
Abstract
Mortalin is a member of the heat shock protein 70 family, which is involved in multiple cellular processes and may play key roles in promoting carcinogenesis. This study attempted to identify the clinical consequences of Mortalin overexpression and its roles in the prognostic evaluation of non–small cell lung cancer. A total of 120 non–small cell lung cancer samples paired with the adjacent non-tumor tissue samples and 10 normal lung tissues were selected for immunohistochemical staining for Mortalin. The localization of Mortalin was detected in A549 non–small cell lung cancer cells using immunofluorescence staining. The correlations between Mortalin overexpression and the clinical features of non–small cell lung cancers were evaluated using the chi-square test. The survival analysis was calculated via the Kaplan–Meier method and the Cox proportional hazard models. Our studies suggested that Mortalin exhibited a primarily cytoplasmic staining pattern in the non–small cell lung cancers. The rate of strongly positive Mortalin expression was higher in the non–small cell lung cancer samples than in the adjacent non-tumor samples or in normal lung tissues. Mortalin overexpression was significantly correlated with high histological grades, advanced stages, lymph node metastases, and lower disease-free survival and overall survival rates of the patients with non–small cell lung cancer. The survival analysis demonstrated that Mortalin overexpression was a significant independent prognostic factor in non–small cell lung cancer, especially for patients with early stage of non–small cell lung cancer. In conclusion, Mortalin is up-regulated in non–small cell lung cancer, and it may be a potential biomarker of prognostic evaluation and a molecular therapeutic target for patients with early stage of non–small cell lung cancer.
Introduction
Lung cancer is one of the most prevalent malignancies and the leading cause of cancer-related death globally. According to a report by Torre et al. 1 in 2015, the incidence and mortality rates of lung cancer remain elevated. Non–small cell lung cancer (NSCLC), the most common type of lung cancer, accounts for about 80% of all lung cancer. Despite the tremendous improvement in diagnoses and treatments, a large number of patients with NSCLC are diagnosed in the advanced stages, and the prognoses of these patients have remained poor over the past decades. 2 Currently, the key obstacle to progress is the lack of accurate and specific targets for the early diagnosis in NSCLC. In this context, biomarker-based assays and molecular results will offer added values.
Mortalin (also termed GRP75/mtHSP70/PBP74) is a member of the heat shock protein 70 (HSP 70) family, which is encoded by the nuclear gene HSPA9B (GeneID: 3313), which is localized on chromosome 5q31.1.1. 3 Mortalin has been identified as a mitochondrial-resident protein and has a molecular weight of 74 kDa. As an essential protein that participates in proliferation, functional maintenance, and stress response of cells, Mortalin has been implicated in human carcinogenesis because it enhances cancer cell proliferation, protects cancer cells against apoptosis, and promotes cancer angiogenesis.4,5 Simultaneously, Mortalin may also inactivate tumor suppressor protein p53 and modulate the Ras–Raf–MAPK (mitogen-activated protein kinase) signaling pathway.6,7 The up-regulation of Mortalin has been detected in numerous human malignancies, including brain tumor, hepatocellular carcinoma (HCC), colon carcinoma, and leukemia. 4 In addition, our previous study demonstrated that the level of Mortalin expression is significantly up-regulated in breast cancer tissues compared with adjacent non-tumor tissues, which suggests that Mortalin could be a prognostic or predictive biomarker of invasive ductal carcinoma of breast. 8 However, to date, there is little information regarding the relationship between Mortalin and NSCLCs.
In this study, we present immunohistochemical (IHC) staining for the Mortalin protein in 120 NSCLC samples, paired with the adjacent non-tumor tissues and 10 normal lung tissue samples. Our data revealed that Mortalin was frequently up-regulated in the NSCLC samples compared with the adjacent non-tumor tissues, which suggests that Mortalin may be an independent biomarker for the prognostic evaluation of patients with NSCLC.
Materials and methods
Clinical samples
A total of 130 tissue samples were used in this study, including samples from 120 cases of NSCLC with paired adjacent non-tumor tissues and 10 samples from normal lung tissues (from autopsy cases). These tissues were collected from Tumor Tissue Bank of Yanbian University Medical College between July 2004 and September 2007. All tissues were routinely fixed in 10% buffered formalin and embedded in paraffin blocks. The study protocol was approved by the institutional review board of Yanbian University Medical College. The pathological parameters, including gender, age, smoking status, tumor size, histological grade, histological type, clinical stage, nodal metastasis, and survival data (75 cases), were carefully reviewed in all 120 of the NSCLC cases. The patients’ ages ranged from 20 to 84 years, and 66 cases were <60 years, and 54 cases were ≥60 years. The male to female ratio was 69:51. Of the 120 NSCLC cases, 101 included tumors sizes T1–T2 and 19 cases had tumors sizes T3–T4. Regarding the histological grades of the NSCLCs, 16 cases were Grade 1, 68 cases were Grade 2, and 36 cases were Grade 3. Regarding the histological types of the NSCLCs, 52 cases were lung adenocarcinomas, and 68 cases were lung squamous cell carcinomas. Regarding the stagings of the NSCLCs, 85 cases were in tumor, node, metastasis (TNM) stages I–II, and 35 cases were in TNM stages III–IV. The TNM stagings were assessed according to the staging system established by the American Joint Committee on Cancer (AJCC). 9 In addition, 53 cases had lymph node (LN) metastasis, and 67 cases had no LN metastasis.
A total of 120 patients with NSCLCs underwent surgical treatments but were without adjuvant chemotherapy at the time of data collection. The survival information for 75 patients was successfully collected over 8 years or until death.
Immunofluorescence staining analysis
The A549 NSCLC cell line was grown on coverslips to 70%–80% confluence, and then all of the cells were fixed with 4% paraformaldehyde for 10 min and permeabilized with 0.5% Triton X-100 for 10 min at room temperature. Subsequently, after blocking with 3% bovine albumin fraction V (A8020; Solarbio, Beijing, China) for 1 h and washing with phosphate-buffered saline (PBS), the cells were incubated with rabbit anti-Mortalin antibody (ab53098; Abcam, Cambridge, MA, USA), at 4°C overnight and then incubated with Alexa Fluor® 488 Goat Anti-Rabbit IgG (H+C) (A11008, 1:1000; Invitrogen, CA, USA) for 1 h. Next, the cells were washed with PBS and counterstained with 4,6-diamidino-2-phenylindole (DAPI; C1006, Beyotime, Shanghai, China). The coverslips were mounted with Antifade Mounting Medium (P0126, Beyotime, Shanghai, China). Finally, the immunofluorescence (IF) signals were visualized and recorded using a BX53 Olympus microscope.
IHC staining analysis
IHC staining was performed using the DAKO LSAB kit (DAKO A/S, Glostrup, Denmark). Briefly, serial 4-µm-thick tissue sections were prepared on silane-coated slides (Sigma, St. Louis, MO, USA) and deparaffinized, rehydrated, and incubated with 3% H2O2 in methanol for 15 min at room temperature. Subsequently, the antigen was retrieved in 0.01 M sodium citrate buffer (pH 6.0). The slides were incubated with rabbit anti-Mortalin antibody (ab53098; Abcam, Cambridge, MA, USA) at 4 °C overnight. After incubation with biotinylated secondary antibody at room temperature for 30 min, the slides were covered with streptavidin–peroxidase complex. IHC staining was developed using 3,3′-diaminobenzidine and counterstaining with Mayer’s hematoxylin. We used liver sections as positive controls and rabbit IgG as an isotype control. Furthermore, the positive tissue sections were processed without primary antibody as a negative control.
Analysis of IHC results
All slides were examined independently by two pathologists (L.-Y.C. and Z.-H.L.) who were blinded to the clinical data. In cases of discrepancies, a final score was established by reassessment on a double-headed microscope. The interpretation criteria were the same as those previously described. 10 Briefly, the IHC staining for Mortalin was semi-quantitatively scored as “−” (negative, none, or less than 5% positive cells), “+” (5%–50% positive cells), and “++” (more than 50% positive cells, considered as strongly positive). For the double scoring system together, “++” scored samples were considered to exhibit Mortalin overexpression, and “−” and “+”scored samples were considered to exhibit Mortalin low expression.
Statistical analysis
The statistical analyses were conducted using the SPSS 17.0 software (SPSS, Chicago, IL, USA) for Windows. The correlations between Mortalin protein expression and the clinicopathological features were evaluated with chi-square tests (χ2) and Fisher’s exact tests. The survival curves were examined using the Kaplan–Meier method, and significant differences were identified with log-rank tests. Multivariate survival analyses were performed on all significant characteristics as measured by the univariate survival analyses using the Cox proportional hazard regression model. Values of p < 0.05 were considered statistically significant.
Results
Mortalin protein expression in the NSCLCs
IF staining indicated that the Mortalin protein exhibited a strictly cytoplasmic staining pattern in the A549 NSCLC cells (Figure 1). IHC staining consistently demonstrated that the Mortalin protein was primarily located in the cytoplasm of the NSCLCs (Figure 2). The Mortalin protein positive rate was 90.0% (108/120) in the NSCLCs, which was significantly higher than that in the adjacent non-tumor samples (3.3%, 4/120) and that in the normal lung tissues (0.0%, 0/10; p < 0.01). Similarly, the rate of strongly positive Mortalin expression was also higher in the NSCLCs (49.2%, 59/120) than in the adjacent non-tumor samples (0.0%, 0/120; p < 0.01; Table 1).

IF staining for the Mortalin protein in the A549 NSCLC cells. The Mortalin protein was primarily located in the cytoplasm of the A549 cells (green indicates Mortalin staining and blue indicates DAPI).
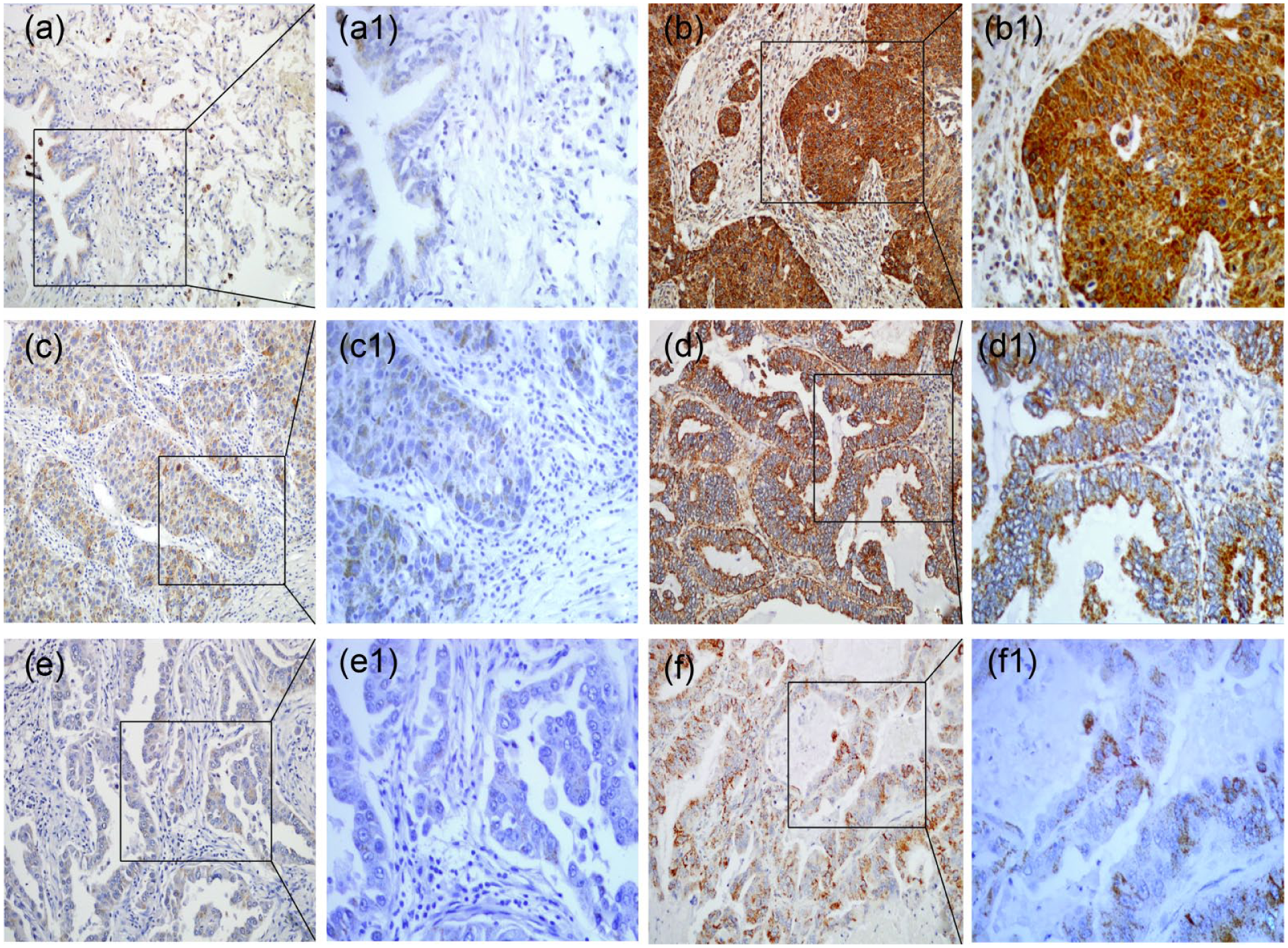
IHC staining for Mortalin protein expression in the lung tissues. (a) The normal lung tissues were negative for Mortalin protein. (b) The Mortalin protein exhibited diffuse and strongly positive staining in the lung squamous cell carcinomas (SCCs) and was principally localized in the cytoplasm of the cells. (c) The lung SCCs were weakly positive for Mortalin. (d) Diffuse and strongly positive Mortalin protein signals were observed in lung adenocarcinoma. (e and f) Mortalin protein staining was negative or weakly positive in the lung adenocarcinomas. (a1)–(f1) indicate higher magnification of the selected area in (a)–(f), respectively (original magnification, a–f: ×200; a1–f1: ×400).
Mortalin protein expression in NSCLC.
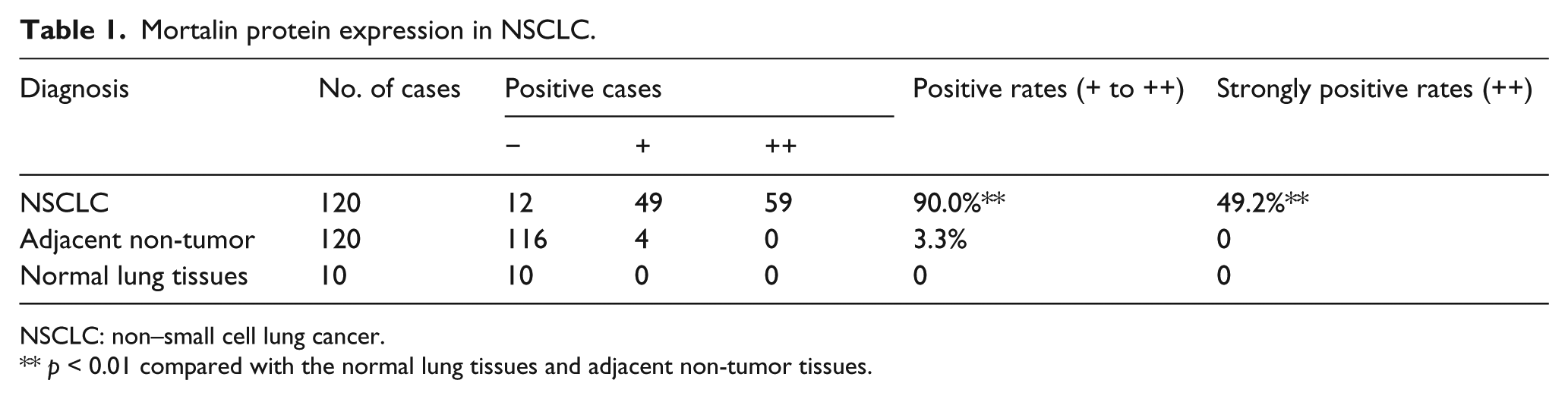
NSCLC: non–small cell lung cancer.
p < 0.01 compared with the normal lung tissues and adjacent non-tumor tissues.
Correlations between Mortalin protein overexpression and the clinical parameters of the NSCLCs
To evaluate the role of Mortalin in NSCLC progression, we analyzed the correlation between Mortalin overexpression and the clinicopathological features of the NSCLC patients. Generally, Mortalin protein overexpression was significantly correlated with the histological grade, clinical stage, and LN metastasis of the NSCLCs but was not related to gender, age, smoking status, histological type, or tumor size (p > 0.05). The rate of strongly positive Mortalin expression was significantly higher in the Grade 3 NSCLCs (72.2%, 26/36) than in the Grade 2 (41.2%, 28/68) and Grade 1 NSCLCs (31.3%, 5/16; p = 0.003). Regarding the clinical stage, the rate of strongly positive Mortalin protein expression was 77.1% (27/35) in the NSCLCs in advanced stages (III–IV), but this rate was only 37.6% (32/85) in the early stage (I–II) cases (p = 0.000). Moreover, the rate of strongly positive Mortalin expression was also higher in the NSCLC patients with LN metastases (64.2%, 34/53) than in those without metastases (37.3%, 25/67; p = 0.003; Table 2 and Figure 3).
Correlations between Mortalin protein expression and the clinicopathological features of the NSCLCs.

NSCLCs: non–small cell lung cancer; TNM = tumor, node, metastasis; LN: lymph node.
p < 0.01.
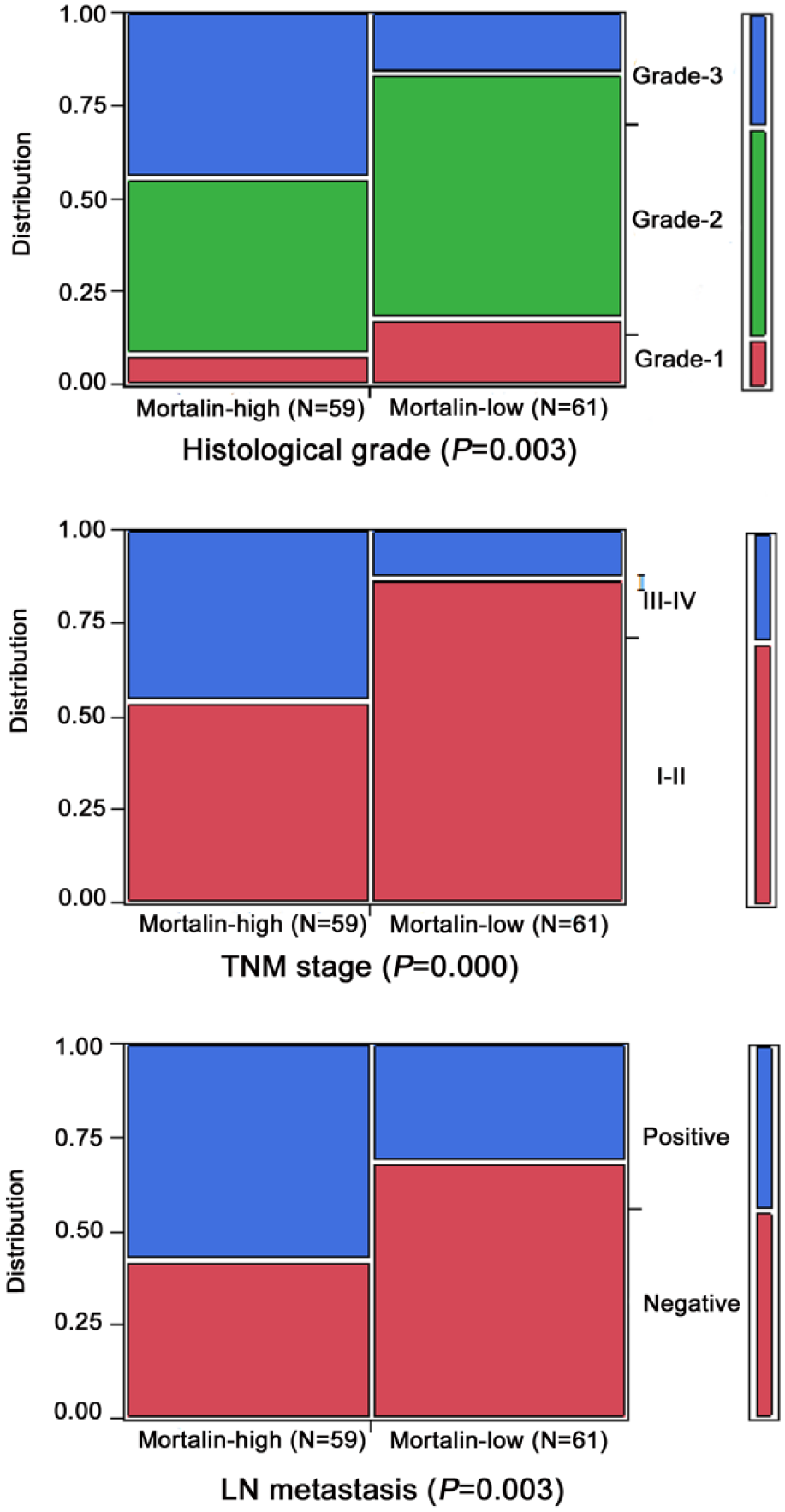
Association between Mortalin expression and clinicopathological parameters of NSCLC. Mortalin overexpression rates in high-grade, late-stage, and lymph node metastasis NSCLCs are significantly higher than in the contrasting groups.
Correlations between Mortalin overexpression and the prognosis of the patients with NSCLCs
To evaluate the role of Mortalin overexpression in NSCLC progression, we analyzed the prognostic factors and the overall survival (OS) of 75 NSCLC cases using the Cox proportional hazards model. Univariate analyses revealed that tumor size (p = 0.039), TNM stage (p = 0.000), LN metastasis (p = 0.007), and the level of Mortalin expression (p = 0.002) were associated with OS in the patients with NSCLC (Table 3), which indicated that Mortalin overexpression might be a valuable prognostic factor in NSCLC. Further multivariate analysis demonstrated that Mortalin overexpression was also emerged as a significant independent prognostic factor for the prognoses of the NSCLCs (hazard ratio (HR): 2.337, 95% confidence interval (CI): 1.114–4.905, p = 0.025). Similarly, TNM stage was a prognostic factor (HR: 3.186, 95% CI: 1.500–6.768, p = 0.003). To further substantiate the importance of Mortalin overexpression in NSCLC progression, we analyzed the association between Mortalin expression and the disease-free survival (DFS) and OS rates of 75 NSCLC cases using the Kaplan–Meier method. The DFS and OS rate was significantly greater in the NSCLC cases with Mortalin low expression than in the cases with Mortalin overexpression (Figure 4). In addition, for the patients with early-stage (I–II) NSCLCs, the survival analysis revealed that the Mortalin level was associated with a lower DFS and OS rate (log-rank = 5.157 and 5.905, respectively; p = 0.023 and 0.015, respectively) (Figure 5(a) and (c)). However, Mortalin protein overexpression did not correlate with the DFS and OS rate among patients with late-stage (III–IV) NSCLCs (log-rank = 0.610 and 0.426, respectively; p = 0.435 and 0.514, respectively) (Figure 5(b) and (d)); this result might be attributable to the small sample size of this experiment.
Univariate and multivariate survival analyses of the clinicopathological features of 75 NSCLCs.

NSCLCs: non–small cell lung cancer; SE: standard error; HR: hazard ratio; CI: confidence interval; TNM = tumor, node, metastasis; LN: lymph node.
The statistical analysis was performed using the Cox proportional hazard regression model.
p < 0.05; **p < 0.01.

Kaplan–Meier survival curves of 75 NSCLC patients according to Mortalin protein expression. The NSCLC patients who exhibited Mortalin overexpression also exhibited a lower (a) DFS and (b) OS rate than those with low expression of Mortalin (p = 0.002 and 0.001, respectively).

Kaplan–Meier survival curves of 75 patients with and without Mortalin-expressing NSCLCs in relation to TNM stage. (a and c) Comparison of the DFS and OS rates of the patients with Mortalin overexpression and the early-stage patients with low expressions of Mortalin. (b and d) Comparison of DFS and OS rates of the Mortalin overexpressing patients and the late-stage, low-expression patients.
Discussion
Mortalin is a highly conserved molecular chaperone in the HSP 70 family. 11 Mortalin is involved in multiple cellular processes and may play key roles in promoting carcinogenesis. Several observations have demonstrated that the levels of Mortalin are elevated in many human tumor cells and immortalized cell lines. 4 Moreover, Mortalin may exhibit differential subcellular location, that is, it localizes to the mitochondria in normal cells and to the cytosol in cancerous cells. 6 Furthermore, Mortalin acts in various functions that are related to the proliferation of cancer cells, including mitochondrial biogenesis, adenosine triphosphate (ATP) production, anti-apoptosis, and chaperoning.12–14 In contrast, the knockdown of Mortalin via RNA interference or the utilization of MKT-077 (a cationic inhibitor of Mortalin) causes the arrest of the growth/apoptosis of cancer cells and senescence-like growth arrest in immortalized cells.4,15–19
Yi et al. 20 demonstrated that Mortalin overexpression is associated with positive venous infiltration and advanced tumor TNM stages in HCCs using a proteomics analysis of matched tumor and non-tumor tissues, which suggests that Mortalin might be a biomarker for the detection of HCCs metastasis and recurrence. Ando et al. 21 revealed that Mortalin expression is significantly higher in gastric cancer tissues than in normal gastric tissues and is closely correlated with the depth of invasion, LN and liver metastasis in patients with gastric cancer. In this study, we performed IHC staining for Mortalin in 120 NSCLC samples, paired with adjacent non-tumor tissues and 10 normal lung tissues, and found that the positive and strongly positive rates of Mortalin protein expression were significantly higher in the NSCLC tissues than in either the adjacent non-tumor tissues or the normal lung tissues. These results indicated that Mortalin plays an important role in the progression of NSCLC and support the premise that Mortalin overexpression is related to the promotion of human carcinogenesis. Moreover, we found that the Mortalin protein exhibited a primarily cytoplasmic staining pattern based on the IF staining of the A549 cells and the IHC analysis of paraffin-embedded NSCLC tissues, and these findings are consistent with those of Shin et al.’s 22 study. Jin et al. 8 demonstrated that Mortalin overexpression is associated with a high histological grade, advanced tumor TNM stages, and LN metastasis in breast cancer. Similarly, we found that the level of Mortalin expression was significantly correlated with the histological grade (p = 0.003), the TNM stage (p = 0.000), and LN metastasis (p = 0.003) but was not related to gender, age, smoking status, histological type, or tumor size in the patients with NSCLC (p > 0.05). Unfortunately, poor differentiation, advanced TNM stage, and LN metastasis are indicative of poor outcomes and recurrence in patients with NSCLCs. Therefore, Mortalin may play an important role in the progression and aggressiveness of NSCLCs.
Regarding survival, we previously found that Mortalin protein overexpression is strongly associated with shortened DFS and OS among patients with invasive ductal carcinoma of the breast. 8 Dundas et al. 23 also reported a significant association between Mortalin overexpression and poor patient survival of colorectal adenocarcinoma patient survival. In this study, we found that NSCLC patients with Mortalin protein overexpression exhibited a lower DFS and OS rate than those with Mortalin protein low expression. In addition, the univariate survival analyses revealed that tumor size, TNM stage, and LN metastasis were all associated with the OS rates of the patients with NSCLC. Multivariate survival analysis revealed that Mortalin overexpression and TNM stage were independent prognostic factors. Furthermore, Mortalin overexpression was strongly correlated with the DFS and OS rate of the early-stage patients with NSCLC; the DFS and OS rates were significantly higher in Mortalin low-expressing patients than in the Mortalin overexpressing patients. These findings indicated that Mortalin might be a potential biomarker for prognostic evaluation and a molecular therapeutic target in patients with early stage of NSCLC.
Recently, Starenki et al. 24 demonstrated that Mortalin can regulate the MEK/ERK pathway and mitochondrial bioenergetics to promote the proliferation of medullary thyroid carcinoma cells. As a common hallmark of tumorigenesis, MEK/ERK pathway can trigger innate tumor-suppressive mechanisms. The researchers proved that Mortalin was a negative regulator of MEK/ERK pathway and might perform a biological target for the reactivation of tumor-suppressive pathway in medullary thyroid carcinoma. Chen et al. 25 found that Mortalin overexpression is correlated with the metastatic phenotype of HCC cells and promotes the epithelial to mesenchymal transition. Despite these data, the molecular mechanism by which Mortalin is responsible for NSCLC progression remains to be elucidated. Thus, further studies with larger sample sizes and molecular biology experiments are required to confirm the role of Mortalin in NSCLC tumorigenesis.
Footnotes
Ethical approval
This research was conducted in accordance with the Helsinki Declaration and was approved by the Human Ethics Committee and the Research Ethics Committee of Yanbian University Medical College. The patients were informed that the resected specimens would be kept by the hospital and potentially used for scientific research, and that their privacy would be maintained. Follow-up survival data were retrospectively collected through medical-record analyses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Special Research Project of the “973 Plan” (2014CB560708), the National Natural Science Funds of China (No. 61371067) and the International Cooperation Project of the Science & Technology Department of Jilin Province (No. 20150414030GH).