
Abstract
Recent studies demonstrated a significantly increased frequency of epidermal growth factor receptor (EGFR) gene mutations in non-small cell lung cancer (NSCLC) patients with malignant pleural effusions (MPEs). The purpose of this study is to investigate the effect of first-line and second-line EGFR-tyrosine kinase inhibitors (TKIs) in the treatment of NSCLC with MPEs harboring exon 19 deletion and L858R mutation. From 2010 to 2015, 203 NSCLC patients with MPEs harboring EGFR mutation treated with EGFR-TKIs were reviewed. The efficacy were evaluated with Pearson chi-square or Fisher’s exact tests, Log-rank test and Cox proportional hazards model. The objective response rate (ORR) and disease control rate (DCR) for patients treated with first-line and second-line EGFR-TKIs were 21.9%, 91.4% and 14.7%, 85.3%, respectively. The overall median PFS and OS of enrolled NSCLC patients with MPE were 9.3 months (95% CI, 8.4–10.2 months), 20.9 months (95% CI, 18.9–22.9 months) after first-line TKIs, and 7.6 months (95% CI, 6.6–8.6 months), 15.3 months (95% CI, 13.6–15.9 months) after second-line TKIs. The exon 19 deletion arm had a longer median PFS (9.4 vs 7.1 months, p=0.003) and OS (16.8 vs 13.8 months, p=0.003) compared with the L858R mutation arm after second-line TKIs. In a conclusion, EGFR genotype was an independent predictor of PFS and OS. No significant side effects differences between the two mutation groups was observed for first or second-line EGFR-TKIs. This study demonstrated that EGFR mutations are significant predictors for advanced NSCLC patients with MPE receiving second-line EGFR-TKIs treatment.
Keywords
Introduction
Lung cancer is the most common cause of cancer-related deaths worldwide and in China.1,2 Non-small-cell lung cancer (NSCLC) accounts for approximately 87% of all lung cancer cases.3,4 Malignant pleural effusion (MPE) is one of the common complications in NSCLC patients. Approximately, 15% of lung cancer patients present with MPE at the time of initial diagnosis and 50% develop it later during the course of their disease.5,6 The presence of pleural effusion in NSCLC patients reflects the invasion of cancer cell into the pleura and usually indicates an advanced disease and a poor prognosis. 7 Evacuation of the pleural fluid followed by pleurodesis with instillation of antibiotics, antiseptics, or antineoplastics are the standard treatments to MPE.8,9 However, these management strategies did not improve patient survival since they focused only on symptom control.
The appearance of small-molecule tyrosine kinase inhibitors (TKIs) of epidermal growth factor receptor (EGFR), such as gefitinib and erlotinib, had shown antitumor activity in such patients, especially in those with EGFR mutations. Several phase-II and phase-III randomized-controlled trials (RCTs) demonstrated superior clinical benefits of TKIs compared with chemotherapy as a first-line therapy for metastatic NSCLC patients. 10 Recently, studies have demonstrated a significantly increased frequency of EGFR mutations in patients with malignant pleural/pericardial effusions compared with patients without MPE,11,12 indicating that NSCLC patients with MPEs may be more sensitive to EGFR-TKIs.
Two major activating EGFR mutations, which account for almost 85% of all clinically important mutations related to EGFR-TKIs, are in-frame deletion of exon 19 encompassing the amino acids from codons L747 to E749 and the single amino acid mutation L858R in exon 21. 13 Wu et al. 14 found that the L858R mutation rate was significantly higher in the patients with MPEs than those without (36.8% vs 20.9%; p = 0.011), and EGFR-L858R mutant enhanced lung adenocarcinoma cell invasive ability and promoted MPE formation. These results suggested that EGFR-L858R mutation may play a particular role in the development of MPE in NSCLC patients.
Studies reported that NSCLC patients with different type of EGFR mutations had varied sensitivity to EGFR-TKIs. 15 However, the sensitivity of TKIs in NSCLC patients with MPE for different EGFR mutations was less reported. So, the purpose of this study is to investigate the clinical outcomes of NSCLC patients with MPE for different EGFR tumor genotypes (exon 19 deletion vs exon 21 L858R mutation) after first-line and/or second-line EGFR-TKIs.
Patients and methods
Patients and clinical characteristics
For this cohort study, we retrospectively reviewed consecutive NSCLC patients harboring either exon 19 deletion or L858R point mutation of EGFR treated at the First Affiliated Hospital of Wenzhou Medical University between December 2010 and September 2015. The eligible criteria for this study were as follows: patients with histologically or cytologically confirmed NSCLC; with MPE at the time of initial diagnosis or after the first-line therapy; received a first- or second-line treatment with gefitinib, icotinib or erlotinib; with Eastern Cooperative Oncology Group Performance Status score of 0–3 (ECOG PS); and with adequate organ functions (including cardiac, hepatic, and renal function) and hematologic function (absolute neutrophil ≥ 1.5 × 109 L−1 or platelet count ≥ 100 × 109 L−1).
The exclusion criteria were as follows: patients had mixed small-cell or small-cell histology; unknown EGFR mutation status; without at least one measurable lesion according to the Response Evaluation Criteria in Solid Tumors (RECIST) 1.1; and lost to follow-up or died within 1 month after the beginning of the treatment.
MPE was diagnosed by cytological examinations of pleural effusions with confirmed malignant cells in pleural effusions. Patients’ gender, age, smoking status, baseline ECOG PS at the start of treatment with EGFR-TKIs, stage of the disease, the type of EGFR-TKIs administered (icotinib, gefitinib or erlotinib), and treatment and control by the first-line chemotherapy were recorded during retrospective chart review.
EGFR mutation analyses
The specimens of each patient for genetic test in this study were obtained from primary tumor or metastatic sites by either diagnostic or surgical procedures. All samples consisted of paraffin-embedded materials. Tumor cells were isolated from the normal cells through microdissection to ensure their presence in the specimens for DNA sequencing. Exons 18–21 were amplified by polymerase chain reaction and analyzed by direct sequencing to detect somatic mutations in the EGFR genes.
Treatment and follow-up evaluation
Oral EGFR-TKIs with gefitinib (250 mg/day), erlotinib (150 mg/day), or icotinib (375 mg/day) were administered as a first-line and/or second-line treatment for enrolled NSCLC patients until progression or intolerable adverse effects. Part of the patients received loca-regional treatment to evacuate the pleural fluid with or without pleurodesis together with the instillation of antibiotics, antiseptics, or antineoplastics.
Re-evaluation was performed at the beginning of oral EGFR-TKIs treatment and then monthly. Evaluation included physical examination, a complete blood count measurement, liver function test, and chest computed tomography (CT) scan. Brain CT with and without contrast, abdominal CT, or bone scan, as well as magnetic resonance images if necessary, were performed when there were relevant symptoms in patients.
Definitions and statistical analyses
Overall survival (OS) was measured from the date of the first EGFR-TKIs treatment to the death or the last follow-up visit. Progression-free survival (PFS) was calculated from the date of the first EGFR-TKIs treatment to the date of confirming disease progression or the death from disease progression. If the complete survival time of a patient was impossible to obtain or the disease did not progress, patients’ status was assumed as the last known survival and/or contact date. The baseline characteristics of parents between EGFR genotype groups and each of the potential influential factors were compared through Pearson chi-squared or Fisher’s exact tests (when there were fewer than five expected counts in the contingency table). Tumor response to EGFR-TKIs was assessed according to the RECIST 1.1. Kaplan–Meier method and log-rank test were applied to evaluate the PFS and OS. The predictive accuracy of EGFR mutations was quantified by Harrell’s concordance index (C-index), which ranges from 0.5 (no predictive power) to 1 (perfect prediction). Multivariate analyses were carried out by the Cox proportional-hazard model. The statistical analysis was computed using SPSS (version 17.0; SPSS Inc., Chicago, IL, USA) and the R stats package (R Foundation for Statistical Computing, Vienna, Austria). Tests were two sided, and p value < 0.05 was considered of statistically significant.
Result
Of 301 NSCLC patients received EGFR-TKIs as a first- or second-line treatment from December 2010 to September 2015, all patients had lung adenocarcinoma; 74 patients were excluded due to insufficient information on EGFR mutational analysis or lost to follow-up; 9 were dead within 1 month after starting the treatment of TKIs; and 15 with other types of EGFR mutations (not exon 19 and L858R mutation) were also excluded.
Table 1 presents the baseline characteristics of NSCLC patients treated by first-line and second-line TKIs. There were 128 and 75 patients enrolled receiving EGFR-TKIs as a first-line and second-line treatment, respectively. The median age was 58 years (range = 35–84 years) and 60 years (range = 38–82 years) for first-line and second-line groups, respectively. The percentage of exon 19 deletion and exon 21 L858R mutation in the first-line EGFR-TKIs patients was 45.3% (58/128) and 54.7% (70/128) and second-line EGFR-TKIs patients was 50.7% (38/75) and 49.3% (37/75), respectively. The enrolled patients were well balanced and matched according to sex, age, smoking status, Eastern Cooperative Oncology Group Performance Status (ECOG PS), tumor–node–metastasis (TNM) stage IV, type of EGFR-TKIs, and treatment.
Characteristics of patients with MPE received EGFR-TKI as first-line and second-line therapy.

MPE: malignant pleural effusions; EGFR: epidermal growth factor receptor; TKIs: tyrosine kinase inhibitors; ECOG PS: Eastern Cooperative Oncology Group Performance Status.
Table 2 shows the general response of all these patients to the first-line and second-line TKIs. For 128 patients treated with first-line EGFR-TKIs, the objective response rate (ORR) and disease control rate (DCR) were 21.9% (28/128) and 91.4% (117/128), respectively. There were 89 patients (69.5%) with stable disease and 11 (8.6%) with progressive disease. The ORR and DCR for exon 19 deletion and L858R mutation were 22.4% versus 21.4% (p = 0.89) and 93.1% versus 90.0% (p = 0.53), respectively. The overall DCR and ORR for patients treated by second-line EGFR-TKIs were 85.3% (64/75) and 14.7% (11/75), respectively. The ORR and DCR for exon 19 deletion and L858R mutation of MPE patients to second-line EGFR-TKIs were 15.8% versus 13.5% (p = 0.78) and 86.8% versus 83.8% (p = 0.71), respectively.
Response to the first-line and second-line EGFR-TKIs in NSCLC patients with malignant pleural effusions.

NSCLC: non-small-cell lung cancer; MPE: malignant pleural effusions; EGFR: epidermal growth factor receptor; TKIs: tyrosine kinase inhibitors.
After first-line TKIs, the overall median PFS and OS of enrolled NSCLC patients with MPE were 9.3 months (95% CI = 8.4–10.2 months) and 20.9 months (95% CI = 18.9–22.9 months), respectively. The estimated 1-year PFS was 24.1% in the exon 19 deletion arm and 22.6% in the L858R mutation arm, respectively. Figure 1 presents the median PFS and OS of NSCLC patients with MPE after the first-line EGFR-TKIs treatment for exon 19 deletion and L858R mutation. The exon 19 deletion group had a similar median PFS compared with the L858R mutation group (9.4 vs 8.8 months, p = 0.53, C-index = 0.52) as shown in Figure 1(a). The estimated 2-year OS was 31.5% and 24.7% for exon 19 deletion and L858R mutation group, respectively. There was also no significant difference on median OS between these two groups as shown in Figure 1(b) (25.3 vs 20.9 months, p = 0.33, C-index = 0.53).

(a) PFS and (b) OS of NSCLC patients with MPE treated by first-line EGFR-TKIs. The curves were plotted with Kaplan–Meier method and compared with log-rank test. The comparison of progression-free survival between exon 19 and 21 EGFR mutations was 9.4 versus 8.8 months (p = 0.53; C-index = 0.52). The comparison of overall survival between exon 19 and 21 EGFR mutations was 25.3 versus 20.9 months (p = 0.33; C-index = 0.53).
The median PFS and OS were 7.6 months (95% CI = 6.6–8.6 months) and 15.3 months (95% CI = 13.6–15.9 months) for NSCLC patients with MPE treated by second-line EGFR-TKIs, respectively. As shown in Figure 2(a), the probabilities of PFS at 6 months were 89.2% in the exon 19 deletions and 83.5% in L858R mutations arms, respectively. Exon 19 deletion group had a longer median PFS than the L858R mutation group (9.4 vs 7.1 months, p = 0.003, C-index = 0.67). The OS was shown in Figure 2(b), in which the probabilities of OS at 2 year were 12.3% for the exon 19 deletion arm and 5.1% for L858R mutation arm, respectively. The exon 19 deletion arm had a longer median OS compared with the L858R mutation arm (16.8 vs 13.8 months, p = 0.003, C-index = 0.69).

(a) PFS and (b) OS of NSCLC patients with MPE treated by second-line EGFR-TKIs. The curves were plotted with Kaplan–Meier method and compared with log-rank test. The comparison of progression-free survival between exon 19 and 21 EGFR mutations was 9.4 versus 7.1 months (p = 0.003, C-index = 0.67). The comparison of overall survival between exon 19 and 21 EGFR mutations was 16.8 versus 13.8 months (p = 0.003; C-index = 0.69).
Univariate and multivariate analyses on PFS and OS for NSCLC patients with MPE treated by first-line and second-line EGFR-TKIs were shown in Table 3. ECOG PS (PFS: p = 0.004; OS: p = 0.01) and TNM stage (PFS: p < 0.001; OS: p = 0.002) were independent predictors of PFS and OS for NSCLC patients with MPE treated by first-line TKIs. ECOG PS (0–1; PFS: p = 0.004; OS: p < 0.001), TNM stage (IVa; PFS: p = 0.04; OS: p = 0.007), and exon 19 deletions (PFS: p = 0.02; OS: p = 0.02) were related to a longer PFS and OS for patients treated with second-line TKIs. Gender was also an independent predictor of OS (p = 0.04) for patients treated with second-line TKIs.
Univariate and multivariate analyses on PFS and OS for NSCLC patients with MPE treated by first-line and second-line TKIs.

NSCLC: non-small-cell lung cancer; MPE: malignant pleural effusions; EGFR: epidermal growth factor receptor; TKIs: tyrosine kinase inhibitors; ECOG PS: Eastern Cooperative Oncology Group Performance Status; PFS: progression-free survival; OS: overall survival; HR: hazard ratio; CI: confidence interval.
Toxicities were reported in Table 4 for NSCLC patients treated with first-line and second-line EGFR-TKIs, in which rash (61/203), fatigue (61/203), and anorexia (34/203) were the three most frequent side effects observed. The common toxicities of grade III/IV were rash (11/203) and fatigue (10/203). Most of the patients tolerated well with the side effects of EGFR-TKI after symptomatic treatments, except for a dose reduction of EGFR-TKIs for 21 patients. There was no significant difference on side effects between NSCLC patients with exon 19 and 21 mutations in the first-line or second-line EGFR-TKIs.
Toxicity profile of the NSCLC patients with MPE treated by first-line and second-line EGFR-TKIs.
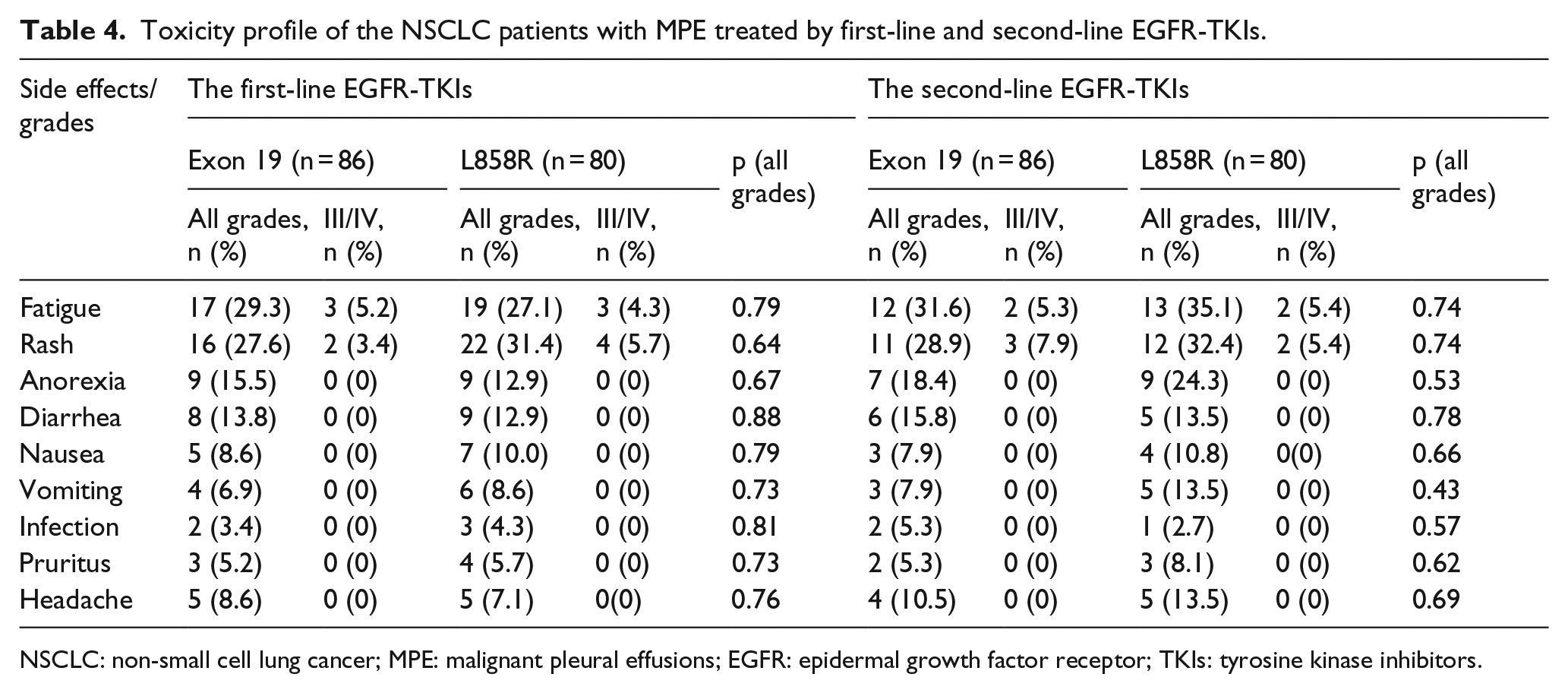
NSCLC: non-small cell lung cancer; MPE: malignant pleural effusions; EGFR: epidermal growth factor receptor; TKIs: tyrosine kinase inhibitors.
Discussion
The efficacy and different sensitivities of first-line and second-line EGFR-TKIs in the treatment of advanced NSCLC patients with MPE according to different EGFR genotype mutations were investigated in this study. There was no significant difference on PFS and OS between exon 19 and 21 mutations groups observed for NSCLC patients with MPE treated by first-line EGFR-TKIs. However, for NSCLC patients with MPE treated by second-line TKIs, patients harboring exon 19 deletion achieved a better PFS and OS compared with those harboring L858R mutation.
MPE is a common complication observed in lung cancer, especially in adenocarcinoma, because lung cancer grows in the periphery of the lung and easily invades the pleural cavity. It has been reported that more than 50% lung cancer patients developed MPE during the clinical courses and presented with poor prognosis despite of systemic and/or local therapy. 6 Previous studies demonstrated that the median OS was significantly lower in stage M1b lung cancer patients with MPE compared with those without MPE (hazard ratio (HR) = 1.49, 95% confidence interval (CI) = 1.44–1.54, p < 0.0001), and MPE was an independent factor for worse survival according to multivariate analysis (HR = 1.36, 95% CI = 1.30–1.43, p < 0.001). 16 The exact mechanisms of lung cancer cell dissemination into the pleural space have not been fully understood. A recent study indicated that this mechanism may be related to an increased mutation in EGFR-L858R, 14 which increased the importance of EGFR-TKIs significantly in the treatment of NSCLC patients with MPE. In this study, the ORR and DCR of NSCLC patients with MPE treated by the first-line EGFR-TKIs were 21.9% and 91.4%, respectively. The ORR was inferior to the reported 53.3% ORR of Korean patients with advanced pulmonary adenocarcinoma harboring EGFR mutations in a multicenter phase-II study, while the DCR in our study was similar to their reported DCR of 86.7%. 17 There was limited data for the response of NSCLC with MPE to second-line EGFR-TKIs. The ORR and DCR of our patients treated with second-line EGFR-TKIs were 14.7% and 85.3%, respectively, which were much higher than those reported 11.3% and 28.3% in a phase-II study on the EGFR wild-type NSCLC patients receiving second-line EGFR-TKIs. 18 These differences may be due to the intrinsic sensitivity differences for different type of EGFR mutations. The ORR and DCR in our study were similar to the reported 26.7% and 81.6% in the TRUST study with Chinese subpopulation. 19 However, no specific EGFR mutation types were reported, and the results of second-line and third-line treatment were mixed in that study. The median OS for patients treated with the first-line EGFR-TKIs in our study was 20.9 months (95% CI = 18.9–22.9 months), which was a bit longer than the reported 18.9 months for patients with EGFR mutations in a previous study. 20 The difference may due to the lower percentage (18%) of NSCLC patients with ECOG PS (2–3) were enrolled in our study.
Studies had shown that sensitivity to EGFR-TKIs in NSCLC is associated with somatic mutations in the EGFR genes, and different EGFR mutations showed different sensitivities to first-line EGFR-TKIs.15,17,20 Yaxiong Zhang et al. 20 revealed that the patients with exon 19 deletion had longer PFS than those with exon 21 L858R mutation under first-line TKIs therapy (HR = 0.59, p = 0.019) in a meta-analysis based on data from six clinical trials. A further clinical trial revealed that the OS benefit of afatinib, an oral irreversible ErbB family blocker, was driven mainly by patients with exon 19 positive tumors (p = 0.0001) as first-line therapy, whereas in patients with EGFR L858R-positive tumors, there was no difference between groups (p = 0.16). 15
However, according to our results of NSCLC with MPE treated by first-line EGFR-TKIs, similar median PFS and OS for patients with exon 19 deletion and L858R mutation (PFS: 9.4 vs 8.8, p = 0.53; OS: 25.3 vs 20.9, p = 0.33) were observed. The possible explanation could be that the existence of MPE reduces the sensitivity of NSCLC patients to EGFR-TKIs. Moreover, all NSCLC patients with MPE were in stage IV. So, the OS may be too short to get benefit from EGFR-TKI for the patients with exon 19 deletion. Recently, a Japanese study found that T790M was detected in nearly 87% of patients with acquired resistance to TKIs, which may be another explanation. 21
In this study, NSCLC patients with MPE harboring exon 19 deletion showed a significant higher median PFS and OS than those harboring L858R mutation receiving second-line EGFR-TKIs (PFS: 9.4 vs 7.1 months, p = 0.003; OS: 16.8 vs 13.8 months, p = 0.003). Multivariate analysis indicated that EGFR genotype was an independent predictor for PFS (p = 0.02) and OS (p = 0.02) for the NSCLC patients with MPE. Similarly, Wang et al. 22 also reported that lung adenocarcinoma patients harboring exon 19 deletions had significantly better median PFS and OS compared with those harboring exon 21 mutation (PFS: 8.1 vs 6.8 months, p = 0.002; OS: 17.6 vs 12.5 months, p = 0.000) receiving second-line TKIs. The mechanism beyond the sensitivity differences between the first-line and second-line TKIs in the treatment of NSCLC patients with MPE was unclear. A former study suggested that chemotherapy may influence EGFR mutation status in NSCLC patients, which may explain part of the difference: Bai et al. 23 found that first-line chemotherapy may significantly reduce EGFR mutation rate in NSCLC patients, and the rate of tumor response to second-line TKI therapy was lower than that for first-line therapy in patients with EGFR mutations, which was similar with the outcome of our study. Combining our outcomes of first-line and second-line TKI therapy, we speculated the reason why patients with exon 19 deletion obtained more benefit after second-line TKI was the effect of first-line chemotherapy.
One limitation of this study is that it is a retrospective methodology from a single-institution experience. The impact of various treatment-related outcomes could not be fully evaluated. The number of patients enrolled may not be sufficient enough and the follow-up duration of the study may not be long enough. External validation using other large database for evaluating the prognostic effect of first-line or second-line EGFR-TKIs in the treatment of NSCLC patients with MPE would be of value to further explore the benefit and different sensitivities of EGFR mutations.
Conclusion
With the advancements in the treatment of NSCLC, the therapy for advanced NSCLC patients with MPE gets more and more attention. Our study demonstrated that NSCLC patients with MPE harboring exon 19 deletions achieved better PFS and OS than those with L858R mutations treated with second-line TKIs treatment. EGFR mutations are significant predictors for advanced NSCLC patients with MPE receiving second-line EGFR-TKIs treatment.
Footnotes
Acknowledgements
We wish to thank statistician Changlin Zou for his expertise and great help. Z.Z. and D.X. contribute equally. Z.Z. and D.X. carried out data analyses and drafted the manuscript. H.S., B.L., L.Z., and D.X. did the follow-up; S.F. and H.C. performed the statistical analysis. X.J. and C.X. designed, coordinated, and supervised the study and critically reviewed and discussed the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. For this type of study, formal consent is not required. This article does not contain any studies with animals performed by any of the authors.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by grants from the Wenzhou Municipal Science and Technology Bureau (H20100068), National Natural Science Foundation of China (11675122), and Natural Science Foundation of Zhejiang Province (LY16H160047 and LY17H160051).