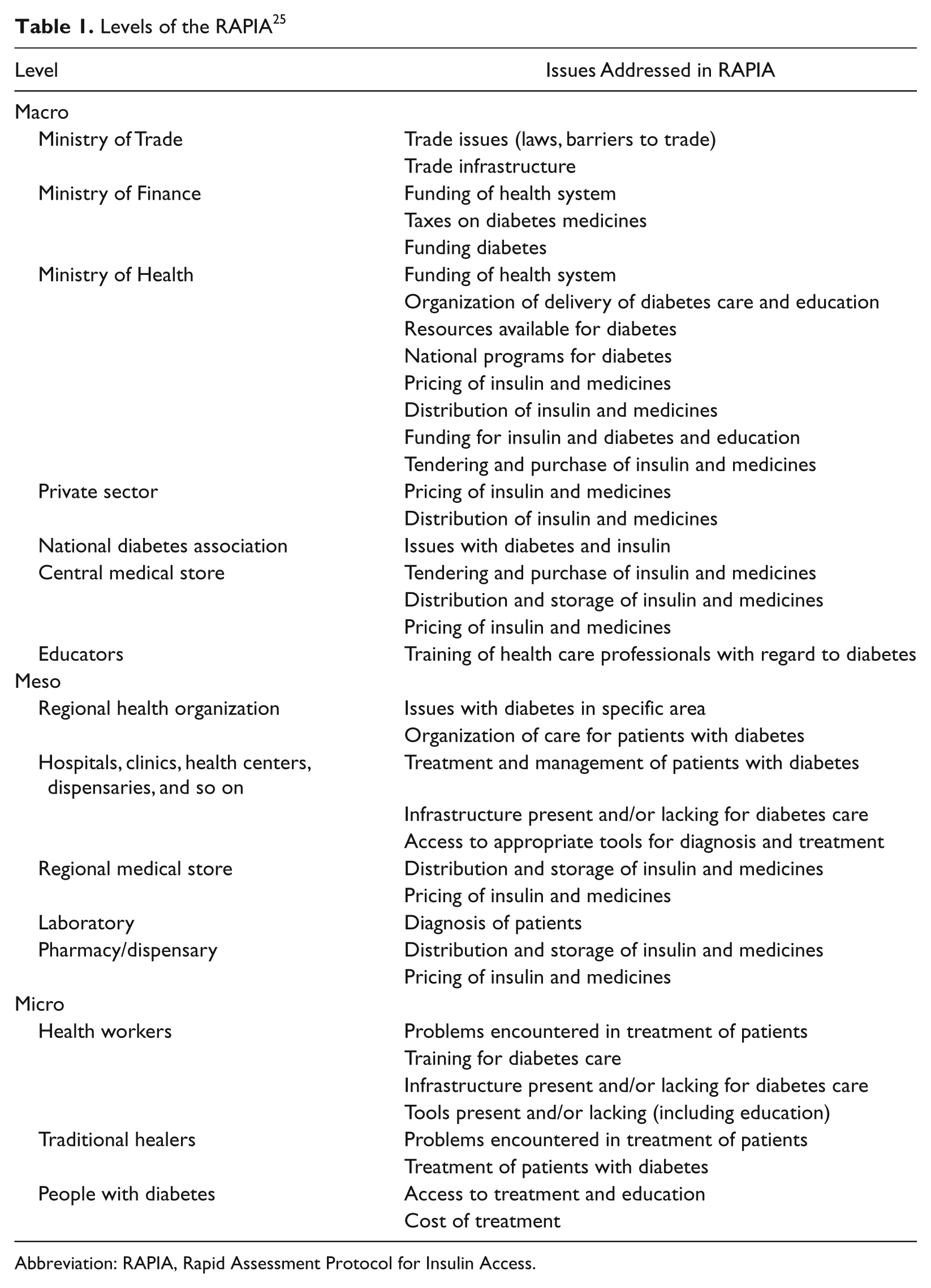
Abbreviation: RAPIA, Rapid Assessment Protocol for Insulin Access.
The RAPIA is divided into 3 components. The first is the macro level, which is aimed at the ministerial levels, private sector, national diabetes association, central medical store, and educators. The meso level targets provincial health officers, “health care settings” (hospitals, clinics, health centers, etc), and pharmacies/dispensaries. Finally, in the micro level carers (health care workers and traditional healers) and people with diabetes are interviewed. The meso and micro levels are implemented in different areas chosen by local stakeholders to be representative of different geographical and socioeconomic situations within the country.
The questionnaires developed and the questions included in them follow each level of the path from the beginning with the purchase and importation of insulin and medicines to the country until these reach or fail to reach the patient. In parallel, the path of care is assessed. The questionnaires serve as a guide and can be adapted to the country investigated. The information is gathered through the different questionnaires (qualitative and quantitative data), site visits, document reviews, and discussions.
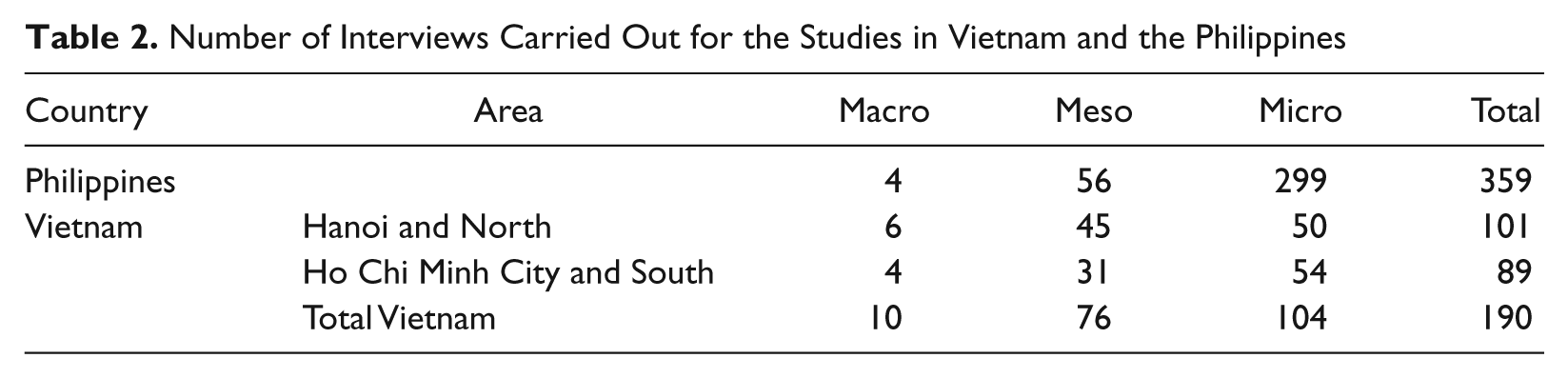
Two studies were separately conducted around the same time in 2008. Local teams trained on how to use the tool carried out interviews. Both teams informed on and collaborated with each other. The Vietnam team, lead by DB, visited 4 areas and carried out 190 interviews. The Philippine team, lead by MH, visited 5 areas and carried out 359 interviews (see Table 2). Both teams approached respondents from different health administration levels (province, district, municipalities, and community) and different sectors (public and private). It was the main reason for the different sample sizes in these studies that more diabetes patients were interviewed in the Philippines to address diversity of patient choices in the country. Different facilities were visited to assess diabetes care with the main facilities viewed as a “center of excellence” for diabetes being surveyed as well as other main facilities. In addition, other facilities were surveyed with the research targeting the lowest-level facility where one would expect diabetes care to be delivered. For people with diabetes, interviews were either carried out on the day of the visit or interviewers returned the day when diabetes consultations were held.
Number of Interviews Carried Out for the Studies in Vietnam and the Philippines
Results
Provision of Diabetes Care
Diabetes care is mainly provided by hospitals with specialized care available at the provincial level in both countries. Most care for diabetes in Vietnam was provided in large urban areas where physicians working in tertiary referral facilities often saw patients for routine consultations. Due to a lack of knowledge of health care workers at lower levels of the health system, care for type 1 diabetes in the Philippines and Vietnam was only provided in a limited number of facilities in main cities. Endocrinology and diabetology are relatively new specialties in Vietnam and therefore there are few doctors considered specialists in this field. In the Philippines, specialty training for endocrinology exists and a private nonprofit institute offers different courses in diabetes.
At the main tertiary facilities in Hanoi and Ho Chi Minh City, all staff have received specialized training in different aspects of diabetes care. At these facilities, nurses play a more active role in care and patient education because of this training. In the Philippines, specialists were concentrated in the provincial capital and usually run private clinics, but also offer some consultations in the public sector.
At provincial and general hospitals in Vietnam some doctors will have had some training in diabetes either from abroad or from specialists from Hanoi or Ho Chi Minh City. In Vietnam, the aim is to devolve diabetes care to the district level, but the main barrier to this policy is lack of trained health care workers. The Philippines has addressed this problem by having professional associations provide both health professionals and lay members with training courses for diabetes educators. Nutritionists and dieticians also play a role in diabetes management, whereas these specialties were lacking in Vietnam.
Guidance exists from the Ministry of Health in Vietnam as to which types of tests should be available to patients at different levels of the health system. There are licensing criteria in the Philippines that include guidance on laboratory equipment. No issues with supplies of reagents or equipment were reported in Vietnam, unlike in the public sector in the Philippines where this was a problem.
Purchase and Supply of Diabetes Medicines
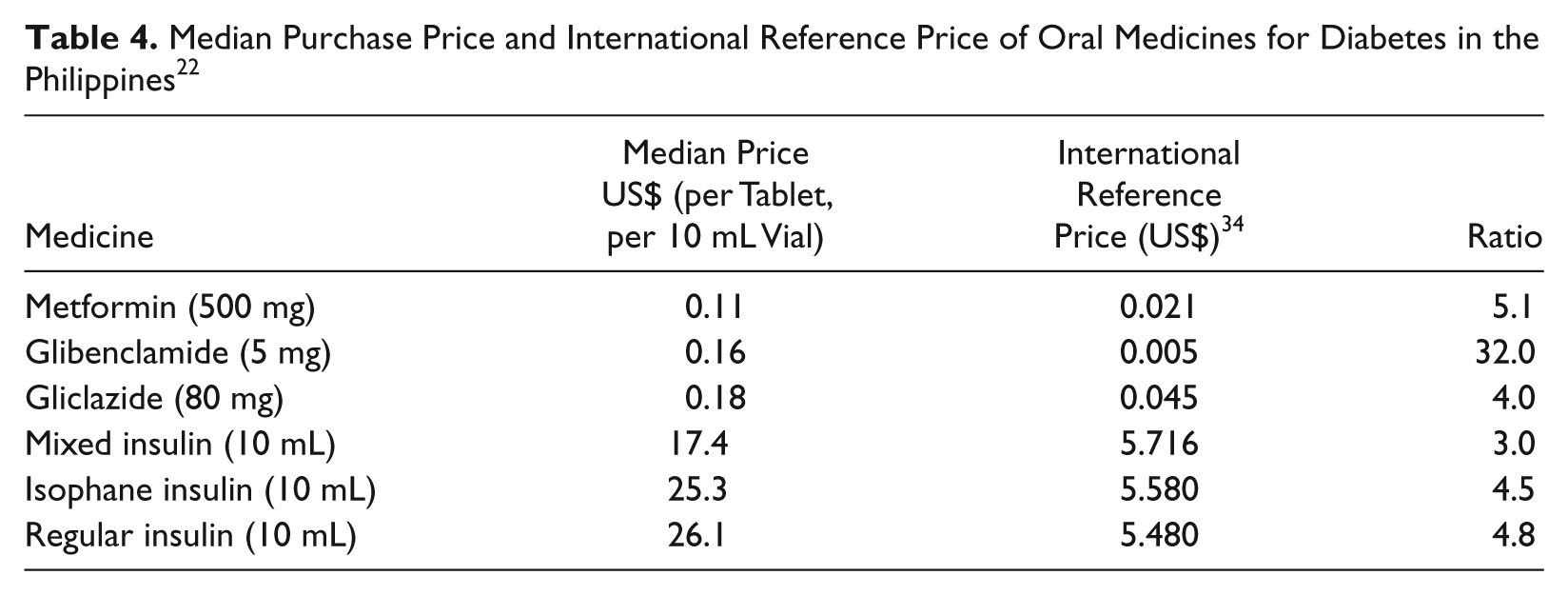
The Ministry of Health in Vietnam prepares guidance prices for different medicines, which are used by each facility to prepare their individual tenders. Some of these prices were up to 6 times higher than those available on the international market. The purchasing of branded medicines versus generics had an impact on expenditure of facilities in Vietnam and ultimately on the individual and/or the insurance system. This information is detailed in Table 3. In the Philippines, prices for common diabetes medicines were found to be substantially higher than international benchmark prices as shown in Table 4.
Price per Tablet Based on Public Sector Tenders and Brand Premium in Vietnam 23
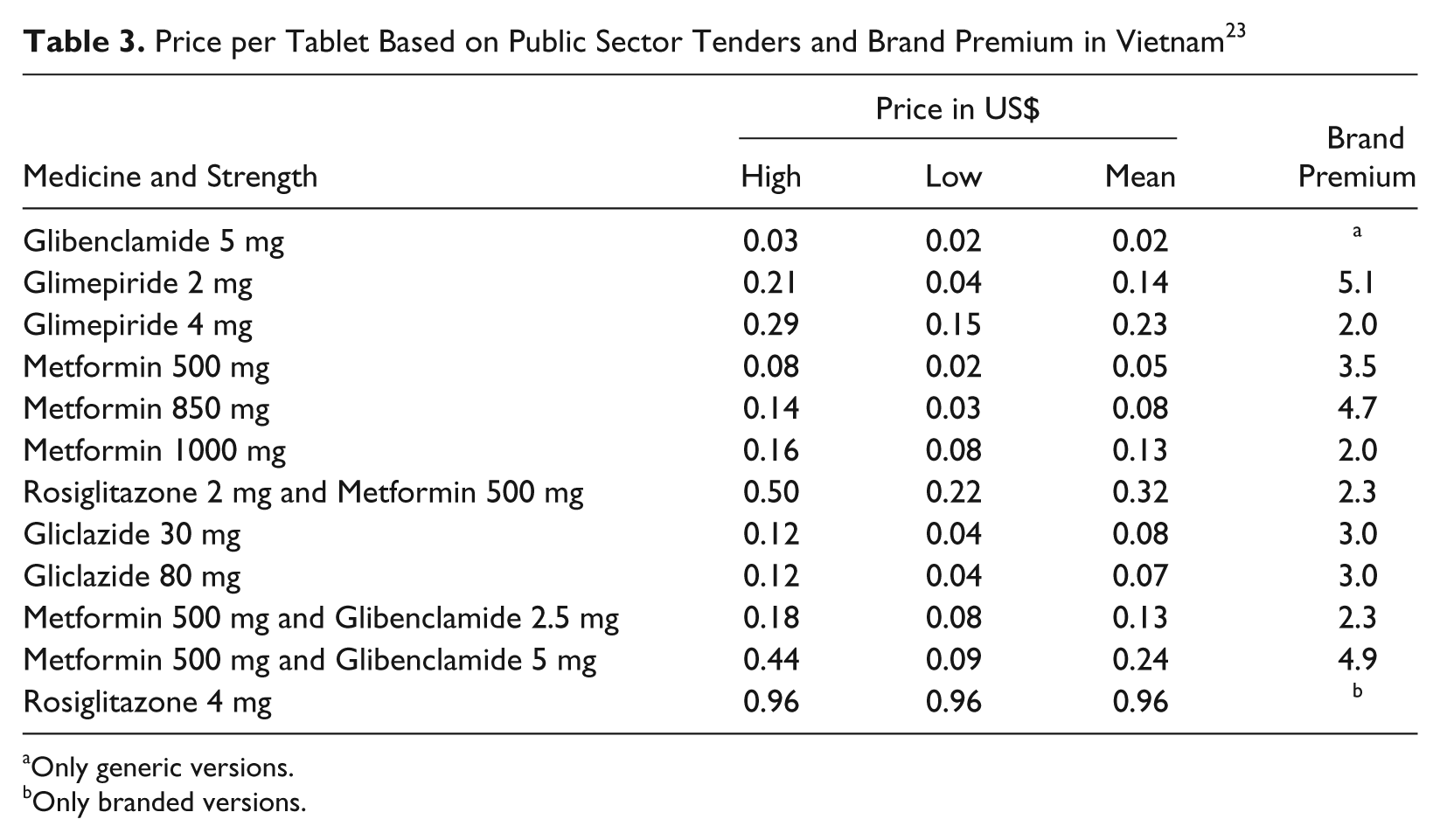
Only generic versions.
Only branded versions.
Median Purchase Price and International Reference Price of Oral Medicines for Diabetes in the Philippines 22
Unlike in Vietnam, medicines for public facilities in the Philippines are procured through the public bidding process at each local government unit based on an annual procurement plan. The Philippine International Trading Corporation, a government-owned and controlled corporation, is responsible for “parallel medicines importation.” These medicines are sold to public hospitals and community medicines outlets at generally lower prices. This is part of the strategies led by the Department of Health to try to reduce medicines price.
In both countries, Glibenclamide and Metformin were available in the majority of hospital pharmacies visited. In Vietnam, other oral medications and insulin were also readily available in the public and private sectors, but this was not the case in the public sector in the Philippines. In pediatric facilities, insulin was not readily available in the public sector in Vietnam and was only available at the main public hospital and in some private hospitals in each province visited in the Philippines.
Insulin and oral medicines for diabetes are subject to 5% import duty and 5% VAT in Vietnam. 30 Mark-ups throughout the supply chain increase the price in the public sector for those without health insurance and the private sector. In the Philippines, medicines are subject to 5% custom duty and 12% VAT. Another factor affecting cost of medicines is the availability of generic versus branded products. In both countries, health care workers and people with diabetes stated their mistrust of generics.
Cost of Diabetes Care for the Individual
People with type 2 diabetes in Vietnam who reported having insurance stated that cost of treatment was not a problem, but other costs such as transportation were sometimes a barrier, especially for people living away from major urban centers. Those without insurance described the financial burden of diabetes, especially type 1 diabetes, as the main obstacle to proper care. Consultation fees at public facilities are free or inexpensive, but the purchasing of medicines and paying for laboratory tests were the major barriers to regular care for the majority of respondents in the Philippines as these are not covered by PhilHealth benefits. Costs of the different aspects of care are detailed in Table 5.
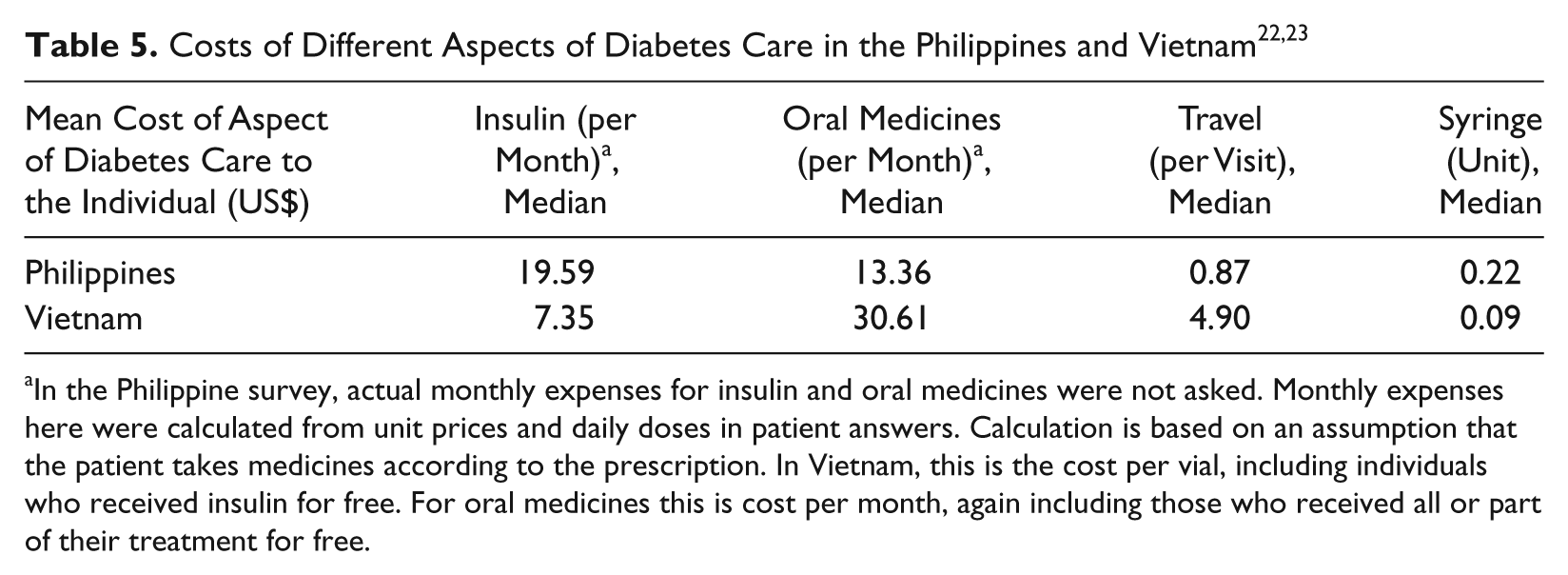
In the Philippine survey, actual monthly expenses for insulin and oral medicines were not asked. Monthly expenses here were calculated from unit prices and daily doses in patient answers. Calculation is based on an assumption that the patient takes medicines according to the prescription. In Vietnam, this is the cost per vial, including individuals who received insulin for free. For oral medicines this is cost per month, again including those who received all or part of their treatment for free.
The private sectors in Vietnam and the Philippines were extremely well supplied with medicines for diabetes. In the private sector in Vietnam and the Philippines, medicines were about 30% and 300% more expensive, respectively, than in the public sector.
Information, Education, and Diabetes Associations
Printed information developed by hospitals and pharmaceutical companies was also available in both countries. The main factor identified as leading to a lack of patient education was shortage of time, with doctors needing to see many patients. Also the health insurance schemes do not cover patient education and counseling. This combined with the high cost of medicines led to poor adherence.
Different organizations involved with diabetes were present in both countries. In Vietnam, the Vietnam Diabetes Association is only for doctors and provides a chance for doctors to meet and discuss different issues surrounding diabetes. There is also a Diabetes Educators Association and anyone can join who has an interest in diabetes. These are mainly active in Hanoi and Ho Chi Minh City. Diabetes clubs exist at different facilities with special diabetes clubs established for children with type 1 diabetes and their families. Their aim is to provide support and education to people with diabetes. These organizations are very dependent on health care workers at these facilities to manage their activities.
Diabetes-related activities varied among the surveyed provinces in the Philippines. In 2 of the 5 areas visited, no diabetes patient support club existed. Establishing and continuing a club seemed to rely on the availability and leadership of physicians in the area. Clubs and their organization varied with some clubs officially registered as an organization and others just gathering patients on a diabetes clinic day. Some clubs routinely (monthly or annually) also collected money from members to support activities.
Policy Environment
A decision by the Vietnamese Prime Minister in 2002 approved a program to control NCDs for the period of 2002 to 2010. This led to a preliminary National Plan for Diabetes prepared for the years 2006 to 2010. 31 The plan highlighted the increasing burden of diabetes in Vietnam and the challenges that Vietnam will face because of this.
Because of the increase in burden of lifestyle-related diseases in the Philippines, the importance of healthy lifestyles has been recognized by the Department of Health. This led to the creation of the National Centre for Disease Prevention and Control in 2000 and a diabetes-specific office at this center. Reduction of mortality and morbidity from lifestyle-related diseases, including diabetes, is listed as one of the goals in “the National Objectives for Health 2005-2010.” Because of decentralization, the level of commitment to implement the program varied among the local government units visited.
The Vietnamese national target program for diabetes and hypertension has recently been approved and receives special funding and attention from the central government. As in the Philippines, because of decentralization, curative activities not effectively linked to promotion and prevention activities, and hospital autonomy, the impact of policy decisions at the central level on actual practice in Vietnam is hard to quantify.
In the Philippines, many policies have focused on the issue of medicine prices (eg, Generics Act of 1988 and Universally Accessible Cheaper and Quality Medicines Act of 2008). Because of a long history of failure in reducing medicine prices, people interviewed were skeptical about the effectiveness of these policies. No such policies have been developed in Vietnam.
Discussion
This comparative study is based on the use of similar methods in Vietnam and the Philippines carried out during the same period of time and therefore allow comparison of 2 similar health systems in Asia.
In both countries, the average cost of overall diabetes care was extremely high, thus having a direct impact on adherence with cost of treatment and medicines being a major barrier. In Vietnam, the average monthly cost of transportation and medicines alone equaled US$34.41, equivalent to 18% of monthly per capita gross national income. The cost of medicines in both the Philippines and Vietnam are passed on to the individual or the insurance system, and therefore procurement practices will affect this cost. Poor procurement practices were present in both countries, leading to high costs of medicines compared with the international market prices as detailed in studies carried out by the World Health Organization and Health Action International. 32
Another factor affecting adherence in both countries was inadequate patient education because of a variety of factors, including overburdened staff, materials not adapted to sociocultural context, lack of trained staff, and a lack of involvement of nurses and other health personnel in managing diabetes.
Once people have registered with the respective insurance schemes these schemes seem to work well, but are often viewed as confusing to register with in the Philippines and to not always be value for money in both countries. Some people in Vietnam said that even though they had or were eligible for health insurance, they preferred to pay out of pocket as they felt they received better service. Health insurance and the aim of achieving universal coverage are an opportunity and a threat to improving the organization of the health system. It is an opportunity as the health insurance scheme could regulate referrals, tests, and medicines being available at different facilities and relieve the burden of cost to the individual. However, this may also have a negative impact as hospitals will keep people in their patient population as they are viewed as a source of income.
This also affects referral systems, which are important for long-term care because as seen in Vietnam, hospitals are individual entities whose sources of income comes from the government (central and local), out of pocket payments, and payments from insurance. In addition, away from major cities diabetes care is problematic because of a lack of specialized staff as well as inadequate infrastructure. With decentralization and the organization of the health system, each facility and its relationship with other facilities higher and lower in the overall system may not be clear. This affects referrals, especially from provinces to larger urban centers.
Conclusion
As countries in Asia develop the means to provide health care to the majority of their populations, the challenge of diabetes and other NCDs cannot be neglected. These conditions will not only burden individuals but also the health systems and economies of these countries. A recent strategy published by the World Health Organization 33 addresses both the issue of high out of pocket payments and how these act as a major barrier to achieving universal coverage in Asia. This strategy document provides clear guidance on how to achieve universal coverage, but to address the increasing burden of diabetes and NCDs, creativity is needed. In this changing disease burden, the role of health insurance should be increased from one that simply reimburses medical care to one that actively tries to prevent chronic diseases. Linking this approach to decentralization, national and local governments need to adapt guidance from the central level to effectively address a health concern that affects all levels of society and therefore clearly define their role in the struggle to prevent and deal with the increasing burden of diabetes and other NCDs.
Footnotes
Acknowledgements
The guidance, support, and comments on drafts of Richard Laing from the World Health Organization are most gratefully recognized by both authors. Support from the following people is gratefully recognized for the work in Vietnam: Dr Larry Deeb and Delice Gan from the International Diabetes Federation, the Trustees of the International Insulin Foundation, John Bowis MEP, Dr Maximilian de Courten, Professor Geoffrey Gill, Professor Harry Keen, Professor Ayesha Motala, Dr Kaushik Ramaiya, Professor Solomon Tesfaye, Professor Nigel Unwin, and Professor John S. Yudkin, as well as local colleagues Professor Nguyen Thy Khue, Professor Ta Van Binh, Dr Hoang Kim Uoc, Dr Le Quang Toan, Dr Nguyen Bich Phuong, Professor Garry Warne, and Dr Kate Armstrong. The following individuals’ support is acknowledged for the work in the Philippines: Dr Clive Ondari, Dr Edelisa Carandang, Ms Alexandra Cameron, Dr Budiono Santoso, Dr Soe Nyuntu, Dr Socorro Escalante, Dr Robert L. P. So, Dr Dennis S. Quiambao, Dr Madeleine R. Valera, Dr Tim Reed, and Ms Margaret Ewan.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
The pilot and development of the RAPIA was made possible thanks to a grant from the World Diabetes Foundation. For the work in Vietnam, the International Insulin Foundation (IIF) received a grant from the International Diabetes Federation, which received support from the Lilly Foundation for this project. The IIF has also received support from the Diabetes Foundation for its work. Support for MH’s work in the Philippines was sponsored by the Foundation for Advanced Studies on International Development and Health Action International.