
Abstract
Nasal-type, extranodal natural killer/T-cell lymphoma is a heterogeneous disorder with poor prognosis, requiring risk stratification in this population. The combined value of baseline absolute lymphocyte count and absolute monocyte count provided prognostic information in some malignancies. However, the evidence requires validation in extranodal natural killer/T-cell lymphoma. Aiming to investigate the prognostic significance of absolute lymphocyte count/absolute monocyte count ratio and absolute lymphocyte count/absolute monocyte count prognostic score for extranodal natural killer/T-cell lymphoma, a retrospective research was carried out. A total of 264 patients with newly diagnosed extranodal natural killer/T-cell lymphoma were analyzed in this study. The patients’ absolute lymphocyte count and absolute monocyte count tested at initial diagnosis were collected. Receiver operating curve analysis showed that the optimal cut-off values for absolute lymphocyte count and absolute monocyte count were 1.0 × 109 and 0.5 × 109L−1, respectively, and for absolute lymphocyte count/absolute monocyte count ratio was 2.85. After a median follow-up of 27 months (range 1–87 months), the 3-year overall survival and progression-free survival was 75.4% and 67.6%, respectively. Patients with absolute lymphocyte count/absolute monocyte count ratio ≥ 2.85 had better 3-year overall survival and progression-free survival than those with absolute lymphocyte count/absolute monocyte count ratio <2.85 (p < 0.001). According to absolute lymphocyte count/absolute monocyte count prognostic score, significant difference has been noticed in 3-year overall survival and progression-free survival (p < 0.001) and high absolute lymphocyte count/absolute monocyte count prognostic score was associated with poorer survival. The International Prognostic Index and Korean Prognostic Index were used for prognosis and showed no significant difference. When adding absolute lymphocyte count/absolute monocyte count ratio and absolute lymphocyte count/absolute monocyte count prognostic score to the International Prognostic Index and Korean Prognostic Index model, additional prognostic information was found. These results suggest that absolute lymphocyte count/absolute monocyte count ratio and absolute lymphocyte count/absolute monocyte count prognostic score might be useful prognostic factors in extranodal natural killer/T-cell lymphoma.
Introduction
Nasal-type, extranodal natural killer/T-cell lymphoma (ENKTL) has been considered as a unique subtype of non-Hodgkin lymphoma (NHL). It is readily diagnosed in adults with the median age of 40 years, male to female: 2–4:1. ENKTL is common and accounts for 7%–10% of all NHLs in Latin America and East Asia, but only 1% in North America and Europe.1,2 ENKTL is divided into two subtypes, namely, upper aerodigestive tract NK/T-cell lymphoma (UNKTL) and extra-upper aerodigestive tract NK/T-cell lymphoma (EUNKTL). UNKTL often involves nasal cavity, paranasal sinuses, nasopharynx, and oropharynx. 3 The primary sites of EUNKTL include skin, gastrointestinal tract, bone marrow (BM), lung, orbit, adrenal gland, testis, and central nervous system.4,5 In clinical practice, ENKTL is a distinctive sickness with unsatisfied 5-year overall survival (OS) for lacking standard treatment.
Clinical risk factors serve as the foundation of treatment choices and prognostic outcome so far. The International Prognostic Index (IPI) has been universally used for prognosis in many subtypes of NHL, especially in B-cell lymphoma, but its value in ENKTL remains debatable.6–9 Lee et al. 1 proposed the Korean Prognostic Index (KPI) and thought that it was better in predictive discrimination than the IPI model. However, the prognostic value of KPI in ENKTL is not generally accepted. Subsequently, some other studies on prognostic models of ENKTL were carried out.10–13 However, no consensus has been established.
Previous studies showed that absolute lymphocyte count (ALC)14–19 and peripheral blood absolute monocyte count (AMC)19,20 at diagnosis can evaluate the prognosis in some lymphoid and hematological malignancies. Moreover, the value of the incorporation of ALC and AMC has been explored and several studies revealed that ALC/AMC ratio21–24 and ALC/AMC prognostic score (low risk and normal ALC and AMC; intermediate risk, low ALC, or high AMC; high risk, low ALC, and high AMC)19,25,26 were related to survival in certain types of lymphomas. Although there are definite results in these cancers, the role of ALC/AMC ratio and ALC/AMC prognostic score 20 in ENKTL is still unclear and requires validation in other patient cohorts. Therefore, the objective of this study was to investigate the prognostic values of ALC/AMC ratio and ALC/AMC prognostic score in ENKTL.
Patients and methods
Patients
A total of 264 consecutive patients newly diagnosed with ENKTL in West China Hospital of Sichuan University were enrolled in this study between August 2008 and May 2015. All the cases were required to meet the following criteria: (1) pathologically and immunohistochemically ascertained diagnosis of ENKTL, according to the WHO classification; 27 (2) no previous antitumor treatment; (3) no evidence of previous or attendant malignancies; and (4) sufficient clinical and laboratory data in the process of follow-up. Patients with negative Epstein-Barr virus (EBV) in situ hybridization, blastic NK-cell lymphoma/leukemia, aggressive NK-cell lymphoma/leukemia, and other subtypes of T-cell lymphomas were excluded.
Data collection
We collected clinical and laboratory data before treatment as follows: age, gender, regional lymph node (RLN) invasion, the Eastern Cooperative Oncology Group (ECOG) Performance Status (PS), B symptoms, local tumor invasiveness (LTI), BM involvement, lactate dehydrogenase (LDH) concentration, ALC, AMC, ALC/AMC ratio, ALC/AMC prognostic score, IPI and KPI indices, and Ann Arbor stage.
RLN invasion was defined according to N1, N2, or N3 of the primary tumor at tumor–node–metastasis (TNM) system (2002 TNM classification of the American Joint Committee on Cancer). 1 The definition of LTI based on the two subtypes differs significantly. For UNKTLs, LTI was defined as bony invasion or perforation or invasion of the skin.1,28 For EUNKTLs, the definition of LTI was different based on the originally involved sites. For EUNKTL primarily involving gastrointestinal tract, T4 tumor in TNM system was considered as LTI. For EUNKTL primarily involving skin or soft tissue, involvement of bone or neurovascular structure was deemed as LTI. 1 ALC/AMC ratio was determined as recorded formerly.21–24 ALC/AMC prognostic score was calculated in accordance with Wilcox’s study. 19 In general, the patients were classified into three risk groups: low risk (normal ALC and AMC), intermediate risk (low ALC or high AMC), and high risk (low ALC and high AMC). Computed tomography (CT) or magnetic resonance (MR) of nasopharynx, neck, chest, and whole abdomen or positron emission tomography/CT (PET/CT) was used to evaluate patients’ disease. The KPI system includes factors in terms of clinical stage, LDH concentration, RLN invasion, and B symptoms. 1
Treatment
For patients with stage I and II, 199 (87.7%) cases received combination of radiation and chemotherapy, 3 (1.3%) received radiotherapy alone, and 25 (11.0%) received chemotherapy alone. Patients with stage III and IV received chemotherapy alone (n = 20, 54.1%) or combined with irradiation of the primary lesion (n = 17, 45.9%). Involved-field radiotherapy was given in a total dose of 50–56 Gy, with daily fractions of 2 Gy based on conventional fractionation (five fractions per week). The treatment response was evaluated according to standard response criteria for non-Hodgkin’s lymphoma. 29
The first-line chemotherapy regimens included
Statistical analysis
The optimal cut-off values of ALC, AMC, and ALC/AMC ratio were calculated using receiver operating curve (ROC) analysis. OS was defined as the time from the date of diagnosis to the date of death or until the deadline of follow-up. Progression-free survival (PFS) was defined as the time from the date of diagnosis to the date of first occurrence of progression and relapse after response, or to the date of death from any cause, or to the date of last follow-up. Both OS and PFS were assessed by the Kaplan–Meier method. The log-rank test was used to compare the survival curves. Cox proportional hazards model was applied to determine the prognostic factors. Categorical characteristics were compared by chi-squared test. Statistical significances were considered if the two-tailed p value was less than 0.05. SPSS version 22.0 software (IBM SPSS) was used for statistical analysis.
Results
Patient characteristics
Patient characteristics were listed in Table 1. The median age was 43 years (range = 13–81 years). There was a male predominance. In all, 227 patients (86.0%) presented with localized disease (Ann Arbor stage I/II) and 37 cases (14.0%) were classified into stage III/IV. Median ALC was 1.25 × 109 L−1 (range = 0.16–3.2 × 109 L−1). Median of AMC was 0.36 × 109 L−1 (range = 0.02–1.91 × 109 L−1). Median of ALC/AMC ratio was 3.46 (range = 0.45–153.5).
Pretreatment characteristics of patients.

ECOG PS: Eastern Cooperative Oncology Group Performance Status; RLN: regional lymph node; LTI: local tumor invasion; BM: bone marrow; IPI: International Prognostic Index; KPI: Korean Prognostic Index; ALC: absolute lymphocyte count; AMC: absolute monocyte count; LDH: lactate dehydrogenase; ULN: upper limits of normal.
The optimal cut-off value for ALC singled out by the ROC analysis was 1.0 × 109 L−1 (area under the curve (AUC) value 0.658, 95% confidence interval (CI): 0.578–0.738, p < 0.001), for AMC was 0.5 × 109 L−1 (AUC 0.532, 95% CI: 0.444–0.621, p = 0.433), and for ALC/AMC ratio was 2.85 (AUC 0.627, 95% CI: 0.545–0.716, p = 0.002; Figure 1). In all, 88 (33.3%) patients had low ALC (< 1.0 × 109 L−1), 63 (23.9%) cases had high AMC (> 0.5 × 109 L−1), 166 (62.9%) of the patients had high ALC/AMC ratio ( ≥2.85), and 98 (37.1%) patients had low ALC/AMC ratio (< 2.85). According to ALC/AMC prognostic score, 130 (49.3%) patients were in the low-risk group, 117 (44.3%) in the intermediate-risk group, and 17 (6.4%) in the high-risk group.

Receiver operating curve (ROC) for determining the optimal cut-off value in predicting survival for (a) ALC, (b) AMC, and (c) ALC/AMC ratio.
Difference of patients’ characteristics classified by ALC/AMC ratio and ALC/AMC prognostic score
Comparisons of characteristics between the patients with low ALC/AMC ratio and high ALC/AMC ratio were displayed in Table 2. Significant differences were found regarding gender (p = 0.001), ECOG PS (p = 0.03), and LDH (p = 0.009). Higher ECOG PS and elevated LDH concentration seemed to be less frequent in patients with high ALC/AMC ratio.
Baseline clinical characteristics according to ALC/AMC < 2.85 versus ≥ 2.85 at diagnosis.

ECOG PS: Eastern Cooperative Oncology Group Performance Status; LTI: local tumor invasiveness; RLN: regional lymph node; BM: bone marrow; LDH: lactate dehydrogenase; ULN: upper limits of normal; IPI: International Prognostic Index; KPI: Korean Prognostic Index; ALC: absolute lymphocyte count; AMC: absolute monocyte count.
In all, 96 patients and 156 patients were eligible for curative effect assessment in ALC/AMC < 2.85 group and ALC/AMC ≥ 2.85 group, respectively.
According to ALC/AMC prognostic score, patients were stratified into three risk groups: low risk (ALC ≥ 1.0 × 109 L−1 and AMC ≤ 0.5 × 109 L−1), intermediate risk (ALC < 1.0 × 109 L−1 or AMC > 0.5 × 109 L−1), and high risk (ALC < 1.0 × 109 L−1 and AMC > 0.5 × 109 L−1). Clinical features of patients in the three risk groups were compared (Table 3). A significant difference was observed in gender, ECOG PS, LTI, B symptoms, LDH, IPI score, KPI score, therapy response rate, and percent of survived patients. Patients with high ALC/AMC prognostic score seemed to have LTI; presence of B symptoms; higher ECOG PS, IPI, and KPI scores; and elevated LDH concentration. Analogously, significant difference in therapy response rate was also found. Namely, 108 (83.1%) patients with low risk, 89 (76.1%) with intermediate risk, and 10 (58.8%) cases with high risk acquired therapy response (p = 0.025). No significant difference was found in age, Ann Arbor stage, RLN invasion, and BM involvement.
Baseline clinical characteristics according to ALC/AMC prognostic score.

ECOG PS: Eastern Cooperative Oncology Group Performance Status; LTI: local tumor invasiveness; RLN: regional lymph node; BM: bone marrow; LDH: lactate dehydrogenase; ULN: upper limits of normal; IPI: International Prognostic Index; KPI: Korean Prognostic Index; ALC: absolute lymphocyte count; AMC: absolute monocyte count.
In all, 126 patients in low-risk group, 111 patients in intermediate-risk group, and all cases in high-risk group were eligible for curative effect evaluation.
Treatment outcomes
Treatment modalities were displayed in Table 4 according to ALC/AMC ratio and ALC/AMC prognostic score grouping. No significant difference was found in regimens classified by ALC/AMC ratio (p = 0.167) or ALC/AMC prognostic score (p = 0.225). Of 264 patients, 216 patients (81.8%) received chemotherapy combined with radiation and 45 (17.0%) had chemotherapy alone. The chemotherapy regimens included VDLP (202 patients), LVP (36 patients),
First-line treatment distribution for patients with ENKTL according to ALC/AMC ratio and ALC/AMC prognostic score.

ALC: absolute lymphocyte count; AMC: absolute monocyte count.
Survival analysis and prognosis factors
After a median follow-up of 27 months (range = 1–87), 66 patients died, including 62 cases died from tumor progression and 4 died of unknown causes. The 3-year OS and PFS in whole group were 75.4% and 67.6%, respectively (Figure 2(a) and (b)).
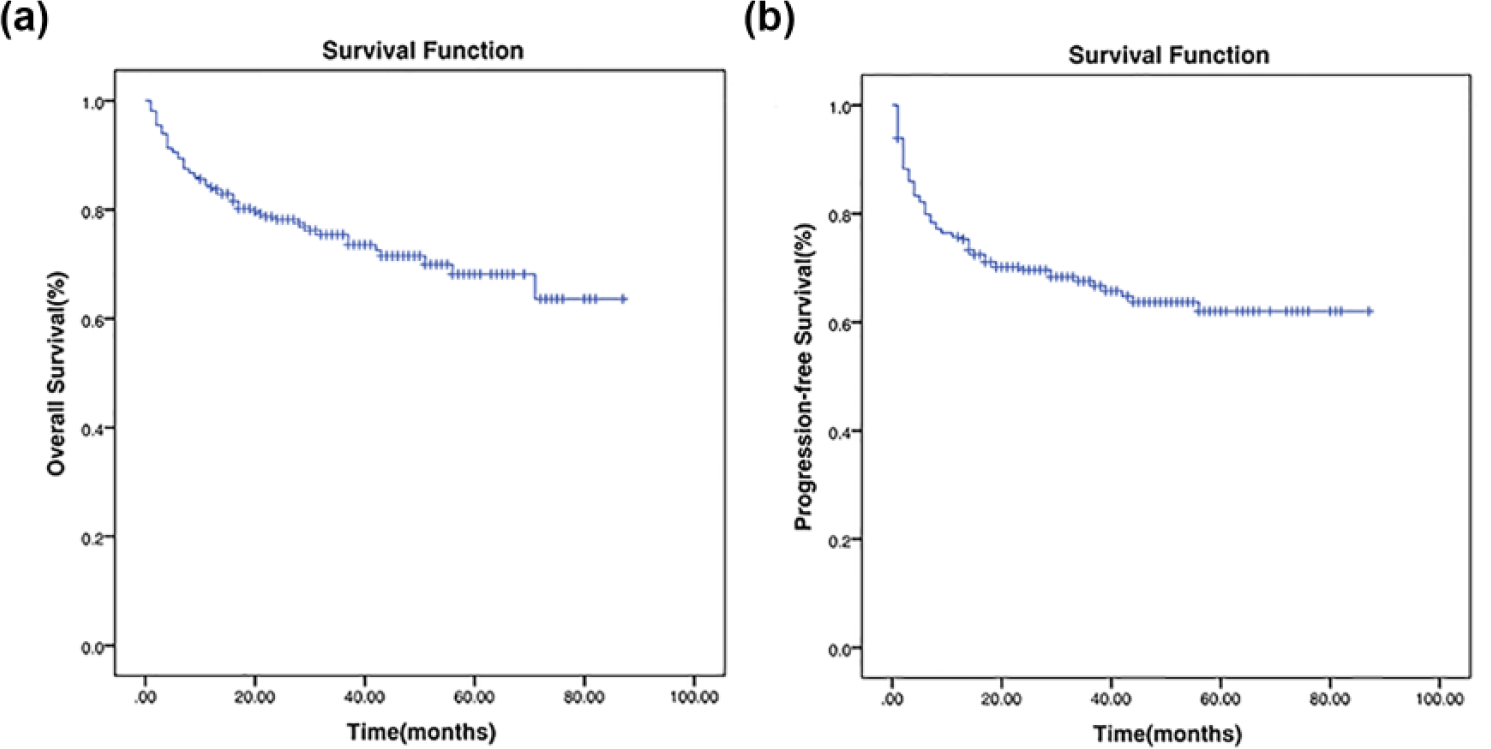
Survival curves of 264 extranodal natural killer/T-cell lymphoma patients: (a) overall survival and (b) progression-free survival.
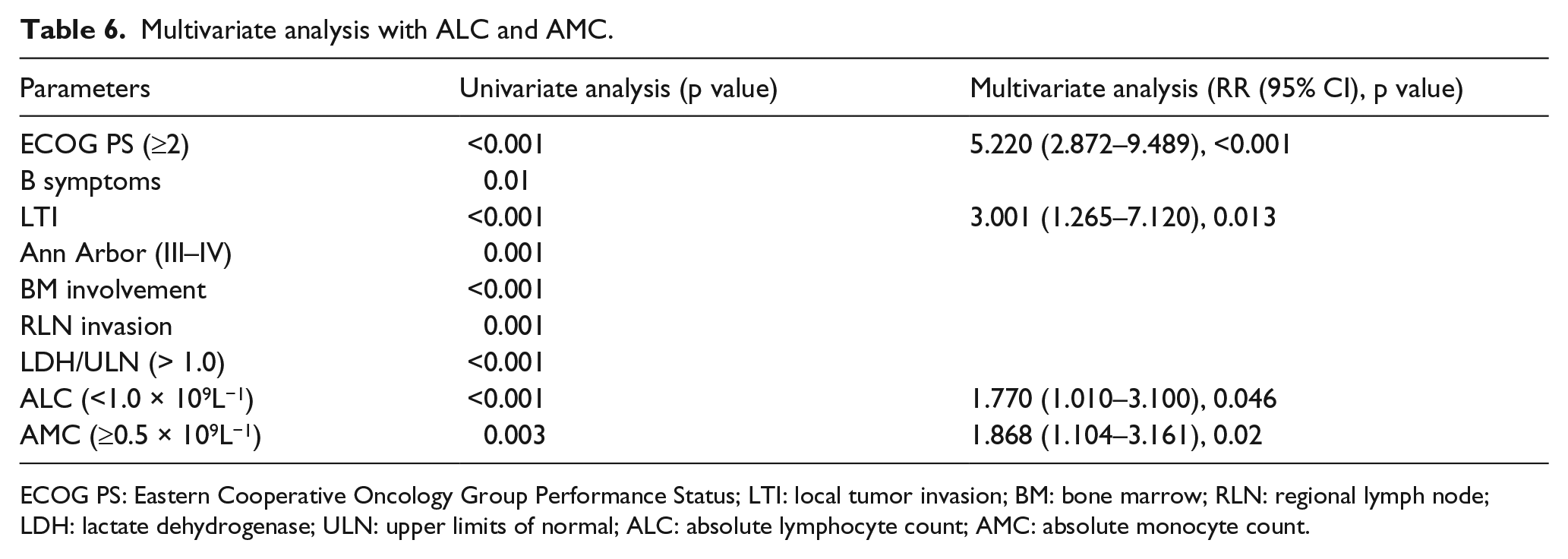
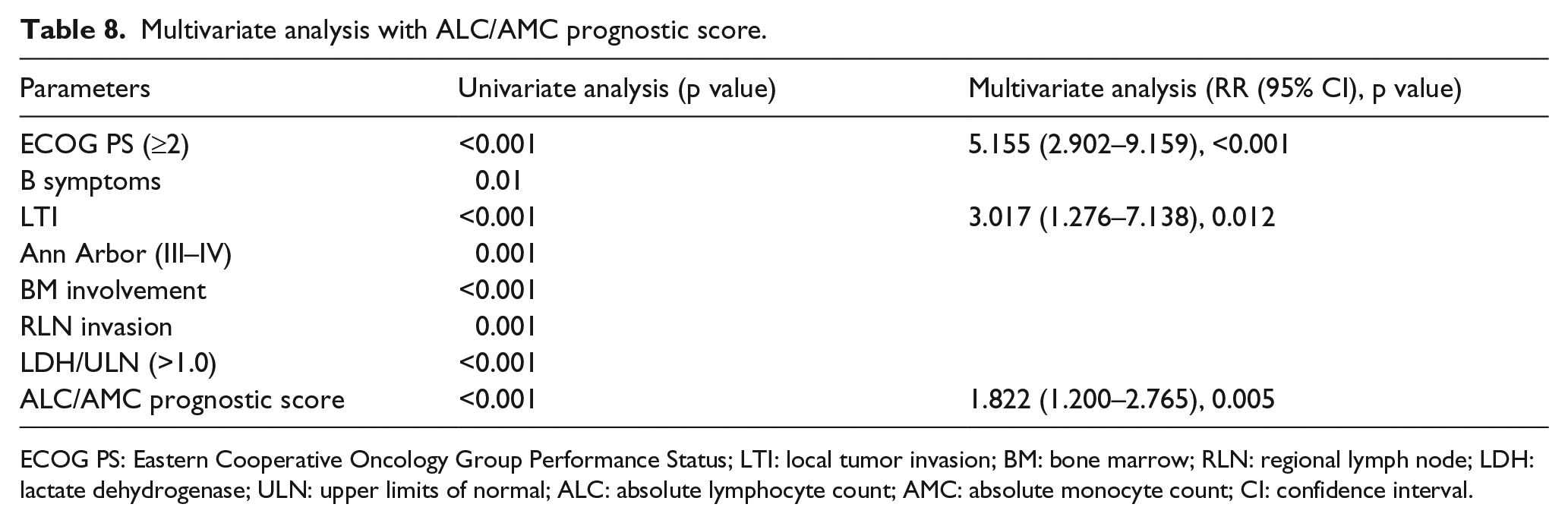
The results from univariate analysis were shown in Table 5. The poor factors for OS were as follows: Ann Arbor stage III/IV, ECOG PS ≥ 2, BM invasion, RLN involvement, presence of B symptoms, LTI, IPI score ≥ 2, KPI score ≥ 1, elevated LDH and AMC, decreased ALC, low ALC/AMC ratio, and high ALC/AMC prognostic score. All parameters except IPI and KPI scores significantly influencing prognosis in univariate analysis were included in multivariate analysis. Multivariate analysis was accomplished separately with ALC and AMC, ALC/AMC ratio, and ALC/AMC prognostic score. The result showed that ALC (p = 0.046), AMC (p = 0.02), ALC/AMC ratio (p < 0.001), and ALC/AMC prognostic score (p = 0.005) were risk factors for OS of patients with ENKTL (Tables 6–8).
Predictive features affecting overall survival in univariate analysis.

ECOG PS: Eastern Cooperative Oncology Group Performance Status; LTI: local tumor invasion; BM: bone marrow; RLN: regional lymph node; ALC: absolute lymphocyte count; AMC: absolute monocyte count; LDH: lactate dehydrogenase; ULN: upper limits of normal; IPI: International Prognostic Index; KPI: Korean Prognostic Index.
Multivariate analysis with ALC and AMC.
ECOG PS: Eastern Cooperative Oncology Group Performance Status; LTI: local tumor invasion; BM: bone marrow; RLN: regional lymph node; LDH: lactate dehydrogenase; ULN: upper limits of normal; ALC: absolute lymphocyte count; AMC: absolute monocyte count.
Multivariate analysis with ALC/AMC ratio.

ECOG PS: Eastern Cooperative Oncology Group Performance Status; LTI: local tumor invasion; BM: bone marrow; RLN: regional lymph node; LDH: lactate dehydrogenase; ULN: upper limits of normal; ALC: absolute lymphocyte count; AMC: absolute monocyte count; CI: confidence interval.
Multivariate analysis with ALC/AMC prognostic score.
ECOG PS: Eastern Cooperative Oncology Group Performance Status; LTI: local tumor invasion; BM: bone marrow; RLN: regional lymph node; LDH: lactate dehydrogenase; ULN: upper limits of normal; ALC: absolute lymphocyte count; AMC: absolute monocyte count; CI: confidence interval.
The prognostic value of AMC/ALC ratio and ALC/AMC prognostic score
For whole group, patients with ALC/AMC ratio ≥ 2.85 had better 3-year OS (83.4% vs 61.9%, p < 0.001) and PFS (76.5% vs 53.0%, p < 0.001) than those with ALC/AMC ratio < 2.85 (Figure 3(a) and (b)). Similarly, in the groups of patients with different ALC/AMC prognostic scores, significant difference on 3-year OS (low risk vs intermediate risk, 88.3% vs 66.5%, p = 0.001; low risk vs high risk, 88.3% vs 0%, p < 0.001; intermediate risk vs high risk, 66.5% vs 0%, p = 0.001; Figure 3(c)) and PFS (low risk vs intermediate risk, 80.7% vs 58.3%, p = 0.002; low risk vs high risk, 80.7% vs 0%, p < 0.001; intermediate risk vs high risk, 58.3% vs 0%, p = 0.003; Figure 3(d)) also has been noticed.

Survivals stratified by ALC/AMC ratio: (a) overall survival and (b) progression-free survival. Survivals stratified by prognostic score: (c) overall survival and (d) progression-free survival.
In order to control confounding factors, 193 patients who had stage I and II and received
The AMC/ALC ratio and ALC/AMC prognostic score provide additional prognostic information when being superimposed on the IPI and KPI
According to the IPI category, patients were unevenly allocated in the four risk groups. 80.3% of them were allocated into the low-risk group. The 3-year OS was 82.5% for low risk, 62.4% for low-intermediate, 31.3% for high-intermediate, and 25.0% for high-risk group. Survival differences in the four risk groups were observed. However, no significant difference was found between high-intermediate and high-risk groups (p = 0.968). The KPI model balanced distribution of patients into different risk groups better than IPI did. The 3-year OS was 91.2% for low risk, 77.2% for low-intermediate risk, 70.7% for high-intermediate risk, and 50.5% for high-risk group. But no significant difference for survival was observed between the low-intermediate and high-intermediate risk groups (p = 0.476).
ALC/AMC ratio and ALC/AMC prognostic score were separately added to the IPI and KPI system. In IPI low-risk group, 3-year OS for high ALC/AMC ratio and low ratio groups were 88.8% and 71.6% (p < 0.001), respectively, and for low-, intermediate-, and high-risk groups, ALC/AMC prognostic score was 90.8%, 73.6%, and 0%, respectively (p = 0.023). Similarly, the ALC/AMC ratio and ALC/AMC prognostic score were also efficient in discriminating 3-year OS rates in patients with KPI low- to high-intermediate risk group (84.7% vs 60.1%, p < 0.001; 87.6% vs 65.5% vs 0%, p = 0.011). However, the ALC/AMC ratio did not differentiate outcomes in patients with IPI high-intermediate to high-risk groups (p = 0.131). The ALC/AMC prognostic score differentiated high-intermediate risk group from high-risk patients according to the IPI, with borderline significance (p = 0.055).
Discussion
Host adaptive immunity and the tumor microenvironment were found to be related to occurrence of lymphoma.30,31 Epidemiologic studies discovered that immunodeficiency increased the probability of NHL.31–34 Lymphocytes are mediators of antibody-dependent cell-mediated cytotoxicity 35 and are indicators of host immune activity. 17 Monocytes generate host antitumor immune suppression and play an important part in tumor angiogenesis, which promote cell proliferation and tumor invasion.30,36,37 Antecedent evidence verified that ALC and AMC were parameters to predict outcomes in several types of cancer.14–20,38–42 ALC and AMC have been studied as combined factors in Hodgkin’s lymphoma and diffuse large B-cell lymphoma.19,21–26 Results showed that ALC/AMC ratio and AMC/ALC prognostic scores seemed to be associated with outcomes. However, the evidence in ENKTL was insufficient. 20
Rambaldi et al. 22 found that ALC/AMC ratio has a strong prognostic relevance and is a risk factor from the IPI when rituximab is added to chemotherapy in diffuse large B-cell lymphoma. Similar results were shown in other cohorts.21,23,24 However, the standard value varies in different reports. Consistent with previous studies, we conducted an ROC method suggesting that the most discriminatory threshold value of ALC/AMC ratio was 2.85, which is similar to Markovic’s research. 24 Both univariate and multivariate analyses demonstrated that ALC/AMC ratio at this cut-off was a prognostic factor. Our data discovered a significant difference in clinical outcome between the high and low ALC/AMC ratio groups (Figure 3(a) and (b)). Furthermore, patients in the group with low ALC/AMC ratio tended to have adverse features, including poorer ECOG PS and higher frequent LDH concentration.
Wilcox et al. 19 first described the role of AMC/ALC prognostic score in diffuse large-B-cell lymphoma. Subsequent evidence also investigated the prognostic value of ALC/AMC prognostic score in diffuse large-B-cell lymphoma.24–26 Significant difference in clinical outcome was noticed in the patients with different ALC/AMC prognostic scores and high score was related to poor survival. We stratified patients into three risk categories with significantly different survival outcomes according to AMC/ALC prognostic score. High AMC/ALC prognostic score was associated with inferior 3-year OS and PFS (Figure 3(c) and (d)). Besides, patients with high ALC/AMC prognostic score readily had disadvantageous characteristics in terms of LTI, B symptoms, poor ECOG PS, and low therapy response rate.
The prognostic role of IPI index has been confirmed in diffuse large B-cell lymphoma and many other subtypes of NHL. Previous studies explored the value of the IPI in ENKTL, but the results remain controversial.6–9 In our study, 80.3% of all patients were in the low-risk IPI category, and this model failed to differentiate patients with different outcomes in the low-risk group. Moreover, the IPI did not discriminate well between patients in the high-intermediate and high-risk groups. The KPI model was first put forward on the basis of anthracycline-based drugs chemotherapy, 1 which has been considered unsuitable for ENKTL. Up to now, the value of the KPI in ENKTL is still disputable. In this study, the KPI balanced the distribution of patients into four risk groups with different outcomes. However, it failed to significantly discriminate survival between the low-intermediate and high-intermediate risk groups. When adding AMC/ALC ratio and ALC/AMC prognostic score separately to the two models, superior predictive results were found.
Conclusion
To the best of our knowledge, this study is the largest to evaluate the prognostic value of ALC/AMC ratio and ALC/AMC prognostic score in ENKTL patients. In addition, this is the first to estimate the value of ALC/AMC ratio in predicting prognosis in ENKTL. Our results suggested that ALC/AMC ratio and ALC/AMC prognostic score could be usefully prognostic parameters for patients with ENKTL and should be included in the prognosis system.
However, on account of the limited number of patients and retrospective and single-institution study, the significance of these parameters requires to be further validated in multicenter studies with larger sample.
Footnotes
Acknowledgements
The authors thank the medical, nursing, and clinical laboratory staff in West China Hospital of Sichuan University for their commendable contributions to this study. N.L. and L.Z. contributed equally to this article. L.Z. designed the research. N.L. collected and analyzed data, performed research, and wrote the paper. L.Z. contributed vital new reagents and analyzed data. H.S. performed statistical analysis. J.Z. collected data. H.W. analyzed and interpreted data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.