
Abstract
The vascular endothelial growth factor regulates angiogenesis that is increased in glioma. VEGF polymorphisms are thought to modulate vascular endothelial growth factor plasma levels and therefore may be implicated in glioma risk. We aimed to clarify the role of VEGF and von Willebrand factor polymorphisms in glioma susceptibility and prognosis. A case–control study of 126 glioma patients and 180 cancer-free controls was performed. Using Sequenom MassARRAY platform, 11 VEGF and 1 VWF polymorphisms were genotyped. Unconditional multivariate logistic regression models were used to calculate odds ratios and 95% confidence intervals. The associations between polymorphisms and survival were evaluated using a Cox regression model. Bonferroni’s adjustment was used to correct for multiple testing. The VEGF polymorphism rs833061 was strongly associated with increased risk for glioma (odds ratio = 164.85) and glioblastoma (odds ratio = 155.66), confirmed after Bonferroni correction. Also, the VEGF polymorphisms rs3024994, rs2010963, and particularly the homozygous carriers of rs1005230 were associated with a worse prognosis for glioma and glioblastoma. Our data support a role of VEGF and VWF polymorphisms as glioma biomarkers, with additional potential relevance for molecular stratification of patients for anti-angiogenic therapies.
Keywords
Introduction
Gliomas are the most frequent primary malignant central nervous system tumors.1–3 These tumors present a multifactorial etiology, being the result of interactions between environmental exposure and genetic susceptibility. 4 The only proven exogenous environmental cause of glioma is ionizing radiation.5,6 Perhaps other environmental causes are involved but remain to be proven. Accordingly, the genetic polymorphisms most frequently studied in the context of brain tumors are located in genes that might influence susceptibility to these tumors in concert with environmental exposures, such as those involved in DNA repair, cell cycle regulation, or immune response.7–12 In addition, few genome-wide association studies have focused on gliomas identifying five risk loci for glioma mostly related to telomerase.13–17
Common pathways in glioma biology include growth factor receptor tyrosine kinases and their signaling pathways. Polymorphisms on the epidermal growth factor (EGF) and its receptor, EGFR, have been identified as risk factors for glioma.17–19 In addition, vascular endothelial growth factor (VEGF) is the principal angiogenic factor in both embryonic development and tumor growth and is highly up-regulated in glioblastoma, and its receptors are over-expressed in tumor vessels. 20 Importantly, the anti-angiogenic drug bevacizumab, a humanized monoclonal immunoglobulin (Ig) G1 antibody that binds to and inhibits the biological activity of human VEGFA, is currently being explored in different clinical trials involving glioma and has been used in combination with chemotherapy for the treatment of recurrent glioblastoma,20–24 which resulted in improved response rates and extended progression-free survival (PFS). Recent studies have shown that some single nucleotide polymorphisms (SNPs) of VEGF/VEGF-related genes could contribute to the modulation of serum VEGF levels, possibly influencing risk and prognosis of solid tumors, including glioma.25–27 Moreover, VEGF and VEGFR2 genetic polymorphisms could predict not only patient outcome, as shown by Sjostrom et al., 28 but also the response to bevacizumab in glioblastoma patients. 29
The von Willebrand factor (VWF) is an essential component of hemostasis at sites of vascular injury. 30 The VWF gene is highly polymorphic, and SNPs have been found to influence the levels of VWF in the circulation.31,32 Moreover, VWF SNPs were also associated with lung cancer risk; however, susceptibility was related with patients’ origin.33,34
Given the important role of VEGF signaling in gliomas and the influence tumor risk and prognosis of particular VEGF/VEGFR polymorphisms in different tumor types, we investigated the relevance of 11 genetic polymorphisms in the 6p12 (VEGFA) and 6p21 (VWF) loci on glioma risk and patient survival.
Materials and methods
Study population
In this case–control study, we enrolled 126 glioma samples from Hospital S. João, Porto, and Hospital de Braga, Braga, Portugal. Tumors were classified according to the World Health Organization (WHO) criteria (Table 1). 1 All patients above 18 years of age, with diagnosis of glioma, treated between 2009 and 2010, and that by informed consent accepted to participate in the study, were included. The patients with different diagnosis or that refused to sign the informed consent were excluded. Complete treatment data were retrieved for 90 patients. Of those, 80 patients underwent surgery, 9 stereotactic biopsy, 77 radiotherapy, 71 chemotherapy (65 underwent Stupp protocol, 35 7 surgery only, 8 surgery+radiotherapy, 5 surgery+radiotherapy+chemotherapy (other than temozolomide), 2 surgery+chemotherapy, and 2 biopsy only), and one additional patient refused treatment. The 180 control samples were selected from cancer-free blood donors at Hospital de Braga, to match for gender and adjust for age in the statistical analysis (Table 1). All patients and controls had a Caucasian background and come from the same region in the north of Portugal. The follow-up information was obtained by consulting clinical records. The control group had no follow-up information. Signed informed consent was obtained from each participant. Local institutional ethics committees of Hospital S. João and Hospital de Braga approved the procedures followed in this study.
Clinico-pathological features of gliomas and controls.

WHO: World Health Organization; n.a.: not applicable; SD: standard deviation; M: male; F: female; OS: overall survival; PFS: progression-free survival.
p value for independent samples t-test, for testing differences in age and M/F ratio between controls and glioma.
Genotyping
DNA was extracted from the leukocytes of blood samples using the commercially available Citogene® Blood Kit according to the manufacturer’s recommendations. Genotyping of the allele-specific primer extension products, which were generated from amplified DNA sequences, was performed using the Sequenom MassARRAY iPLEX Gold platform (Sequenom, San Diego, CA) at the Instituto Gulbenkian de Ciência (IGC), Lisbon, Portugal. Primers were designed using MassARRAY Assay Design 3.1 software (Sequenom), and genotyping was performed in a blinded manner regarding sample status (i.e. case or control subjects). The genotyping quality was assessed by duplicate analysis of 10% of the samples, which demonstrated a 100% agreement rate.
Statistical analysis
Independent samples t-test, χ2 test, and nonparametric Wilcoxon–Mann–Whitney test were used to compare the frequency distribution of age, sex, and genotypes of VEGF and VWF and the allele distribution among the cases and controls. Moreover, the χ2 test was used to verify whether the observed allele distribution in the control group was in Hardy–Weinberg equilibrium (HWE). The odds ratio (OR) and 95% confidence intervals (95% CIs) for the effect of the polymorphic variants on the risk for glioma were estimated by multivariate logistic regression analysis, adjusted for gender and age as a continuous variable. Bonferroni’s adjustment was used to correct for multiple testing. Associations between polymorphic variants and patient survival were assessed using a multivariate Cox regression model adjusted for patient gender and age. All statistical tests were two-sided, and significance was considered for p < 0.05. Data analysis was performed using IBM® SPSS Statistics, version 20.0.
Results
Our cohort of samples included 126 glioma samples (WHO grade II–IV) and 180 cancer-free controls (Table 1). All studied variants were in HWE, apart from the polymorphism rs3025035, for which it was not possible to calculate due to the absence of the homozygous recessive genotype.
Glioma risk assessment
In order to explore the associations between VEGF and VWF variants and risk for glioma, we used an unconditional multivariate logistic regression analysis adjusted for potential confounding variables (SNP genotypes, patient age, and sex).
We could successfully include on the multivariate logistic analysis 107 cases and 143 controls. The frequencies of each genotype in controls and cases are presented in Table 2 for VEGF and VWF. The most frequent allele was used to establish the reference genotype. The control group was compared with all glioma cases (WHO grades 2–4), and also with glioblastoma (WHO grade 4), and oligodendroglioma (WHO grades 2–3; Table 2), since these were the most frequent subtypes in our series (Table 1).
Multivariate logistic regression analysis of associations between VEGF/VWF polymorphisms loci and risk for glioma groups.
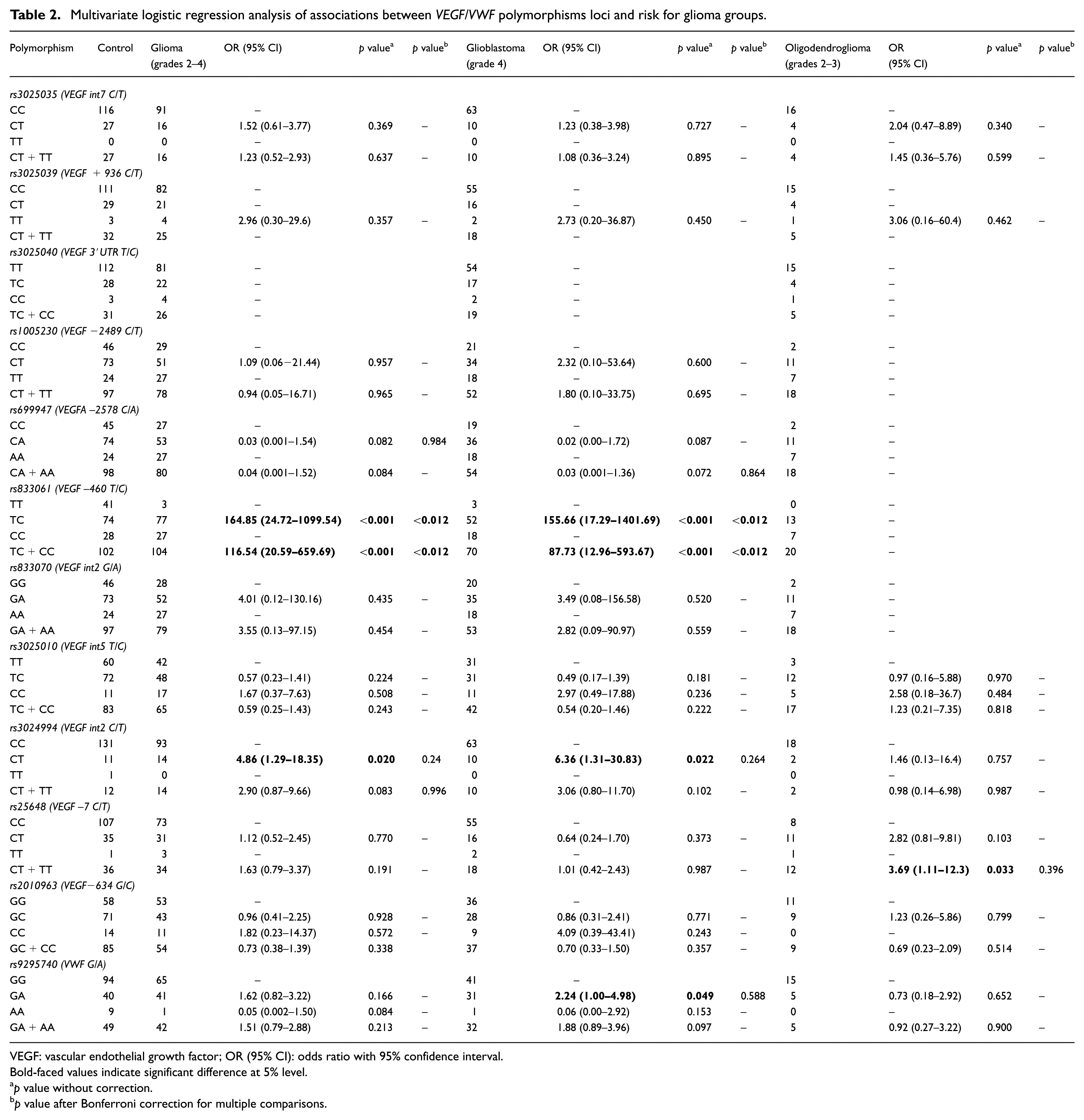
VEGF: vascular endothelial growth factor; OR (95% CI): odds ratio with 95% confidence interval.
Bold-faced values indicate significant difference at 5% level.
p value without correction.
p value after Bonferroni correction for multiple comparisons.
We found a significant association between the VEGF SNPs heterozygous rs833061 and risk for glioma and glioblastoma (OR = 164.85, 95% CI = 24.72–1099.54 and OR = 155.66, 95% CI = 17.29–1401.69, respectively, p < 0.001 and p < 0.012 after Bonferroni correction, Table 2), as well as the variant carriers of this SNP had an increased glioma and glioblastoma risk (OR = 116.54, 95% CI = 20.59–659.69 and OR = 87.73, 95% CI = 12.96–593.67, respectively, p < 0.001 and p < 0.012 after Bonferroni correction, TT vs TC+CC). Also, the heterozygous rs3024994 was associated with increased risk for glioma (OR = 4.86, 95% CI = 1.29–18.35, p = 0.020, Table 2) and glioblastoma (OR = 6.36, 95% CI = 1.31–30.83, p = 0.022, Table 2), and the rs25648 variant carriers demonstrated an increased risk for oligodendroglioma (OR = 3.69, 95% CI = 1.11–12.26, p = 0.033, Table 2); however, the significance of these results was not confirmed after Bonferroni correction (p > 0.05).
Regarding the VWF rs9295740 SNP, we observed a significant association between the heterozygous genotype and risk for glioblastoma (OR = 2.24, 95% CI = 1.00–4.98, p = 0.049, Table 2); however, the significance of this result was not confirmed after Bonferroni correction (p > 0.05).
No statistically significant associations were found between the VEGF SNPs rs3025035, rs3025039, rs3025040, rs1005230, rs699947, rs833070, rs3025010, and rs2010963 variants and risk for glioma, glioblastoma, or oligodendroglioma (Table 2; all p values > 0.05).
Glioma prognostic assessment
In a subset of glioma patients, follow-up data were also available (n = 57). The PFS of the samples was 9 months (1–48 months), and the overall survival (OS) was 16.5 months (1–52 months; Table 1). We interrogate the associations between each VEGF variant, VWF, and PFS or OS by a multivariate Cox proportional hazard model, adjusted for patient age and sex (Table 3). The heterozygous rs3025035 was significantly associated with improved PFS of glioma and glioblastoma (hazard ratio (HR) = 0.15, 95% CI = 0.03–0.73, p = 0.019 and HR = 0.11, 95% CI = 0.02–0.72, p = 0.021, respectively, Table 3). Improved PFS for glioma was also seen for the heterozygous rs3025010 and for the variant carriers of this SNP (HR = 0.23, 95% CI = 0.08–0.70, p = 0.009 and HR = 0.29, 95% CI = 0.11–0.78, p = 0.015, respectively, Table 3). On the other hand, glioma patients’ carriers of rs833061 variant (HR = 12.59, 95% CI = 1.19–38.55, p = 0.035, Table 3) and heterozygous or variant carriers of rs3024994 (HR = 6.52, 95% CI = 1.38–30.82, p = 0.018 and HR = 5.08, 95% CI = 1.30–19.81, p = 0.019, respectively, for OS and HR = 16.33, 95% CI = 2.79–95.43, p = 0.002 and HR = 6.17, 95% CI = 1.51–25.15, p = 0.011, respectively, for PFS, Table 3) had a decreased survival. However, after Bonferroni correction, only the heterozygosity of rs3024994 was found to be significantly associated with decreased survival (p = 0.024, after correction).
Multivariate Cox proportional hazard model analysis of associations between VEGF/VWF polymorphisms and glioma patient’s survival (adjusted for patient’s age and sex).
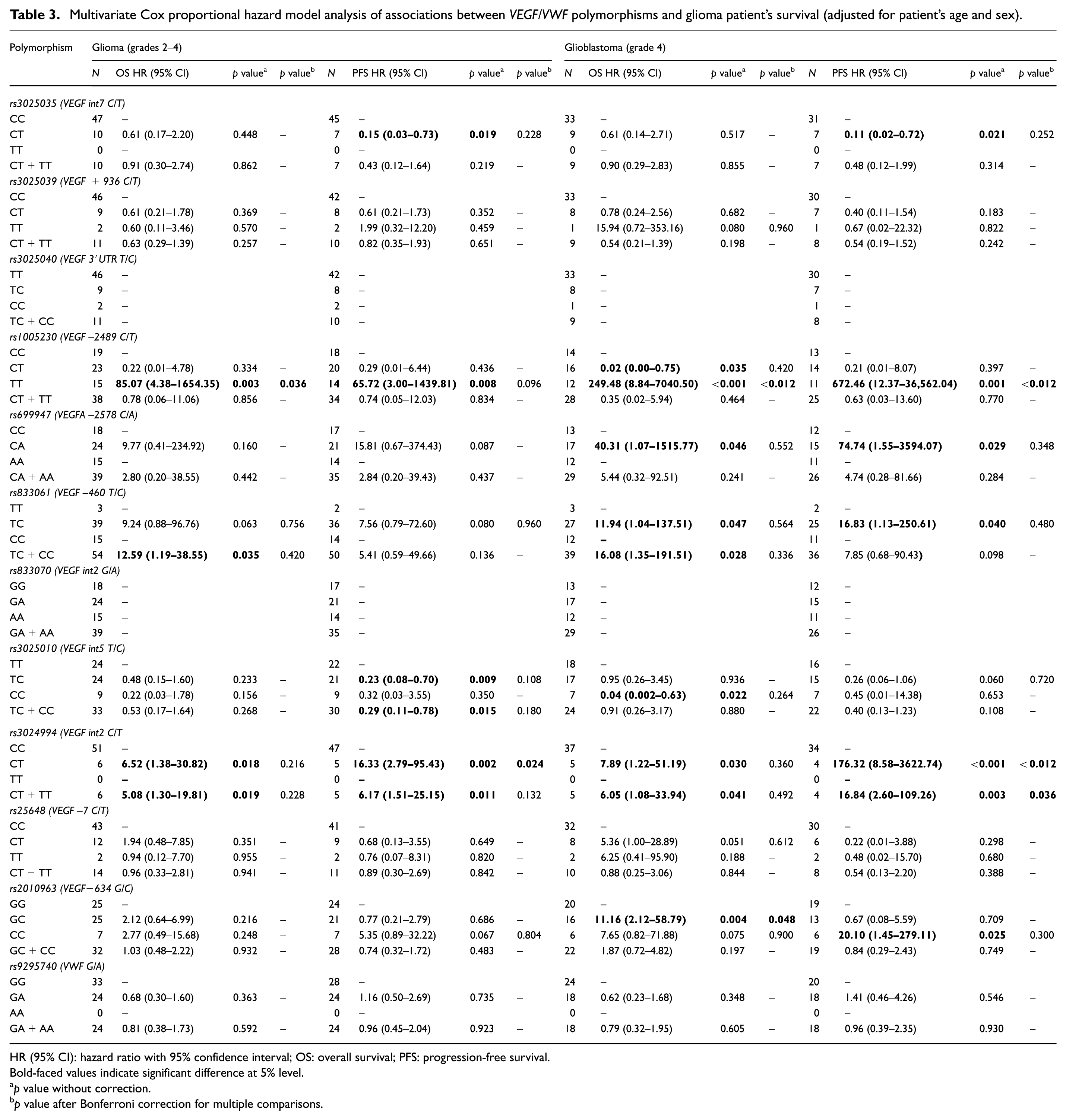
HR (95% CI): hazard ratio with 95% confidence interval; OS: overall survival; PFS: progression-free survival.
Bold-faced values indicate significant difference at 5% level.
p value without correction.
p value after Bonferroni correction for multiple comparisons.
The rs1005230 homozygous carriers presented a decreased OS and PFS both for glioma (OS: HR = 85.07, 95% CI = 4.38–1654.35, p = 0.003 and p = 0.036 after Bonferroni correction and PFS: HR = 65.72, 95% CI = 3.00–1439.81, p = 0.008 and p = 0.096 after Bonferroni correction, Table 3) and glioblastoma patients (OS: HR = 249.48, 95% CI = 8.84–7040.50, Figure 1(a) and PFS: HR = 672.46, 95% CI = 12.37–36,562.04, p < 0.001 and p < 0.012 after Bonferroni correction, Table 3). The heterozygous genotype, has shown to confer an increased OS for glioblastoma patients (HR = 0.02, 95% CI = 0.00–0.75, p = 0.035, Table 3); however, not confirmed after Bonferroni correction.

Survival graphs of significant associations between overall survival of glioblastoma patients and VEGF SNPs. Multivariate Cox proportional hazard model regression with respect to glioblastoma patient survival of (a) rs1005230, hazard ratio (HR) = 249.48; 95% confidence interval (CI) = 8.84–7040.50, p < 0.001, for TT genotype and (b) rs2010963, HR = 11.16, 95% CI = 2.12–58.79, p = 0.004.
In addition, when only glioblastoma patients were analyzed, we further observed a decreased survival for rs699947 heterozygous (OS: HR = 40.31, 95% CI = 1.07–1515.77, p = 0.046 and PFS: HR = 74.74, 95% CI = 1.55–3594.07, p = 0.029, Table 3), rs833061 heterozygous or variant carriers (OS: HR = 11.94, 95% CI = 1.04–137.51, p = 0.047 and HR = 16.08, 95% CI = 1.35–191.51, p = 0.028, respectively, and PFS: HR = 16.83, 95% CI = 1.13–250.61, p = 0.040, Table 3); however, the significance of these results was not confirmed after Bonferroni correction (p > 0.05). The rs3024994 heterozygous or variant carriers (OS: HR = 7.89, 95% CI = 1.22–51.19, p = 0.03 and HR = 6.05, 95% CI = 1.08–33.94, p = 0.041, respectively, and PFS: HR = 176.32, 95% CI = 8.58–3622.74, p < 0.001 and p < 0.012 after Bonferroni correction, and HR = 16.84, 95% CI = 2.60–109.26, p = 0.003 and p = 0.036 after Bonferroni correction, Table 3) and rs2010963 heterozygous and variant homozygous (OS: HR = 11.16, 95% CI = 2.12–58.79, p = 0.004 and p = 0.048 after Bonferroni correction, Figure 1(b) and PFS: HR = 20.10, 95% CI = 1.45–279.11, p = 0.025 and p = 0.300 after Bonferroni correction, respectively, Table 3). Finally, rs3025010 variant homozygous carriers had an improved OS for glioblastoma (HR = 0.04, 95% CI = 0.002–0.63, p = 0.022 and p = 0.264 after Bonferroni correction, Table 3).
Discussion
VEGF is the major proangiogenic factor involved in tumor growth and progression, including glioblastoma, being over-expressed in tumor vessels. 20 VEGF–VEGFR signaling pathway stimulates not only angiogenic signals but also the secretion of the VWF from endothelial cells, and VWF was described as having a potential role on angiogenesis.36–38 We have studied the contribution of 11 VEGF and 1 VWF polymorphisms to the risk and outcome of glioma and glioblastoma in the Portuguese population. These polymorphisms were selected based on some of the several studies that reported that some SNPs in the VEGF and VWF loci may conditionate serum VEGF expression modulation and therefore confer tumor risk.25–27,34,39 These polymorphisms were reported to modify VEGFA serum levels, in particular rs3025039 and rs2010963, and to modulate risk, aggressiveness prognosis of different solid tumors, specifically rs3025035, rs3025040, rs699947, rs833061, rs833070, rs3025010, and rs3024994.34,40–44 Moreover, anti-angiogenic therapies are currently in clinical use for glioma patients, and allelic variations of VEGF and VEGFR genes have being associated with glioma patient responses to those therapies. 28
We found that, in our population, the VEGF rs833061 SNP conferred an increased risk for glioma and glioblastoma. Strikingly, rs833061 T/C heterozygotes were over 150 times as likely to develop glioblastoma (OR = 155.66, 95% CI = 17.29–1401.69) or glioma (WHO grade 2–4; OR = 164.85, 95% CI = 24.72–1099.54). Although the physiological or pathological function of the SNP rs833061 in glioblastoma is still unknown, this SNP has already shown to be related to increased PFS in response to bevacizumab in combination with sorafenib in recurrent glioblastoma patients. 29
The rs3024994 C/T genotype presented an OR = 4.86 (95%CI = 1.29–18.35) for glioma and OR = 6.36 (95% CI = 1.31–30.83) for glioblastoma and also the VWF rs9295749 SNP was associated with an increased risk for glioblastoma; however, the significance of this result was not confirmed after Bonferroni correction (p > 0.05). Li et al. 27 have reported that rs3024994 variant was associated with a decreased risk, whereas rs2010963 variant carriers and rs3025039 variant homozygous had an increased risk for glioma. Also Jiang et al. 40 described rs3025039 and rs2010963 variant homozygosity to be associated with an increased risk for glioma. These discrepancies could be related to different background of the populations studied. While the previous works have studied Chinese patients, our samples are from Caucasian origin. Although no significant differences in genotype or allele frequencies are observed between different population origins, 45 it was already reported for other diseases that these polymorphisms differentially related to risk in distinctive populations.46,47
Importantly, VEGF polymorphisms have been related with patients’ response to anti-angiogenic drugs, particularly bevacizumab.29,48 Few studies have described an association between VEGF SNPs, specifically rs2010963, rs699947, rs833061, and rs1005230 and response to bevacizumab in glioblastoma patients. In particular, the rs2010963, rs699947, and rs833061 variant homozygous genotypes were associated with an increase in PFS, whereas the rs1005230 variant homozygous genotype was associated with a decrease in PFS of glioblastoma patients following bevacizumab treatment. A major limitation of our study is the small number of patients treated with bevacizumab (n = 8), which did not allow any statistical analysis to access the value of the studied polymorphisms in the context of the bevacizumab treatment. Therefore, we have also analyzed the effect of these polymorphisms on patients’ survival, independently of the treatment regimen applied.
The rs1005230 variant homozygous consistently presented a decreased OS and PFS both for glioma and glioblastoma patients. Similarly, the rs3024994 variant heterozygous consistently presented a decreased PFS both for glioma and glioblastoma patients. Also the rs2010963 heterozygous glioblastoma patients had a reduced OS.
In conclusion, our data strongly suggest that different VEGF SNPs highly increase the risk to develop gliomas, and specifically glioblastoma, particularly the presence of the rs833061 variant. Moreover, several VEGF SNPs seem to be prognostic markers of glioma and glioblastoma patients’ survival. In particular, rs3024994 heterozygous and the homozygous carriers of rs1005230 confer a worse prognosis for these patients. Although these data need confirmation by independent studies, they demonstrate that VEGF SNPs are potential glioblastoma biomarkers.
Footnotes
Acknowledgements
Paulo Linhares and Marta Viana-Pereira contributed equally to this work.
Compliance with ethical standards
This study was approved by “Comissão de tica para a Sade,” stating that it was unanimously approved, with nothing to object. Signed informed consent was obtained from each participant. Local institutional ethics committees of Hospital São João, Portugal and Hospital de Braga, Portugal, approved the procedures followed in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Fundação para a Ciência e Tecnologia (FCT), Portugal (![]() ; grant PTDC/SAU-ONC/115513/2009_FCOMP-01-0124-FEDER-015949 to R.M.R.). This article has been developed under the scope of the project NORTE-01-0145-FEDER-000013, supported by the Northern Portugal Regional Operational Programme (NORTE 2020), under the Portugal 2020 Partnership Agreement, through the European Regional Development Fund (FEDER). M.V.-P. is recipient of an FCT Post-Doctoral fellowship (ref: SFRH/BPD/104290/2014).
; grant PTDC/SAU-ONC/115513/2009_FCOMP-01-0124-FEDER-015949 to R.M.R.). This article has been developed under the scope of the project NORTE-01-0145-FEDER-000013, supported by the Northern Portugal Regional Operational Programme (NORTE 2020), under the Portugal 2020 Partnership Agreement, through the European Regional Development Fund (FEDER). M.V.-P. is recipient of an FCT Post-Doctoral fellowship (ref: SFRH/BPD/104290/2014).