
Abstract
The carcinogenesis of non–small cell lung carcinoma has been found to associate with activating and resistant mutations in the tyrosine kinase domain of specific oncogenes. Here, we assessed the type, frequency, and abundance of epithelial growth factor receptor, KRAS, BRAF, and ALK mutations in 154 non–small cell lung carcinoma specimens using single-molecule amplification and re-sequencing technology. We found that epithelial growth factor receptor mutations were the most prevalent (44.2%), followed by KRAS (18.8%), ALK (7.8%), and BRAF (5.8%) mutations. The type and abundance of the mutations in tumor specimens appeared to be heterogeneous. Thus, we conclude that identification of clinically significant oncogenic mutations may improve the classification of patients and provide valuable information for determination of the therapeutic strategies.
Keywords
Introduction
Being one of the most common cancer types worldwide and accounting for a significant number of cancer-associated fatalities, lung cancer is a major threat for public health.1–3 Lung cancer is often diagnosed at an advanced stage when it displays a poor prognosis, largely resulting from the fast-growing nature of the cancer cells and their early metastases. 4 Non–small cell lung carcinoma (NSCLC) is a lung cancer of three subtypes based on pathology: squamous cell carcinoma, large cell carcinoma, and adenocarcinoma. Recently, our knowledge on the molecular mechanisms and biology of lung cancer has been improved, with the introduction of new therapeutic agents and approaches into lung cancer treatment.5–11 However, the overall 5-year survival rate is still below 4%. 12 Hence, further elucidation of molecular regulation of lung cancer growth appears to be critical for improving therapeutic outcome and the overall 5-year survival rate of the patients.
Genetic profiling of NSCLC specimens has detected some genetic variants in certain oncogenes.13–15 Among the common mutations associated with NSCLC, the epithelial growth factor receptor (EGFR) gene is a pronounced one. The higher frequencies of EGFR mutation are commonly found in an Asian population of never smokers (up to 50%), whereas the lower frequencies of EGFR mutation are commonly found in a western population (down to 10%).16–18 anaplastic lymphoma kinase (ALF),19–21 Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS),22–24 and serine/threonine-protein kinase B-Raf (BRAF)25–27 mutations are also detected in a small portion of NSCLC patients.
Next-generation sequencing (NGS)-based diagnostic methods are becoming reliable and accurate assays for detecting oncogenic mutations in formalin-fixed biopsy samples.28,29 Given the diversity of clinically significant oncogenic mutations associated with NSCLC tumors, a more comprehensive methodology with the capacity to simultaneously detect and quantitate multiple oncogenic mutations is highly needed for evaluating the patient’s tumor mutation profile and for identifying the subgroups of patients with an anticipated satisfactory therapeutic outcome. 30
Here, we evaluate the performance of a recently developed single-molecule amplification and re-sequencing technology (SMART) for detecting and quantitating the hot spot EGFR, ALK, KRAS, and BRAF mutations in NSCLC tumor biopsies.
Materials and methods
Study approval
The research study (Figure 1) was approved by Human Ethics Committee of Fourth Hospital of Hebei Medical University. A total of 154 patients diagnosed with NSCLC at Fourth Hospital of Hebei Medical University participated in the study. The biopsied specimens were formalin-fixed and then evaluated for EGFR mutations using the gold standard amplification refractory mutation system-polymerase chain reaction (ARMS-PCR) assay. These specimens were then evaluated for the presence of oncogenic mutations in EGFR, KRAS, BRAF, and ALK by a multiplex SMART assay. The specific aim of the study was to determine the concordance between the two assays for detecting EGFR mutations, the overall frequency, and level of oncogenic mutations in the tumor specimens. For these studies, all patients provided signed, informed consent for their tissues to be used for scientific research.

Sensitivity of SMART assay for detection of common EGFR variants.
Before using SMART assay for analyzing gene mutations in NSCLC specimens, the reliability of the SMART assay to quantitate EGFR mutations was evaluated using artificial models with increasing mutation input levels of 0.01%, 0.05%, 0.1%, 0.5%, 1%, 5%, 10%, and 50%. By Pearson correlation, there was a linear relationship between actual (Y-axis) and theoretical Lg values (R2 = 0.99).
Pathology of NSCLC specimens
Tumor specimens removed by surgery were formalin-fixed and paraffin-embedded for histology. Histologic evaluation of NSCLC sections was performed independently by two experienced pathologists. The histological features of the specimens were evaluated by two experienced pathologists independently, according to the World Health Organization classification criteria.
Preparation of genomic DNA from formalin-fixed specimens
A total of 10 formalin-fixed and paraffin-embedded sections (6 mm thickness) from each NSCLC specimen were used to prepare genomic DNA for mutation profiling by ARMS-PCR and SMART assays. Isolation of genomic DNA was performed using the DNeasy Blood & Tissue Kit (Qiagen, Valencia, CA, USA), according to the manufacturer’s instruction.
EGFR mutation detection by ARMS-PCR assay
ARMS-PCR for detection of EGFR mutations was performed using the Human EGFR Mutation Analysis Kit for Real-Time PCR (EntroGen, Inc, Woodland Hills, CA, USA), according to the manufacturer’s instruction.
Detection of EGFR, KRAS, BRAF, and ALK mutation by SMART assay
Quantitation of the level of EGFR, KRAS, BRAF, and ALK mutations in tumor specimen genomic DNA was performed using a multiplex SMART assay. In brief, 50 ng of DNA was fragmented to an average size of 300 bp. DNA libraries were prepared. Single DNA molecules were circularized and targeted with back-to-back primers located within 20–48 nucleotides of the mutant loci of interest. Following amplification of the targeted alleles by inverse polymerase chain reaction (PCR), paired end sequencing was performed. A minimum of 1000 unique allelic molecules were counted, and mutation levels of >0.1% were defined as positive. The mutation ratio was calculated as the number of mutant alleles/total alleles.
Statistical methods
All statistical analyses were carried out using the SPSS 18.0 statistical software package. Comparison of expected and experimentally determined mutation levels was performed by Pearson’s correlation. The relationship of EGFR gene mutations with clinic data was assessed by the chi-square test. A p value of <0.05 was considered statistically significant.
Results
Patient information
The baseline clinical characteristics of the 154 study participants are summarized in Table 1. The median age of the patient cohort was 56.8 years, with majority (100, 64.9%) under the age of 65 years old. The ratio of male participates to female participates was 95:59. For smoking history, approximately half of the patients (79, 51.3%) reported either a current or previous history of smoking. The majority of patients (140, 90.9%) had histologic subtypes of adenocarcinoma, whereas other patients had squamous carcinoma (14, 9.1%). Based on clinical staging, there were 35 stage I (22.8 %), 35 stage II (22.8 %), 28 stage III (18.2%), and 56 stage IV (36.3%) patients. Thus, this study cohort was representative of a fairly typical group of patients with diverse pathologies and stages of NSCLC.
Patient demographics and clinical information of EGFR.

EGFR: epithelial growth factor receptor; SMART: single-molecule amplification and re-sequencing technology; NSCLC: non–small cell lung carcinoma.
Validation of SMART assay for quantitation of EGFR mutations
Before using SMART assay for analyzing gene mutations in NSCLC specimens, the reliability of the SMART assay to quantitate EGFR mutations was evaluated using artificial models with increasing mutation input levels of 0.01%, 0.05%, 0.1%, 0.5%, 1%, 5%, 10%, and 50%. To closely mimic a formalin-fixed and paraffin-embedded specimen which contains fragmented genomic DNA, test samples with the indicated mutation levels were prepared by precisely mixing the correct proportions of a long PCR fragment containing the mutation with normal genomic DNA. Thereafter, the DNA mixture was fragmented prior to SMART assay using the same protocol that was applied to fragmenting the formalin-fixed and paraffin-embedded samples, which demonstrated a linear relationship between observed and expected mutation levels, with R2 values reaching 0.99 (Figure 1), suggesting that the SMART assay was quantitative over the wide dynamic range of test mutation levels.
Concordance of SMART and ARMS-PCR assays for detecting EGFR mutation
Formalin-fixed 154 NSCLC specimens were then analyzed independently by an ARMS-PCR assay and by the validated SMART assay. Positive and negative concordance between ARMS-PCR and SMART methods for detection of these EGFR mutations was used to judge the performance of both assays (Table 2). Overall, there was a high degree of concordance between the two assays, particularly for the most frequently detected mutations L858R and exon 19 deletions (E19 del). In 52 EGFR mutation-positive samples by ARMS-PCR, SMART assay detected 50 positive samples but missed 2 with E19 del. In the remaining 102 samples that were negative for EGFR mutations by ARMS-PCR, 96 were also negative by SMART assay but 6 samples were positive. In summary, comparing with ARMS-PCR method which is currently the gold standard for EGFR mutation detection, the SMART assay had an overall detection sensitivity of 92.2% (50 out of 52 true positive samples) and 98.0% specificity (96 out of 98 true negative samples), which is pretty acceptable.
Concordance of SMART and ARMS-PCR assay for detection of EGFR mutations.
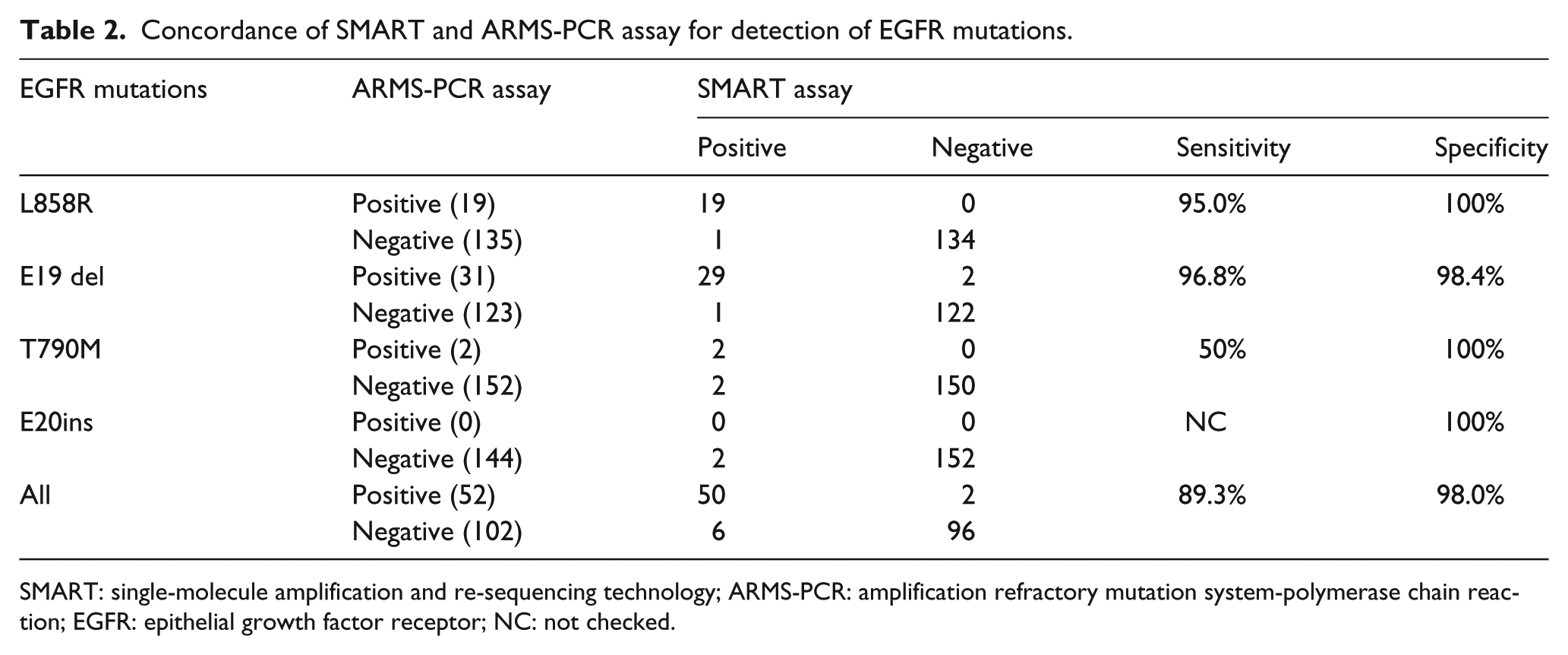
SMART: single-molecule amplification and re-sequencing technology; ARMS-PCR: amplification refractory mutation system-polymerase chain reaction; EGFR: epithelial growth factor receptor; NC: not checked.
Clinicopathological association of EGFR mutations
By correlation of EGFR mutation status with the clinicopathological characteristics of the 154 NSCLC patients, a significantly higher frequency of EGFR mutations were observed in females versus males (p < 0.05) and in non-smokers versus smokers (p < 0.05). There was no significant difference in the frequency of EGFR mutations in patients with adenocarcinoma or squamous carcinoma or in patients with stage I, II, III, or IV disease (Table 1).
Spectrum of EGFR, KRAS, BRAF, TP53, and ALK mutations
The SMART assay mutation data for the four other genes KRAS, BRAF, and ALK were then combined with the EGFR mutation data to give an overall perspective of the nature and frequency of mutations present in the 154 NSCLC specimens in relation to histologic type and stage of NSCLC (Figure 2). A total of 118 mutations were detected in the 154 samples. EGFR mutations (68, 44.2%) were the most frequent followed by mutations in KRAS (29, 18.8%), ALK (12, 7.8%), and BRAF (9, 5.8%; Figure 2). Moreover, the individual patient mutation profiles were very heterogeneous with respect to mutation type, frequency and abundance.

Spectrum of EGFR, KRAS, BRAF, TP53, and ALK mutations.
The SMART assay mutation data for the four other genes KRAS, BRAF, and ALK were then combined with the EGFR mutation data to give an overall perspective of the nature and frequency of mutations present in the 154 NSCLC specimens in relation to histologic type and stage of NSCLC. A total of 118 mutations were detected in the 154 samples. EGFR mutations (68, 44.2%) were the most frequent followed by mutations in KRAS (29, 18.8%), ALK (12, 7.8%), and BRAF (9, 5.8%).
Discussion
Here, mutations in the EGFR, KRAS, BRAF, TP53, and ALK genes using the validated single allelic molecule counting assay revealed highly heterogeneous tumor mutation profiles regardless of disease stage of NSCLC. The incidence and nature of the mutations detected in these four oncogenes were similar to that previously reported in other NSCLC patient cohorts.17,31,32 EGFR tyrosine-activating mutations L858R and the E19 del were the most prevalent mutations. Although many NSCLC biopsies had a single mutation event, some did contain more than one, consisting with previous studies.17,31,32 Moreover, there were oncogenic mutation(s) associated with histologic pathology type or stage of NSCLC. Thus, our findings support that random mutations are common in NSCLC.
In this study, we showed that the SMART assay was very accurate for measuring levels of common EGFR variants. Specifically, the SMART assay was highly sensitive and specific for detection of the EGFR mutations. Since “false negatives” E19 del were independently confirmed as a true negatives, re-adjustment of the concordance data for EGFR mutation detection may be applied in future study.
This study provides several advantages of the SMART assay for detecting patient-specific oncogenic mutations in NSCLC. First, the multiplex design allowed analyzing EGFR, KRAS, BRAF, and ALK mutations in a single assay. Therefore, it should be possible to design additional primers to target the relevant hot spot mutations in genes other than EGFR, KRAS, BRAF, and ALK mutations and develop an even more comprehensive SMART assay that covers all known oncogenic driver mutations associated with NSCLC. Second, the ability to quantitate the level of each mutation down to very low levels provides valuable clinical information about the penetrance of the mutation in each tissue specimen and what proportion of tumor cells could be potentially targeted by drug therapies. Third, with the emergence of promising reports showing the ability to detect oncogenic mutations in the circulating plasma DNA of NSCLC patients, the SMART assay may be emerging as a useful diagnostic tool for broad oncogenic mutation surveillance of plasma in response to chemotherapy.
Broad surveillance of mutations has confirmed a high degree of heterogeneity in the mutation status of NSCLC patients. We found that many tumor specimens had a single mutation. Interestingly, the single mutation was highly variable in tumor specimens from patients with stage I, II, III, or IV NSCLC, suggesting that either each mutation might occur independently. Further single cell genetic studies may help to identify the genetic constitution of tumor specimens with different spectrums and levels of oncogenic mutations. These observations revealed by SMART assay analysis of tumor specimens highlight the importance of obtaining a personalized mutation profile for all newly diagnosed patients to guide the clinician on the most effective drug therapy to target tumors with a known mutation load.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.