
Abstract
Phyllodes tumors are rare biphasic breast tumors with the potential for both local recurrence and distant metastasis. The aberrant expression of B7-H3 and B7-H4 B7 molecules could be potential targets for future development of immunotherapeutic approaches. This work was undertaken to evaluate the expression of B7-H3 and B7-H4 in phyllodes tumors and assess the association with the grade and clinical behavior of phyllodes tumors. In addition, the roles of B7-H3 and B7-H4 in the regulation of tumor immune surveillance were evaluated by assessing the relationship between B7-H3/B7-H4 expression and T-cell infiltration. The messenger RNA and protein expression of B7-H3/B7-H4 were determined by RNAscope in situ hybridization and immunohistochemistry, respectively, in 101 phyllodes tumors (60 benign, 26 borderline, and 15 malignant) using a tissue microarray. Immunohistochemistry for CD3 and CD8 was also performed. B7-H3 messenger RNA and protein appeared to be concentrated mainly in the stromal compartment of phyllodes tumors. However, B7-H4 messenger RNA and protein were undetectable in the stromal compartment of phyllodes tumors. Stromal B7-H3 messenger RNA and protein expression were noted in 10 (16.7%) and 31 (51.7%) of 60 benign phyllodes tumors, 12 (46.1%) and 20 (76.9%) of 26 borderline phyllodes tumors, and 10 (66.7%) and 13 (86.7%) of 15 malignant phyllodes tumors, respectively. Stromal B7-H3 messenger RNA and protein expression increased as phyllodes tumors progressed from benign to borderline and finally to the malignant grade (Pearson’s R = 0.411, p < 0.001 and Pearson’s R = 0.293, p = 0.003, respectively). The recurrence rate was higher in the stromal B7-H3 messenger RNA or protein-positive group than in the negative group, but this difference was not significant. Stromal B7-H3 protein expression inversely correlated with the densities of CD3+ and CD8+ T-cell infiltrates (p = 0.001 and p = 0.027, respectively). These results suggest that B7-H3 is involved in the progression of phyllodes tumors and may contribute to their immune surveillance.
Introduction
Phyllodes tumors (PTs) are rare biphasic fibroepithelial neoplasms with a reported incidence <1% of all primary tumors of the breast.1,2 Based on their histological characteristics, PTs are subclassified as benign, borderline, or malignant. 1 Overgrowth of the sarcomatous stromal component is one of the characteristic features of malignant PTs.
The standard treatment for PTs is complete surgical resection with negative margins. 2 Local recurrences occur in all PTs with a range of 10%–65% and distant metastases develop in about 5%–40% of all PTs.3,4 Recurrent and metastatic PTs pose a therapeutic challenge, since effective treatment options have not yet been reported.3–6 Therefore, the development of new treatment options for PTs is of paramount importance for the improvement of public health.
Cancer immunotherapy is a promising new treatment strategy that harnesses and enhances the innate powers of the immune system to fight cancer.7,8 Recent clinical trials have indicated a potential for using immunotherapeutic approaches in patients with sarcomas.9–11 Therefore, we sought to identify targetable immune regulators in PTs of the breast. The interactions between B7 molecules and CD28-family receptors are essential for the regulation of adaptive immunity.12,13 In human tumors, the aberrant expression of several co-inhibitory molecules belonging to the B7 family leads to reduced anti-tumor immunity and immune evasion. 13
B7-H3 and B7-H4 are two of the most significant co-inhibitory molecules of the B7 family, and they can negatively regulate the T-cell immune response by inhibiting T-cell activation and proliferation.14,15 B7-H3 and B7-H4 have been implicated in the development and suppression of multiple solid tumors, including breast cancer, and they appear to be promising new targets for immunotherapies.16–19 Recent studies have revealed that the protein expression of B7-H3 and B7-H4 is elevated in sarcoma and assists in tumor progression.20–22 Nonetheless, limited information has been available regarding the expression of B7-H3 and B7-H4 within PTs.
Almost all prior studies have measured B7-H3 or B7-H4 expression by immunohistochemistry (IHC) in formalin-fixed, paraffin-embedded (FFPE) sections, and no uniform standard has been defined for B7-H3 or B7-H4 staining. Recently, a novel antibody-independent assay for messenger RNA (mRNA) in situ hybridization (ISH) in FFPE tissues using the RNAscope® method has become a preferred approach owing to its advantages of a high specificity and objective interpretation.23,24
The purpose of this study was to evaluate the mRNA and protein expression of B7-H3 and B7-H4 in PTs and evaluate correlations between the expression data and the clinicopathological features of PTs. In addition, correlations between B7-H3 or B7-H4 expression and the infiltration of T-lymphocytes were also assessed to investigate the immunomodulatory functions of these molecules. The mRNA and protein expression of B7-H3/B7-H4 were determined by RNAscope ISH and IHC, respectively, in 101 PTs using a tissue microarray (TMA) approach. In addition, immunohistochemical staining for CD3 and CD8 was also performed.
Materials and methods
Tumor samples
FFPE PT samples obtained between January 1999 and December 2012 were retrieved from four institutions (Chonnam National University Hospital, Chonnam National University Hwasun Hospital, Cell In All Private Clinics, and Foryou Private Clinics).
Hematoxylin and eosin-stained slides of PTs were reviewed, and the original diagnosis was confirmed in all cases by two pathologists. The subclassification of PTs as benign, borderline, and malignant was performed based on the 2012 World Health Organization criteria. 1 One hundred and one cases, including 60 benign, 26 borderline, and 15 malignant PTs, were selected. Some PT cases were offered by the Biobank of Chonnam National University Hwasun Hospital, a member of the Korea Biobank Network. This study was approved by the ethics committee of Chonnam National University Hwasun Hospital under the condition of anonymization (reference: CNUHH-2017-021).
Histologically representative areas in each PT were selected for inclusion in TMA blocks. Two cores (2 mm in diameter) from each FFPE block were punched to make a TMA block. A total of 40 cores per TMA block and five TMA blocks were prepared manually. Serial sections at a thickness of 4 μm were consecutively cut using a rotary microtome and mounted on charged slides (Superfrost™ Plus, Thermo Fisher Scientific, Massachusetts, USA). Sections were stained with hematoxylin and eosin to confirm the presence of the selected areas.
RNAscope ISH assay
For the detection of B7-H3 and B7-H4 mRNA transcripts, a chromogenic RNAscope ISH assay was performed using an RNAscope FFPE assay kit (Advanced Cell Diagnostics, California, USA) as previously described.23–25 Briefly, TMA slides were deparaffinized, dehydrated, and pretreated with heat and protease digestion. Thereafter, the slides were hybridized with RNAscope probes at 40°C for 2 h. The following RNAscope probes were used in this study: Hs-B7-H3 (430411, accession #NM_001024736.1, nucleotides 1233–2214), Hs-B7-H4 (418081, accession #NM_001253849.1, nucleotides 745–1844), positive control probe peptidylprolyl isomerase B (Hs-PPIB), and negative control probe bacterial dihydrodipicolinate reductase (DapB). The hybridization signal was visualized using an RNAscope 2.0 HD reagent kit (Brown) (Advanced Cell Diagnostics). 3,3′-Diaminobenzidine solution was used for color development. The ISH slides were counterstained with Gill’s hematoxylin. FFPE HeLa cell pellet sections were also used to assess the performance of the assay procedure using the PPIB-positive control probe and DapB-negative control probe.
RNAscope ISH slides were digitized (Aperio Technologies, California, USA) and the mRNA signal results were scored as follows based on the manufacturer’s guidelines: 0 (no staining or <1 dot/10 cells), 1 (1–3 dots/cell), 2 (4–10 dots/cell), 3 (>10 dots/cell with <10% of positive cells having dot clusters), and 4 (>10 dots/cell with >10% of positive cells having dot clusters).23,25 Only TMA cores with PPIB scores ≥2 and DapB background scores ≤1 were included in the analysis of B7-H3 and B7-H4 mRNA expression. The results were classified as positive (score 3–4) or negative (score 0–2) for statistical analysis.
IHC assay and evaluation of IHC staining
IHC staining for B7-H3, B7-H4, CD3, and CD8 was conducted on TMA sections using an automated immunostainer (Leica Microsystems, Illinois, USA) according to the manufacturer’s instructions as follows: (1) deparaffinization of the slides using BOND-MAX™ dewax solution; (2) heat-induced antigen retrieval using BOND™ epitope retrieval solution 1; (3) endogenous peroxidase blocking with hydrogen peroxide; (4) incubation with primary antibodies specific to B7-H3 (1:800 dilution, clone 6A1, Thermo Fisher Scientific), B7-H4 (1:20 dilution, clone MIH43, Thermo Fisher Scientific), CD3 (1:50 dilution, clone F7.2.38, DAKO, Glostrup, Denmark), and CD8 (1:100 dilution, clone C8/144B, DAKO); (5) color development with 3,3′-diaminobenzidine; and (6) hematoxylin counterstaining. Negative controls were processed similarly except that the primary antibodies were replaced with dilution buffer.
The immunostained TMA slides were digitized (Aperio Technologies), and the stromal immunoreactivity of B7-H3 and B7-H4 was determined by the intensity and extent of staining according to previously reported methods with slight modifications. 21 The intensity of immunoreactivity was scored as: 0, no reaction; 1, weak reactivity, 2, moderate reactivity; and 3, strong reactivity. The extent of positive immunoreactivity was scored on a scale of 0–3 (0, <5%; 1, 5%–25%; 2, 25%–50%; and 3, >50%). The intensity score and the extent score were multiplied to obtain a final staining score. Final staining scores >4 were defined as positive expression, while scores ≤4 were defined as negative expression.
The densities of CD3+ and CD8+ T-cell infiltrates in the stroma were determined. CD3+ and CD8+ T-lymphocytes were counted and averaged per 3 high-power fields (hpf) within the most densely infiltrated areas. The densities were grouped as: group 0 (≤5 cells/3 hpf), group 1 (6–50 cells/3 hpf), group 2 (51–99 cells/3 hpf), and group 3 (≥100 cells per 3 hpf). The results were classified as low (groups 0–1) or high (groups 2–3). 17
Statistical analysis
The agreement between mRNA ISH and IHC data for B7-H3 and B7-H4 expression was analyzed using the κ statistic method. The linear-by-linear association test was used to analyze the trend in the proportion of samples in which B7-H3 and B7-H4 expression was detected in relation to the grades of PTs. Differences in B7-H3 and B7-H4 expression between groups were analyzed by the chi-square test or Fisher’s exact test. SPSS 13.5 (SPSS Inc., Illinois, USA) was used for statistical analyses and a probability of p < 0.05 was regarded as significant.
Results
Patient demographics
The mean age and tumor size were 46.5 years and 6.1 cm in patients with malignant PTs, 43.7 years and 5.9 cm in those with borderline PTs, and 39.6 years and 4.2 cm in those with benign PTs, respectively. The tumor size increased alongside the grade of PTs (p < 0.05). The median follow-up period was 61 months (range, 5–212 months). A total of 15 patients had a local recurrence. The local recurrence rates were 20.0% (3/15) in the malignant PT group, 15.4% (4/26) in the borderline PT group, and 13.3% (8/60) in the benign PT group, respectively. The local recurrence rate of patients with positive surgical margins was higher than that of patients without positive surgical margins (20.0% vs 12.8%), but this difference was not statistically significant. Distant metastasis was recorded one of malignant PTs. Disease-related death was not recorded.
Expression of B7-H3 and B7-H4 in PTs
To analyze the mRNA expression of B7-H3 and B7-H4 in PTs, an RNAscope ISH assay was performed on the TMA slides of 101 PT specimens. First, we verified the technical quality of the assay using FFPE HeLa cell pellets with a PPIB-positive control probe and a DapB-negative control probe. We found a high PPIB signal with no DapB staining (Figure 1(a)–(d)). Positive staining for the PPIB probe was observed in the nucleus and/or cytoplasm with brown, punctate spots. PPIB control probe had medium sensitivity (10–30 copies of target per cell). Next, the tissue RNA quality of TMA samples was assessed by performing RNAscope ISH with the PPIB-positive control probe and DapB-negative control probe. The mRNA signals of the PPIB probe were variously observed, and all the cores had a score of ≥2 (Figure 1(e) and (f)). No signals were detected on any tissue core with the DapB-negative control probe (Figure 1(g) and (h)). All cores on the TMAs were considered to be suitable for the B7-H3/B7-H4 mRNA ISH study.

RNAscope® in situ hybridization quality control. Sections from HeLa cell pellets showed strong PPIB positive control probe staining (a, b) and clean negative DapB control probe staining (c, d). Serial sections of phyllodes tumors showed positive signals for the PPIB probe (e, f) and no signals for the DapB probe (g, h). (a, c, ×2 magnification, scale bars, 2 mm; e, g, ×4 magnification; scale bars, 600 µm; b, d, f, h, ×400 magnification, scale bars, 60 µm.)
Representative images of ISH staining for B7-H3 and B7-H4 mRNA are shown in, Figure 2; B7-H3 and B7-H4 mRNAs were expressed in both the cytoplasm and nucleus. We found that B7-H3 mRNA was predominantly expressed in the stromal component and at lower levels in the epithelial component of PTs (Figure 2(a), (b), (i), and (j)). On the contrary, B7-H4 mRNA expression was only observed in the epithelial component, while the stromal component was negative for B7-H4 mRNA (Figure 2(c), (d), (k), and (l)).

Expression and localization of B7-H3 mRNA (a, b, i, j), B7-H4 mRNA (c, d, k, l), B7-H3 protein (e, f, m, n), and B7-H4 protein (g, h, o, p) in benign (a–h) and malignant (i–p) phyllodes tumors. B7-H3 mRNA expression was observed in the epithelial and stromal components. However, B7-H4 mRNA and protein expression were only observed in the epithelial component. (a, c, e, g, i, k, m, o, ×4 magnification, scale bars, 600 µm; b, d, f, h, j, l, n, p, ×400 magnification, scale bars, 60 µm.)
To compare the mRNA expression of B7-H3 and B7-H4 with their protein expression, IHC analysis was also performed. B7-H3 and B7-H4 protein expression was observed in the cell cytoplasm and membrane. The staining patterns of B7-H3 and B7-H4 protein expression were concordant with the mRNA expression patterns detected by ISH. Although some B7-H3 protein was detected in the epithelial component, it was mainly concentrated in the stromal component of PTs (Figure 2(e), (f), (m), and (n)). B7-H4 protein was expressed in the epithelial component; however, its expression in the stromal component was negative or weak (Figure 2(g), (h), (o), and (p)). Because none of the studied cases showed positivity for the stromal expression of B7-H4 mRNA or protein, we only further evaluated B7-H3 expression by ISH and IHC. We identified a positive correlation between the mRNA and protein expression of B7-H3 in the stromal component of PTs (r = 0.804, p < 0.001) (Figure 3). In all PTs, the stromal expression of B7-H3 mRNA and protein was confirmed, but for the analysis, its expression was classified as positive or negative on the basis of cutoff points (Table 1). The stromal expression of B7-H3 mRNA and protein was classified as positive or negative on the basis of cutoff points (Table 1). Positive B7-H3 mRNA and protein expression were observed in 32 (31.7%) and 64 (63.4%) cases with PTs, respectively. Thirty-one (30.7%) were found to be B7-H3-positive by both ISH and IHC, and 36 (35.6%) were negative by both ISH and IHC. However, 1 (1.0%) case was assessed as B7-H3-positive by ISH and B7-H3-negative by IHC, while 33 (32.7%) cases were assessed as B7-H3-negative by ISH and B7-H3-positive by IHC. The concordance between B7-H3 mRNA ISH and protein IHC was 66.3% (κ value = 0.387, p < 0.001).
Cross-tabulation of B7-H3 status by mRNA RNAscope® in situ hybridization and protein immunohistochemistry in phyllodes tumors.

Concordance 66.3%; κ value = 0.387, p < 0.001.

Expression of B7-H3 mRNA and protein in the stromal component of phyllodes tumors. A positive correlation was observed between B7-H3 mRNA and protein expression (r = 0.804, p < 0.001).
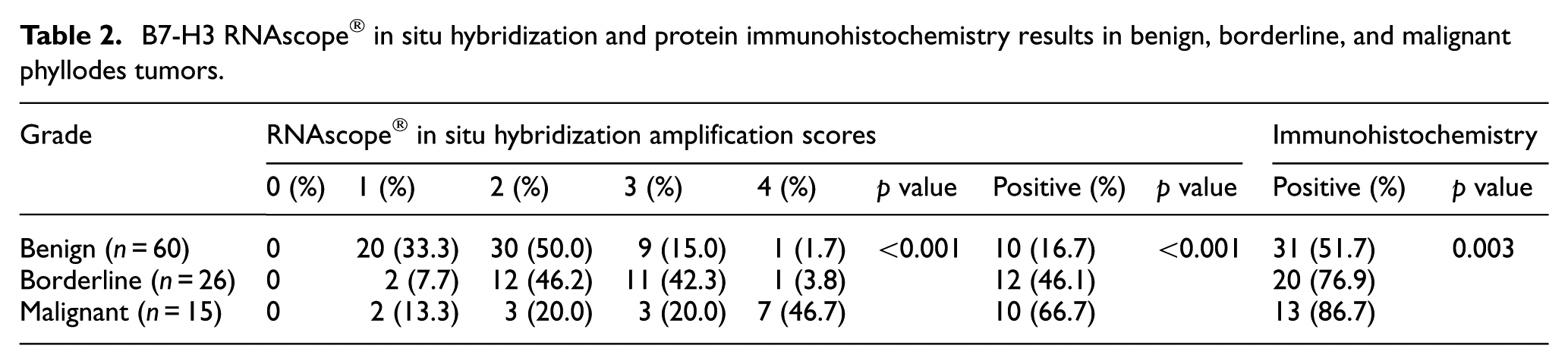
The relationships between stromal B7-H3 mRNA and protein expression and clinicopathological features in PTs were analyzed. Positive stromal expression of B7-H3 mRNA and protein was noted in 10 (16.7%) and 31 (51.7%) of 60 benign PTs, 12 (46.1%) and 20 (76.9%) of 26 borderline PTs, and 10 (66.7%) and 13 (86.7%) of 15 malignant PTs, respectively (Table 2). Stromal B7-H3 mRNA and protein expression increased (Pearson’s R = 0.411, p < 0.001 and Pearson’s R = 0.293, p = 0.003, respectively) as PTs progressed from benign to borderline and finally to the malignant grade. The stromal B7-H3 mRNA and protein expression of the borderline and malignant PTs were significantly higher than those of the benign PTs (p < 0.01 and p < 0.001 for mRNA, p < 0.01 and p < 0.01 for protein, respectively). However, no significant differences in stromal B7-H3 mRNA and protein expression were observed between the borderline and malignant PTs.
B7-H3 RNAscope® in situ hybridization and protein immunohistochemistry results in benign, borderline, and malignant phyllodes tumors.
The percentages of recurrence were higher in the B7-H3 mRNA- and protein-positive groups (18.7%, 6/32 and 18.7%, 12/64, respectively) than in the B7-H3 mRNA- and protein-negative groups (13.0%, 6/69 and 8.1%, 3/37, respectively). However, these differences were not statistically significant (p = 0.319 for B7-H3 mRNA positive vs negative and p = 0.245 for B7-H3 protein positive vs negative).
Infiltration of CD3+ and CD8+ T-cells in PTs
All PTs had CD3+ and CD8+ T-cells in the stromal compartment. The numbers of CD3+ and CD8+ T-lymphocytes per 3 hpf ranged from 2 to 135 (mean ± standard deviation, 26.9 ± 27.8) and 2 to 94 (mean ±standard deviation, 16.1 ± 18.0), respectively. There was no association between the density of CD3+ or CD8+ T-cell infiltrates and the grade of PTs (data not shown).
The densities of CD3+ and CD8+ T-cell infiltrates significantly differed between PTs that were positive for stromal B7-H3 protein expression and those that were negative (p < 0.001 and p = 0.049, respectively; Table 3). After classifying PTs as having high or low T-cell infiltration using cutoff points, high CD3+ and CD8+ T-cell infiltrates were noted in 12 (11.9%) and 8 (7.9%) of 101 PTs, respectively. Stromal B7-H3 protein expression was negatively correlated with the densities of CD3+ and CD8+ T-cell infiltrates (p = 0.001 and p = 0.027, respectively; Figure 4 and Table 3). Although the differences were not statistically significant, the densities of CD3+ and CD8+ T-cell infiltrates in the stromal B7-H3 mRNA-positive group were lower than those in the B7-H3 mRNA-negative group.
Relationship between stromal B7-H3 expression and infiltration of CD3+ and CD8+ T cells in phyllodes tumors.

ISH: in situ hybridization; IHC: immunohistochemistry.
Group 0 = ≤5 cells/3 hpf, group 1 = 6–50 cells/3 hpf, group 2 = 51–99 cells/3 hpf, group 3 = ≥100 cells/3 hpf.
High = group 2 and group 3.

Expression and localization of B7-H3 mRNA (a, e, i, m), B7-H3 protein (b, f, j, n), CD3+ T-cells (c, g, k, o), and CD8+ T-cells (d, h, l, p) in benign (a–h) and malignant (i–p) phyllodes tumors. The numbers of CD3+ and CD8+ T-cells (arrows) in the stromal B7-H3 positive group (a–d, i–l) were lower than those in the B7-H3-negative group (e–h, m–p). (a–p, ×400 magnification, scale bars, 60 µm.)
Discussion
Complete surgical resection with negative margins has improved the overall outlook and quality of life for women with PTs; however, a substantial fraction of women still experience recurrent or metastatic PTs, highlighting the need for new therapeutic approaches such as immunotherapy.2–6 To date, few studies have evaluated the targetable immune system in PTs of the breast. In this study, ISH and IHC were used to detect the mRNA and protein expression of B7-H3 and B7-H4 in PTs. The results showed that stromal B7-H3 mRNA and protein expression increased steadily as PTs progressed from benign to borderline and finally to the malignant grade. We found that stromal B7-H3 protein expression inversely correlated with the densities of CD3+ and CD8+ T-cell infiltrates.
Although the main standard treatment of PTs is adequate surgery with negative surgical margins, there is a significant potential for both local recurrence and distant metastasis after treatments.2–4 Owing to the high risk of treatment failure following surgical intervention alone, the addition of adjuvant radiotherapy or chemotherapy alongside surgery has been investigated; however, no consensus has been reached.4–6
Immunotherapy has become an important part of cancer treatment and involves the activation or regulation of the patient’s immune system to treat cancer.7,8 There are three main types of cancer immunotherapeutics, namely, monoclonal antibodies, cancer vaccines, and immune checkpoint inhibitors.7,8 B7-CD28 family molecules are crucial in the regulation of immune checkpoints.12,13 Programmed death-1 (PD-1) and its ligand, programmed death ligand-1 (PD-L1)/B7-H1, are members of the B7-CD28 family and this PD-1/PD-L1 pathway suppresses the antitumor immune response. PD-1/PD-L1 pathway blockade is being rapidly introduced as a therapeutic strategy for several types of cancer, including sarcoma.9–11 Recently, Gatalica et al. 5 evaluated PD-1 and PD-L1 expression in 22 malignant PTs including three metastatic tumors. The expression of PD-L1 in tumor tissues was observed in three malignant PT cases (14%) including one metastatic PT. Those authors suggested that the PD-1/PD-L1 immune checkpoint pathway can be a promising therapeutic target in cases of aggressive PTs.
B7-H3 and B7-H4 are important co-inhibitory molecules of the B7-CD28 family that have functions in cancer immune surveillance and cancer development.14,15 Both B7-H3 and B7-H4 are expressed in a variety of solid tumors and the overwhelming majority of published studies have shown correlations between high B7-H3 or B7-H4 expression and negative patient outcomes.14,15 Arigami et al. 17 evaluated B7-H3 mRNA expression in breast carcinoma by quantitative reverse transcription polymerase chain reaction and found that B7-H3 mRNA expression in primary breast cancer was a cancer progression factor and was associated with the extent of regional nodal metastasis. Meanwhile, IHC analyses have shown that B7-H3 and B7-H4 protein was highly expressed in several subtypes of breast cancer and B7-H3 and B7-H4 can be regarded as markers of poor prognosis in breast cancer.16,18,19
Among sarcomas, most of the studies on B7-H3 and B7-H4 expression have been done in osteosarcoma. B7-H3 expression was elevated in osteosarcomas of human and mice and was found to be associated with tumor aggressiveness and metastasis.20,22 Dong and Ma 21 demonstrated via IHC that B7-H4 expression in osteosarcoma was elevated and correlated with an advanced tumor stage and distant metastasis. In addition, a high expression of B7-H4 protein was an independent poor prognostic factor for overall survival time. Collectively, these studies suggest that the expression of B7-H3 or B7-H4 is associated with osteosarcoma progression and represents a useful prognostic marker in patients with osteosarcoma.
Despite extensive studies on the expression of B7-H3 and B7-H4 in several types of human cancers, the expression of B7-H3 and B7-H4 in PTs and their association with the clinicopathological features of PTs have not yet been investigated. It is useful to evaluate mRNA and protein expression together, and discriminating mRNA expression at a single-cell level within a morphological context by ISH provides information about dynamic changes in genetic expression that cannot be captured by techniques that require tissue homogenization such as quantitative reverse transcription polymerase chain reaction. 24 The RNAscope method is a significant advancement in mRNA ISH technology and the key benefits of this method are its high sensitivity and specificity.23,24 The measurement of both the mRNA and protein expression of B7-H3 and B7-H4 provides integrative information for evaluating their roles in the progression and immune surveillance of PTs. In this study, the mRNA and protein expression of B7-H3 and B7-H4 were determined by RNAscope ISH and IHC, respectively, in 60 benign, 26 borderline, and 15 malignant PTs using a TMA approach. The RNAscope ISH signals for the B7-H3 and B7-H4 probes were visualized as brown, punctate spots in the nucleus and/or cytoplasm. B7-H3 mRNA was notably expressed at high levels in the stromal component and at lower levels in the epithelial component. However, B7-H4 mRNA was negative in the stromal compartment of PTs. The staining patterns of B7-H3 and B7-H4 protein detected by IHC were concordant with those of their mRNA expression detected by ISH. Because there was no PT case with positive stromal expression of B7-H4 mRNA or protein as classified on the basis of cutoff points, we only evaluated stromal B7-H3 expression by ISH and IHC. In 101 PTs, 32 (31.7%) and 64 (63.4%) were B7-H3-positive in the stromal compartment as detected by RNAscope ISH and IHC, respectively. Although the underlying mechanism of B7-H3 upregulation in PTs remains to be elucidated, our data confirmed that the upregulation of B7-H3 mRNA and protein expression mainly occurred in the stromal component of PTs.
In this study, there was a positive correlation between stromal B7-H3 mRNA and protein expression in PTs with a concordance of 66.3%. However, 34 cases showed discrepancies between stromal B7-H3 mRNA and protein expression and can be grouped under two situations. The one is B7-H3-positive by ISH and B7-H3-negative by IHC and the other is B7-H3-negative by ISH and B7-H3-positive by IHC. In the B7-H3 mRNA-positive and B7-H3 protein-negative group, it is possible that B7-H3 mRNA was not adequately translated into protein, either because of impaired posttranscriptional processing of the mRNA transcript or the repression of translation initiation. 26 In this study, stromal B7-H3 mRNA was observed in all PTs, but it was classified as positive or negative on the basis of cutoff points. For this reason, the cases with B7-H3 mRNA-negative and B7-H3 protein-positive can be interpreted as the amount of B7-H3 mRNA is much lower than would be expected from the corresponding protein. Possible explanations include increased translation of available mRNA and decreased elimination of activator proteins in tissues. 27
In this study, stromal B7-H3 mRNA and protein expression differed among the three grades of PTs and significantly increased with the progression of PTs from benign to malignant. Stromal B7-H3 mRNA and protein expression significantly differed between borderline or malignant PTs and benign PTs but not between borderline PTs and malignant PTs. These results suggested that an increase in stromal B7-H3 expression occurs during the transition from benign to borderline PTs and presumably represents an early step in PT progression. Since the absolute number of borderline and malignant cases included in this study was small, these results need to be confirmed in additional series of cases.
Although the differences were not significant, patients with positive stromal B7-H3 mRNA or protein expression experienced disease recurrence more often than patients with negative stromal B7-H3 mRNA or protein expression. Considering the potential prognostic value of B7-H3 in patients with PTs, further studies in larger cohorts of PT cases with a longer follow-up period are needed.
Tumor-infiltrating lymphocytes are one of the major immune components that infiltrate solid tumors including breast carcinoma and sarcoma.28,29 B7-H3 has been proven to play important roles in T-lymphocyte regulation.14,15 To investigate whether a relationship exists between B7-H3 expression and T-lymphocyte infiltration, we next examined T-cell infiltration by detecting CD3+ and the CD8+ subset of cytotoxic/suppressor T-lymphocytes. In this study, stromal B7-H3 protein expression inversely correlated with the densities of CD3+ and CD8+ T-cell infiltrates. Although the differences were not statistically significant, the densities of CD3+ and CD8+ T-cell infiltrates in the stromal B7-H3 mRNA-positive group were lower than those in the B7-H3 mRNA-negative group. Previous studies also found significant inverse correlations between B7-H3 protein expression and CD8+ T-cell infiltration.20,30 Taken together, our results and those of previous studies indicate that one of the most important potential tumor-promoting effects of B7-H3 protein expression in PTs is the impairment of host T-cell-mediated immunity via the negative regulation of T-lymphocyte infiltration. B7-H3 expression in PTs can change the tumor microenvironment to reduce the numbers of infiltrating total T-lymphocytes and cytotoxic CD8+ T-lymphocytes.
In the current investigation, 69 (68.3%) and 37 (36.6%) cases were B7-H3 negative as determined by RNAscope ISH and IHC, respectively. Because various immune checkpoints are promising targets for cancer immunotherapy, 13 other immune checkpoints would also be good candidates for further investigation to develop immunotherapeutic approaches in PTs.
In conclusion, this study indicates that the co-inhibitory molecule B7-H3 is involved in the progression of PTs. The negative regulation of T-cell infiltration in PTs may be one of the main mechanisms of action of B7-H3. Our results suggest that efforts are needed to develop immunotherapeutic approaches targeting B7-H3 for the treatment of PTs.
Footnotes
Acknowledgements
G.-E.K., who is the first author, constructed the figures and tables and performed statistical analyses. N.I.K. performed histologic diagnosis. M.H.P. assisted with clinical data and experiments. J.S.L., who is the corresponding author, contributed to the preparation of the manuscript and all aspects of data collection and analysis. This article was presented in part at the 2018 USCAP Annual Meeting, Vancouver, March 17–23, 2018.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the ethics committee of Chonnam National University Hwasun Hospital under the condition of anonymization (reference: CNUHH-2017-021).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (HCRI17906-1) from Chonnam National University Hwasun Hospital Institute for Biomedical Science.