
Abstract
Whole brain radiotherapy has been a standard treatment of brain metastases. Stereotactic radiosurgery provides more focal and aggressive radiation and normal tissue sparing but worse local and distant control. This meta-analysis was performed to assess and compare the effectiveness of whole brain radiotherapy alone, stereotactic radiosurgery alone, and their combination in the treatment of brain metastases based on randomized controlled trial studies. Electronic databases (PubMed, MEDLINE, Embase, and Cochrane Library) were searched to identify randomized controlled trial studies that compared treatment outcome of whole brain radiotherapy and stereotactic radiosurgery. This meta-analysis was performed using the Review Manager (RevMan) software (version 5.2) that is provided by the Cochrane Collaboration. The data used were hazard ratios with 95% confidence intervals calculated for time-to-event data extracted from survival curves and local tumor control rate curves. Odds ratio with 95% confidence intervals were calculated for dichotomous data, while mean differences with 95% confidence intervals were calculated for continuous data. Fixed-effects or random-effects models were adopted according to heterogeneity. Five studies (n = 763) were included in this meta-analysis meeting the inclusion criteria. All the included studies were randomized controlled trials. The sample size ranged from 27 to 331. In total 202 (26%) patients with whole brain radiotherapy alone, 196 (26%) patients receiving stereotactic radiosurgery alone, and 365 (48%) patients were in whole brain radiotherapy plus stereotactic radiosurgery group. No significant survival benefit was observed for any treatment approach; hazard ratio was 1.19 (95% confidence interval: 0.96–1.43, p = 0.12) based on three randomized controlled trials for whole brain radiotherapy only compared to whole brain radiotherapy plus stereotactic radiosurgery and hazard ratio was 1.03 (95% confidence interval: 0.82–1.29, p = 0.81) for stereotactic radiosurgery only compared to combined approach. Local control was best achieved when whole brain radiotherapy was combined with stereotactic radiosurgery. Hazard ratio 2.05 (95% confidence interval: 1.36–3.09, p = 0.0006) and hazard ratio 1.84 (95% confidence interval: 1.26–2.70, p = 0.002) were obtained from comparing whole brain radiotherapy only and stereotactic radiosurgery only to whole brain radiotherapy + stereotactic radiosurgery, respectively. No difference in adverse events for treatment difference; odds ratio 1.16 (95% confidence interval: 0.77–1.76, p = 0.48) and odds ratio 0.92 (95% confidence interval: 0.59–1.42, p = 71) for whole brain radiotherapy + stereotactic radiosurgery versus whole brain radiotherapy only and whole brain radiotherapy + stereotactic radiosurgery versus stereotactic radiosurgery only, respectively. Adding stereotactic radiosurgery to whole brain radiotherapy provides better local control as compared to whole brain radiotherapy only and stereotactic radiosurgery only with no difference in radiation related toxicities.
Keywords
Introduction
Brain metastases occur in 24%–45% of patients with systemic cancers every year 1 and is the most common intracranial neoplasms in adults. 2 The most common primary tumors that metastasize to the brain are melanoma, lung, breast, and renal cancer.1,2 The outcome for the patients with brain metastases is generally poor, with median survival time of 1–2 months with corticosteroids and up to 6 months with whole brain radiotherapy (WBRT).3–6
Postoperative WBRT for patients with single metastasis reported less recurrence as compared to surgery alone. 7 For accessible single brain metastasis, surgical resection followed by WBRT has been compared to WBRT alone.5,6,8 Two of these randomized trials found a survival benefit after surgical resection plus WBRT versus WBRT alone.9–11
Radiosurgery focuses high doses of radiation beams more closely to the tumor than conventional external beam radiation in an attempt to avoid and protect normal surrounding brain tissues. This approach is most commonly used in situations where the tumor is small (3 cm or less in diameter and limited in number) and in eloquent regions of the brain, for example, speech and motor localized areas. Radiosurgery can also be used to treat tumors that are not accessible with surgery, such as those deep within the brain. Outcomes for patients with single solid metastatic brain tumors amenable to either surgical resection or stereotactic radiosurgery (SRS) have been shown to be roughly equivalent for both local control and overall patient survival.12–15
Limited intracranial disease status and long-term adverse effects following WBRT brings SRS role in treating brain metastases which delivers high-dose focal radiation and can be used for recurrences if whole brain radiation was previously given or as a local “boost” following whole brain radiation.5,6,8,16–18 SRS may result in superior local control rates for radioresistant lesions (e.g., renal cell, melanoma, etc.) as well and may allow WBRT to be deferred for subsequent salvage treatment without adverse sequelae.
The current standard of care for patients with brain metastasis consists of WBRT and/or SRS and/or surgery.1–11,16–18 However, controversy still exists regarding selection of the optimal treatment regimen. This review summarizes the high level evidence available to compare the outcomes of WBRT, SRS, and their combination in the treatment of newly diagnosed single/multiple brain metastases. Outcomes are compared to show significance and effectiveness of each of the treatment.
Methods
Research method
The following electronic databases (PubMed, MEDLINE, Embase, and Cochrane Library) were searched up to Jan 2017 using various combinations of MeSH headings and keywords such as “brain metastasis,” “radiotherapy,” “radiosurgery,” “gamma knife,“ “cyberknife,” “linac,” “whole brain radiotherapy,” “whole brain irradiation,” and “stereotactic radiosurgery,” without restricting languages. Moreover, the references of all the identified eligible articles were manually searched for additional relevant citations.
Inclusion criteria
Studies published in English.
Only randomized controlled trials (RCTs) were eligible for inclusion in the review and meta-analysis.
RCTs that compared any of the following interventions were eligible for inclusion: WBRT versus WBRT plus SRS, SRS versus WBRT versus WBRT plus SRS, and SRS alone versus SRS plus WBRT.
Patients who had been diagnosed with one or more brain metastases less than 4 cm in diameter.
Participants were eligible regardless of the primary tumor histology and status as long as they had not received prior cranial irradiation.
Outcomes assessed
The meta-analysis evaluated WBRT alone versus WBRT plus SRS and SRS alone versus SRS plus WBRT. The primary outcomes were overall survival following treatment, quality of life (QOL) measured using a validated health-related QOL scale, and neurocognitive function.
The secondary outcomes were local tumor control rate, neurological death, and adverse effects defined as acute/early (within 90 days of treatment) or late/delayed (after 90 days of treatment) morbidity.
Study quality assessment
Two reviewers independently assessed validity of the studies and evaluated the bias of each study using the Cochrane tools. 19 The assessment item included sequence generation, allocation of sequence concealment, blinding of participants and personnel, blinding of outcomes and assessments, incomplete outcome data, selective outcome reporting, and other biases. Disagreements were resolved through discussion.
Data extraction
Two reviewers extracted the data from all eligible RCTs. Median survival and local tumor control rates were extracted either directly or from survival curves, and hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated for time-to-event data. 20 Data on other outcomes of interest were also extracted. All available data were extracted from relevant texts, tables, and figures. All analyses were performed on an intention-to-treat basis. Any disagreements in study selection were resolved through discussion.
Statistical analysis
This meta-analysis was performed using the Review Manager (RevMan) software v 5.2, provided by Cochrane Collaboration. Pooled HRs with 95% CIs were calculated for time-to-event data using fixed-effects model. Weighted mean differences with 95% CIs were calculated for continuous data, while pooled Odds ratio with 95% CIs were calculated for dichotomous data. Statistical heterogeneity was assessed using the chi-square statistics.
Results
A total of 1365 relevant studies were screened. Forty-two studies passed through title and abstract screening. After full-text screening, five studies (n = 763) were finally selected for inclusion in this meta-analysis meeting the inclusion criteria (Figure 1). All the included studies were RCTs. The sample size ranged from 27 to 331. In total, 202 (26%) patients underwent WBRT alone, 196 (26%) patients underwent SRS alone, and 365 (48%) patients were in WBRT plus SRS group. General characteristics of the studies are listed in Table 1 and extracted data are given in Table 2.
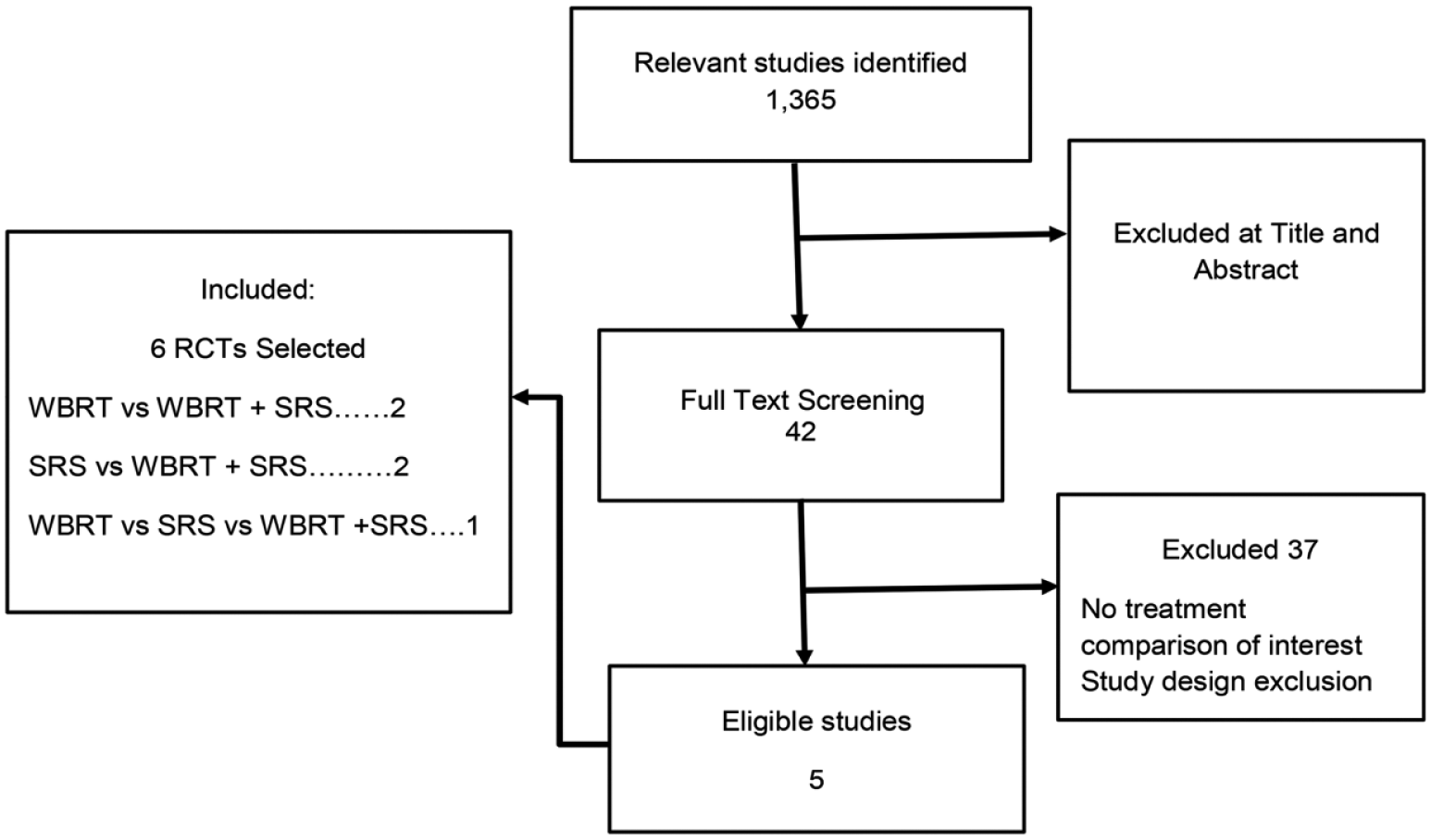
Flow chart of the literature research.
General characteristics of included studies.

RCT: randomized controlled trial; WBRT: whole brain radiotherapy; SRS: stereotactic radiosurgery; f: fraction; BM: brain metastases.
Extracted data from the studies included.
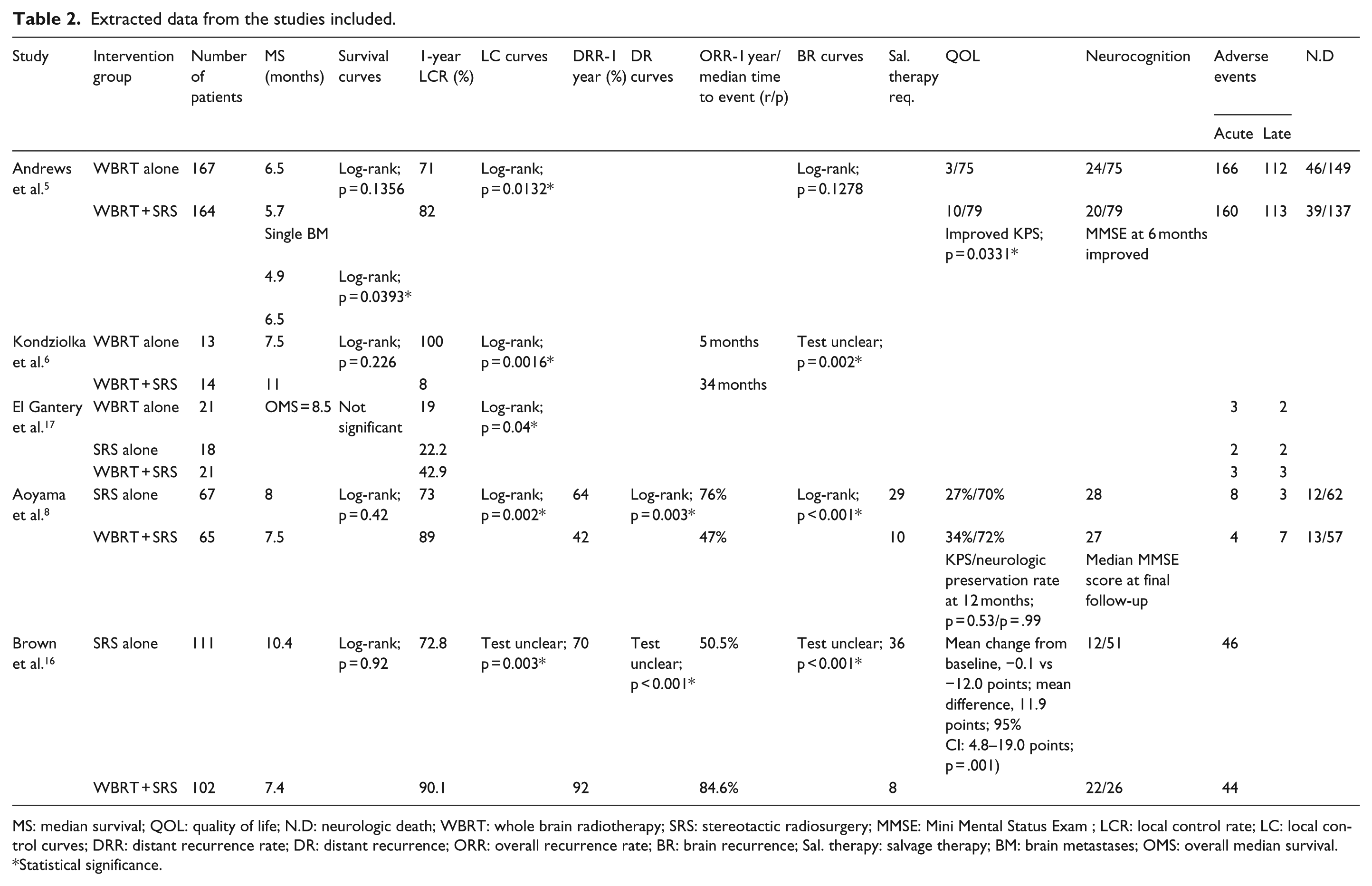
MS: median survival; QOL: quality of life; N.D: neurologic death; WBRT: whole brain radiotherapy; SRS: stereotactic radiosurgery; MMSE: Mini Mental Status Exam ; LCR: local control rate; LC: local control curves; DRR: distant recurrence rate; DR: distant recurrence; ORR: overall recurrence rate; BR: brain recurrence; Sal. therapy: salvage therapy; BM: brain metastases; OMS: overall median survival.
Statistical significance.
Studies included were well matched for baseline information. Lung cancer was the primary tumor site followed by breast cancer. Adenocarcinoma followed by squamous cell carcinoma was the primary tumor histology. Patients were well matched for Karnofsky Performance Scale (KPS) score, Recursive Partitioning Analysis (RPA) classes, and primary tumor status (stable/unstable) in all the studies. Baseline characteristics of the participants are outlined in Tables 3 and 4.
Baseline characteristics of the participants in the included randomized controlled trials.

WBRT: whole brain radiotherapy; SRS: stereotactic radiosurgery ; RPA: recursive partitioning analysis; KPS: karnofsky performance scale.
Baseline characteristics of the participants in the included randomized controlled trials.

WBRT: whole brain radiotherapy; SRS: stereotactic radiosurgery.
Bias assessment
In all the studies neither the patients nor clinicians were blinded. Assessments of risk bias are illustrated in Figures 2 and 3.

Risk of bias graph.

Risk of bias summary.
Review and meta-analysis
Overall survival
WBRT versus WBRT plus SRS
Pooled data revealed no statistically significant difference between the treatments for survival outcome. HR was 1.19 (95% CI: 0.96–1.43, p = 0.12) based on three RCTs (Figure 4). Significant survival benefit was reported in WBRT plus SRS group in patients with single metastases compared to WBRT alone but there was no difference between the treatment groups in patients with multiple metastases (one RCT, n = 331). Overall, better survival was reported for patients with single brain metastases compared to patients with multiple brain metastases regardless of the treatment.

Meta-analysis of the overall survival shown as forest plot between WBRT (whole brain radiotherapy) alone and WBRT plus SRS (stereotactic radiosurgery). Hazard ratios with 95% CI are shown.
SRS versus WBRT plus SRS
No statistically significant difference was revealed in survival between the treatments; the HR was 1.03 (95% CI: 0.82–1.29, p = 0.81) based on three RCTs (Figure 5). There was no data available for comparing patients with single brain metastases or multiple metastases with regard to treatments. However, better survival was reported for patients with single brain metastases compared to patients with multiple brain metastases regardless of the treatment.

Meta-analysis of the overall survival shown as forest plot between SRS (stereotactic radiosurgery) alone and WBRT (whole brain radiotherapy) plus SRS. Hazard ratios with 95% CI are shown.
Quality of Life
QOL has not been investigated as an independent treatment outcome using a specific measure. A few different measures have been used encompassing physical well being (KPS score, neurologic function preservation), neurocognitive function, and so on.
WBRT versus WBRT plus SRS
QOL was significantly better at 6-month follow-up in patients receiving WBRT plus SRS (one RCT n = 331). Patients receiving additional radiosurgery reported significantly improved KPS score (patients with improved KPS score: WBRT + SRS (10/79) vs WBRT (3/75), p = 0.0331) and decreased steroid use (patients with decreased steroid use: WBRT + SRS (41/76) vs WBRT (25/75), p < 0.0158). However, no significant difference was observed in mental status outcome at 6-month follow-up between treatments.
SRS versus WBRT plus SRS
One RCT (n = 213) assessed QOL using Functional Assessment of Cancer Therapy-Brain (FACT-B), the only RCT assessing QOL using specific measure (FACT-B score ranges from 0–200, high score represent better QOL). At 3-month follow-up, there was better QOL with SRS alone (overall QOL mean change from baseline: −0.1 vs −12.0, p = 0.001). In long-term survivors (surviving 12 months) only one index of QOL was significantly different favoring SRS at 3-month evaluation (physical well being, mean change from baseline: −9.6 vs −40.2, mean difference: −30.6 points, 95% CI: −53.9 to −7.3 points, p = .01).
Another RCT (n = 132) reported no significant difference between the treatments at 12-month follow-up. Systemic functional preservation rate (KPS score >70, WBRT + SRS (33.9%) vs SRS (26.9%), p = 0.53) and neurologic preservation rate (WBRT + SRS (72.1%) vs SRS (70.3%), p = 0.99) at 12-month follow-up were evaluated and no difference between the treatments was observed.
Neurocognitive function
Two of the RCTs evaluated the neurocognitive function using the Mini Mental Status Exam (MMSE). Another RCT specifically aimed at neurocognitive function comparing SRS alone with WBRT plus SRS used a range of cognitive tests to evaluate neurocognitive function of the patients following treatment.
WBRT versus WBRT plus SRS
There was no statistically significant difference between the two groups in mental status at a 6-month follow-up based on one RCT (n = 331).
SRS versus WBRT plus SRS
One RCT (n = 213) evaluating neurocognitive function deterioration as the primary outcome using a wide range of tests. At 3-month follow-up cognitive deterioration was less frequent after SRS alone (SRS (40/63) vs WBRT + SRS (44/48), p < .001). In long-term survivors (n = 34, patients surviving 12 months), RCT reported the incidence of cognitive deterioration (at least a 1 standard deviation (SD) decrease in 1 test score) was less after SRS alone at 3-month follow-up (SRS (5/11) vs WBRT + SRS (16/17), p = 0.007) and at 12-month follow-up (SRS (6/10) vs WBRT + SRS (17/18), p = 0.04).
Another RCT (n = 132) evaluated the mental status at 12-month follow-up, and no difference between the groups was reported (MMSE median score: WBRT + SRS (28) vs SRS (27))
Local control rate and distant recurrence
WBRT versus WBRT plus SRS
Meta-analysis for local tumor control revealed a significant difference between the treatments. Patients receiving SRS boost were less likely to have lost tumor control; pooled data revealed a combined HR 2.05 (95% CI: 1.36–3.09, p = 0.0006) based on three RCTs (Figure 6).

Meta-analysis of the local tumor control shown as forest plot between WBRT (whole brain radiotherapy) alone and WBRT plus SRS (stereotactic radiosurgery). Hazard ratios with 95% CI are shown.
SRS versus WBRT plus SRS
The pooled HRs revealed significantly better control for patients receiving SRS boost; the HR was 1.84 (95% CI: 1.26–2.70, p = 0.002) for local control and 1.71 (95% CI: 1.20–2.44, p = 0.003) for distant brain recurrences with an overall HR of 1.93 (95% CI: 1.52–2.45, p < 0.00001) for overall brain tumor control (Figure 7). Also, significantly higher number of patients required salvage treatment in the patients receiving SRS only based on two RCTs. The odds ratio (OR) was 4.91 (95% CI: 2.74, 8.80, p < 0.00001; Figure 8).

Meta-analysis of the overall tumor control rate shown as forest plot between SRS (stereotactic radiosurgery) alone and WBRT (whole brain radiotherapy) plus SRS. Hazard ratios with 95% CI are shown.

Meta-analysis of the salvage therapy is shown as forest plot between SRS (stereotactic radiosurgery) alone and WBRT (whole brain radiotherapy) plus SRS. Hazard ratios with 95% CI are shown.
Neurological death
Only two RCTs provided the data comparing neurologic death outcome, one for each comparison. Hence meta-analysis of this outcome was not done.
WBRT versus WBRT plus SRS
The RCT reported no significant difference between treatments in neurological cause of death. The OR was 1.12 (0.67–2.0) (95% CI: 0.67–1.87, p = 0.66).
SRS versus WBRT plus SRS
No significant difference was reported between the treatments at 12-month follow-up. The OR was 0.81 (95% CI: 0.34–1.96, p = 0.64).
Adverse events
Four RCTs reported adverse events for the treatment difference. Adverse events consisted of acute and late toxicities. Acute toxicities are identified as the events that arose within 90 days of the start of radiotherapy and late toxicities as events that occurred thereafter according to Radiation Therapy Oncology Group (RTOG) central nervous system (CNS) toxicity criteria. Meta-analysis of adverse events was performed on the basis of data provided by four RCTs.
WBRT versus WBRT plus SRS
Meta-analysis of adverse events (⩾Grade 2) showed no significant difference in the treatments with an overall OR of 1.16 (95% CI: 0.77–1.76, p = 0.48). Meta-analysis of acute and late toxicities (⩾Grade 2) revealed no significant difference between the treatments based on two RCTs. The OR for acute and late toxicities were 1.36 (95% CI: 0.83–2.24, p = 0.23) and 0.80 (95% CI: 0.37–1.73, p = 0.57), respectively (Figure 9).

Meta-analysis of the adverse events shown as forest plot between WBRT (whole brain radiotherapy) alone and WBRT plus SRS (stereotactic radiosurgery). Odds ratios with 95% CI are shown.
SRS versus WBRT plus SRS
Meta-analysis of acute and late toxicities (⩾Grade 2) revealed no difference in treatments. The OR for acute and late toxicities were 1.53 (95% CI: 0.55–4.25, p = 0.41) and 0.48 (95% CI: 0.16–1.49, p = 0.20), respectively. Comparison for overall adverse events (⩾Grade 2) reported was carried out, and no difference was obtained based on three RCTs with a combined OR 0.92 (95% CI: 0.59–1.42, p = 71; Figure 10).

Meta-analysis of the adverse events shown as forest plot between SRS (stereotactic radiosurgery) alone and WBRT (whole brain radiotherapy) plus SRS. Odds ratios with 95% CI are shown.
Discussion
WBRT has been a standard treatment for brain metastases for several decades. In recent years, addition of SRS (focal aggressive therapy) to WBRT has been recognized. Benefits of the combined approach are mostly restricted to a better local control rate but no survival benefit has been reported.5,6,8,16–18 Contrasting results have been obtained previously on the benefit of omitting upfront WBRT and treating patients with SRS alone.
This meta-analysis is the first meta-analysis to compare WBRT alone and SRS alone or in combination for treating brain metastases based only on RCTs. One previous meta-analysis 21 has compared these treatment modalities in treating brain metastases. However, of the three RCTs included in the study, two compared WBRT alone versus WBRT plus SRS and in one study the sample was only 27 patients. The third RCT was only published as an abstract comparing these three approaches. Furthermore, their comparison of SRS alone versus WBRT plus SRS was mostly based on prospective study included in the study and not on RCT. Hence this study was done to draw clearer conclusions on all the three treatment approaches.
The results of this meta-analysis revealed that all the three therapeutic approaches were similar for survival outcome. However, WBRT plus SRS was favorable for single brain metastasis for significantly better survival based on one RCT result compared to WBRT only. 5 Other RCTs did not provide any data regarding comparison of single versus multiple brain metastases for treatment difference.6,8,16,17 Overall, single brain metastases showed better survival regardless of the treatment modality. Similarly, in his prospective cohort study restricted to patients with single brain metastasis, Li et al. 22 reported highly significant (p < 0.0001) median survival benefit for WBRT plus SRS study arm in comparison to WBRT alone but there was no significant difference between SRS alone and WBRT plus SRS for survival advantage (9.3 vs 10.6 months).
This meta-analysis reported no survival advantage for WBRT plus SRS in comparison to WBRT alone or SRS alone for multiple brain metastases. Similar results were reported in the RCT done by Chougule et al., 18 where all the three approaches were compared and showed a slight difference in median survival but were not significant statistically. In contrast, survival benefit for multiple brain metastases in WBRT plus SRS group in comparison to WBRT alone was reported in two retrospective cohort studies by Shanghavi et al. 23 and Wang et al. 24 (91 vs 37 weeks). Shanghavi et al. retrospective cohort trial was based on recursive partitoning analysis (RPA) and showed a median survival of 16.1, 10.3, and 8.7 months for RPA classes I, II, and III, respectively, suggesting survival benefit for WBRT plus SRS boost. Another aspect of these retrospective cohort studies was that they also found survival benefit for patients with low KPS scores (KPS < 70) irrespective of the number of brain metastases while the results of this meta-analysis are validated for patients with KPS 70-100.
Adding SRS to WBRT did not improve survival in patients with multiple brain metastases in comparison to SRS alone. This result has been reported in a number of retrospective cohort studies in which SRS was compared to WBRT plus SRS in patients with single or multiple brain metastases.25–30 Li et al. 22 also reported no significant median survival benefit for patients with single brain metastasis. Hall et al., 31 in his retrospective study, reported no significant differences in overall survival among patients treated with SRS alone, SRS + WBRT, or Surgery + SRS (S + SRS) with respective median survival of 9.8, 7.4, and 10.6 months. Combs et al. 32 reported significant better survival for SRS group, but in his study, only patients with brain metastases from breast cancer were included. Schüttrumpf et al. 33 reported a significant survival benefit for patients who had received a WBRT (SRS + WBRT: 341 days/SRS alone: 231 days, p = 0.049) in the univariate analysis of survival data. Similarly Wang et al.s’ 24 four-arm study also reported better survival (91 vs 67weeks) for patients receiving SRS boost.
Meta-analysis of local tumor control revealed significantly better local control for WBRT plus SRS boost in comparison to both WBRT alone and SRS alone. SRS alone presents with a high incidence of distant as well as local recurrence rates. Li et al.s’ 22 prospective cohort study reported statistically significant local control (p < 0.004) and median time to progression for treated tumor (p < 0.00001) for patients with single brain metastasis receiving SRS boost in comparison to WBRT alone. Chougule et al. 18 reported a local control of 87%, 91%, and 62% for patients treated with Gamma Knife (GK), GK + WBRT, and WBRT alone, respectively, suggesting comparatively low local tumor control for patients undertaking WBRT only. Wang et al. 24 reported no difference in local tumor control rate at 1 month (95.6% vs 88.3%). However 1-month duration is far too short time to assess the difference in local control. ASTRO’s evidence–based guidelines reported improved overall brain control when SRS boost was added to WBRT in patients with multiple metastases.
SRS only treatment approach results in significantly high incidence of local and distant failure. Chang et al. 34 reported that 73% of patients in the SRS plus WBRT group were free from CNS recurrence at 1 year, compared with 27% of patients who received SRS alone (p = 0.0003). Similarly, significant increase in local recurrence and reduced time to local recurrence were reported in one retrospective cohort study 30 in patients surviving more than 1 year. However, this significance was not observed in the distant recurrence analysis. Some of the studies have reported no significant difference in local tumor control for the treatment difference.22,25,26,28 Two of the RCTs reported significant difference in distant recurrence in patients receiving only SRS.8,16 This significant difference in distant brain recurrence was also reported in some of the retrospective cohort studies.25,29,35 However, there are some retrospective cohort studies26,28,30,32 comparing the two modalities reported no significance difference in distant recurrence rate.
High rate of local and distant brain recurrences associated with SRS only also results in high need for salvage treatment intervention and so has been reported in the two RCTs8,16 included in this study. Hall et al.’s retrospective study also reported that salvage therapy was required in 43% of SRS-alone and 26% of SRS + WBRT patients (p < 0.009).
Prognostic factors associated with better survival and local control are RPA class 1, number of brain metastasis, extent of intracranial lesion, no of brain sites involved, primary disease status (controlled/active), primary histology in some studies, and treatment modality.5,6,8,16–18 Secondary analysis of RTOG 9508 5 using a newly developed prognostic index “graded prognostic assessment” (GPA), revealed a better survival for patients with high GPA score (3.5–4.0) receiving WBRT + SRS versus WBRT alone (21 vs 10.3 months). 36 A diagnosis-specific GPA (DS-GPA) secondary analysis of JROSG99-1 8 restricted to patients with only non–small cell lung cancer (NSCLC), revealed significantly better survival in DS-GPA 2.5-4.0 group in patients receiving WBRT + SRS versus SRS alone. 37 This survival advantage could be explained by better local control achieved with combined approach in DS-GPA 2.5–4.0 (HR: 8.31; 95% CI: 3.05–29.13, p < .001) as compared to DS-GPA 0.5–2.0 (HR: 3.57, 95% CI: 1.02–16.49, p = .04).
It has been suggested that avoidance of WBRT has a positive impact on cognitive function and health-related QOL (class I evidence). 34 In this review, only one RCT 5 provided the data comparing WBRT alone with WBRT plus SRS at 6-month follow-up and reported no difference in neurocognition function between treatments. Neurocognitive function was evaluated based on MMSE. Using similar approach, Aoyama et al. reported no difference between SRS alone and WBRT plus SRS at 12-month follow-up. Analyzing the data on neurocognitive function from same trial, Aoyama et al. 38 reported the average duration until deterioration was 16.5 months in the WBRT + SRS group and 7.6 months in the SRS-alone group (p = 0.05). Contrasting results were obtained in the RCT done by Brown et al. using a comprehensive range of tests to evaluate different aspects of neurocognitive function and found statistically significant progression in WBRT plus SRS group than with SRS alone at 3-month follow-up. Similarly, in their study, 34 Chang et al. reported that patients treated with SRS plus WBRT were at a greater risk of a significant decline in learning and memory function by 4 months compared with the group that received SRS alone. Both these RCTs8,34 reported a better cognitive function in patients receiving SRS only at 3 and 4 months might be too early and so the results might reflect only temporarily and reversible decrease in cognitive function and QOL.
WBRT has been implicated for causing negative impact on health-related QOL. 39 It is argued that better intracranial tumor control could result in better QOL parameters. 40 In this study, one RCT 5 comparing WBRT versus WBRT plus SRS found statistically significant improvement in clinical performance and decreased steroid use in patients receiving SRS boost as compared to WBRT only. Another RCT 16 reported QOL data comparing SRS alone with combined approach. In this RCT, a greater clinically significant decline in QOL from baseline was documented in patients receiving SRS plus WBRT compared with SRS alone in terms of physical well being at 3-month follow-up in a group of 30 long-term survivors.
Whole brain radiation has been associated with high rate of toxicity particularly late toxicities. The results of this meta-analysis revealed a fair amount of evidence to justify that the overall toxicity (acute and late toxicities) remains the same whether or not the WBRT is used in combination with SRS or alone. Similarly in comparison to SRS only, the combined approach did not show any significant difference in causing the adverse events. No previous study has been done to specifically compare the treatments for its adverse events.
Despite the fact that this review and meta-analysis was based on RCTs and baseline characteristics of the included population were well matched; however, there are some limitations regarding the quality of these studies. None of the studies included were double blinded or even single blinded. One of the RCTs 5 is previously criticized for excessive bilateral crossover confounding the intent-to-treat survival analysis for patients with 2–3 tumors and inclusion of tumor masses >3 cm diameter which are not favorable for SRS. Kondziolka et al.’s 6 RCT was stopped at 60% accrual and hence its statistical power to assess differences in median survival was limited. The application of two RCTs results for survival analysis comparing WBRT versus WBRT plus SRS might be limited to some extent. Moreover, few patients were included in two of the RCTs.6,17
Previously, it has been thought that improving local tumor control would yield in better survival outcome for patients with brain metastases. Adding SRS to WBRT improves local tumor control and functional independence; however, this improvement in local control has not yielded a survival benefit. Though secondary analysis for graded prognostics assessment showed better survival in patients with high GPA score receiving WBRT + SRS as compared to WBRT only as well as SRS only. As well as omitting WBRT would require a much high rate of salvage treatment induction and since adverse events mostly remain the same, it can be concluded that adding SRS to WBRT as initial treatment is a much better choice of treatment for brain metastases. Better QOL and cognitive function is reported earlier with SRS only and so patients with worst prognosis could be recommended to receive SRS only.
Conclusion
There was no significant survival difference between the treatments in patients with multiple brain metastases. WBRT plus SRS improves survival in patients with single brain metastasis. WBRT plus SRS results in significantly better local tumor control as compared to WBRT only. SRS only results in significantly high local tumor control failure and distant brain recurrences as compared to combined approach. Stereotactic radiosurgery only results in better QOL in short term while cognitive function is preserved in long term. Therefore SRS only could be recommended in patients with low prognostic factors as better cognitive function and QOL of life is achieved earlier on following treatment. No difference was observed for adverse effects and neurologic death between the treatments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of China (Grants: 81272508, 81302326, and 81572964) and Natural Science Foundation of Guangdong (Grant: 2014A030313289).