
Abstract
Polycystic ovary syndrome (PCOS) is a chronic endocrine disorder affecting women of reproductive age, with a prevalence of about 10%. Hyperandrogenism, anovulation, polycystic ovarian morphology, and related hormonal and metabolic abnormalities are its hallmarks. This review focuses on the pathophysiologic landmarks, diagnostic criteria, and management strategies, including hormonal, metabolic, and pharmacological interventions associated with PCOS. Comprehensive literature collection was conducted using various scientific databases, including PubMed, PubMed Central, ScienceDirect, and Google Scholar, focusing on Rotterdam criteria, which include the presence of at least two of the following features: oligo- or anovulation, clinical signs of hyperandrogenism, elevated free androgen index levels in serum, and polycystic ovaries on sonography. The endocrine dysfunctions include hyperandrogenism (causing hirsutism and acne), anovulation with irregular menstruation, and multiple ovarian follicles. Management is individualized based on symptoms and fertility goals. Diagnosis is challenging due to the absence of a single definitive test, as PCOS is a multifactorial disorder. This review helps in the management and diagnosis of PCOS, and it is mainly based on the Rotterdam criteria and involves multiple pharmacological and supportive strategies.
Introduction
Polycystic ovary syndrome (PCOS) mainly impacts women in the childbearing years; it was first identified by scientists in the 1930s as Stein-Leventhal syndrome. This genetic disorder affects the normal process of the ovary and releases eggs; ovaries develop multiple pathological cysts as they become enlarged, as shown in Figure 1. The polycystic ovary has a thick center and more follicles than a normal ovary. Testosterone is produced in this location, which is referred to as the stroma. 1 The hallmark of PCOS is insulin resistance, which increases the lifetime risk of cardiovascular disease and calls for early detection and treatment. 2 Along with the traditional symptoms, PCOS is increasingly associated with psychological stress, psychosocial problems, and depression. Ovarian dysfunction and clinical and/or biochemical hyperandrogenism are included in the National Institutes of Health (NIH) criteria for PCOS. Later in 2003, the American Society for Reproductive Medicine (ASRM) and the European Society for Human Reproduction and Embryology (ESHRE) jointly sponsored a conference in Rotterdam, Netherlands, where a more comprehensive classification was carried out, taking into account the symptoms of NIH and the existence of polycystic ovarian morphology (PCOM). In 2006, the Androgen Excess Society (AES) established hyperandrogenism as a required criterion for PCOS, coupled with ovulatory abnormalities with or without PCOM. 3 The measurement of ovarian stromal volume, expressed as the S/A ratio (the ratio of stromal area to total ovarian area), is another diagnostic metric. A number of hypotheses have been put forth to explain the pathophysiology of PCOS, including endometrial progesterone resistance, a distinct defect in the action and secretion of insulin, a primary neuroendocrine defect that results in an exaggerated frequency and amplitude of the luteinizing hormone (LH) pulse, a defect in androgen synthesis that leads to an increase in the production of androgens in the ovaries, and a change in cortisol metabolism as a result of increased adrenal androgen production. 4 Ultrasound, computed tomography (CT) scanning, and magnetic resonance imaging (MRI) are frequently used to detect PCOS. PCOS currently has no known treatment or cure. Instead, each patient will receive treatment based on how their symptoms manifest. Oral contraceptives, hormonal therapy, glucocorticoids, gonadotropins, surgery, in vitro fertilization, lifestyle changes, fertility medications like clomiphene citrate (CC, the first line of treatment for ovulation induction), and other medications like metformin, troglitazone, and flutamide are all part of the fine line of treatment. 5
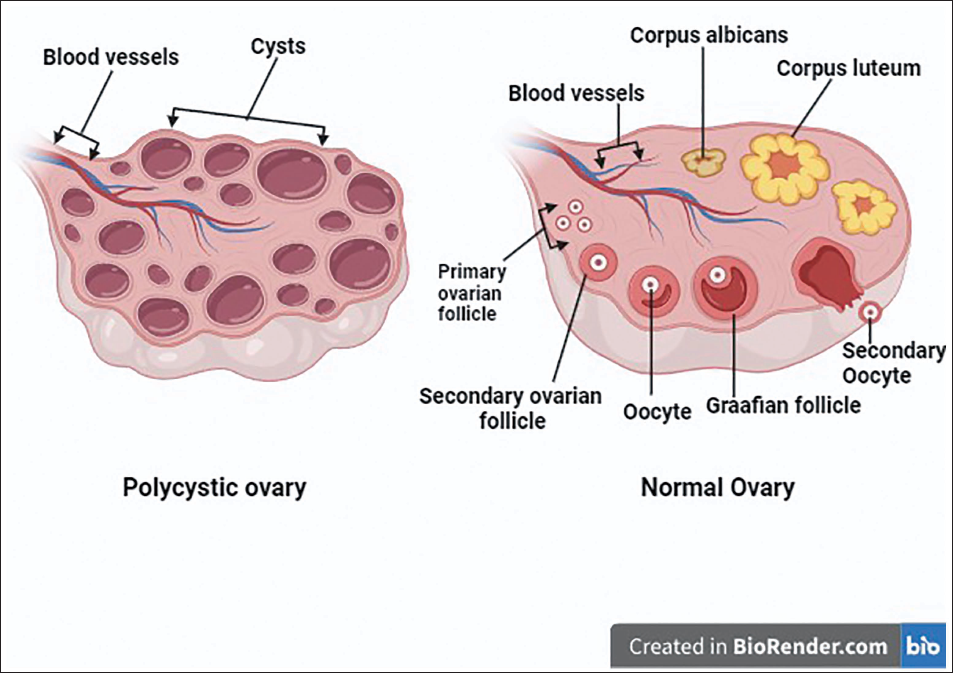
Internal Structure of Normal Ovary and Polycystic Ovary.
Causes and Symptoms of PCOS
It involves a variety of environmental, genetic, and hormonal problems, and the comparison is made with the general population. PCOS patients are also more likely to experience the morbidity associated with metabolic and cardiovascular illnesses. Ethnic considerations affect the phenotypic symptoms of PCOS (shown in Figure 2), even though the syndrome is equally prevalent throughout all nations. There is substantial evidence that women with PCOS are more likely to develop type 2 diabetes and, as some studies have shown, are also more likely to develop cardiovascular disease. 6
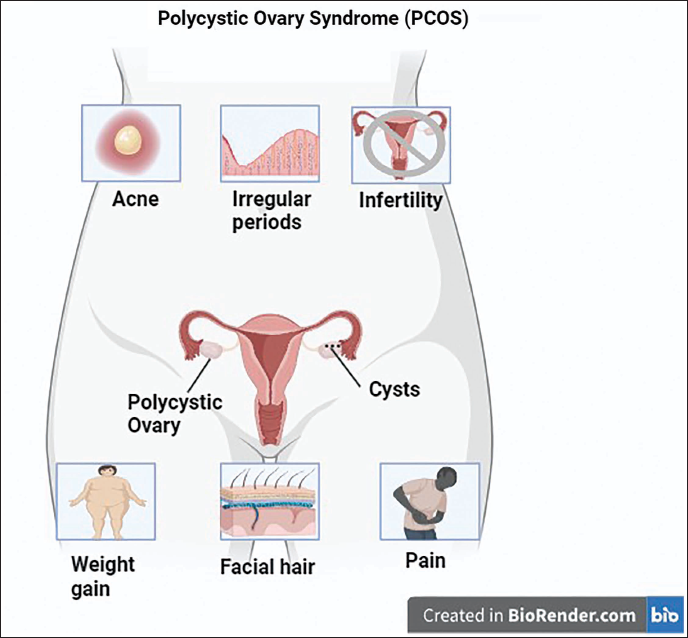
Different Types of Sign and Symptoms in PCOS Women.
Research Models of PCOS (In Vivo)
Exogenous androgens have been incorporated into various animal models in the last few years to investigate the part that developmental factors play in the pathophysiology of PCOS. Hyperandrogenism is a frequently observed clinical feature of PCOS patients. To imitate PCOS-like phenotypes in experimental animals, direct androgen therapy techniques have been performed with agents like dihydrotestosterone (DHT), testosterone propionate (TP), or dehydroepiandrosterone (DHEA). There have also been uses for other hormonal drugs, namely, glucocorticoids, human chorionic gonadotropin (HCG), anti-Müllerian hormone (AMH), and estradiol valerate (EV). In sheep and primates, the hormonal intervention administered was testosterone, which was conducted prenatally, whereas in rodents, the hormonal interventions administered were testosterone, which was conducted prenatally, and DHT and DHEA, which were administered postnatally. 7 Table 1 includes a list of the hormones that are administered to the animal models.
List of Direct Hormonal Interventions Induced in Animal Polycystic Ovary Syndrome (PCOS) Models. 7
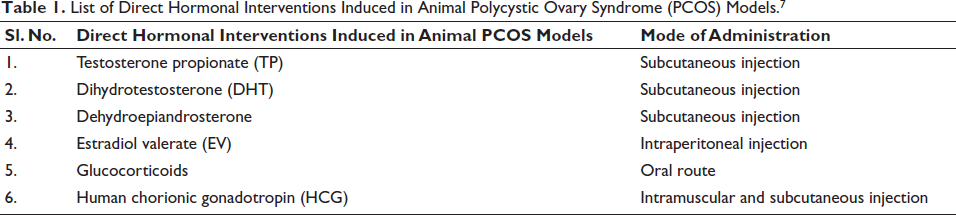
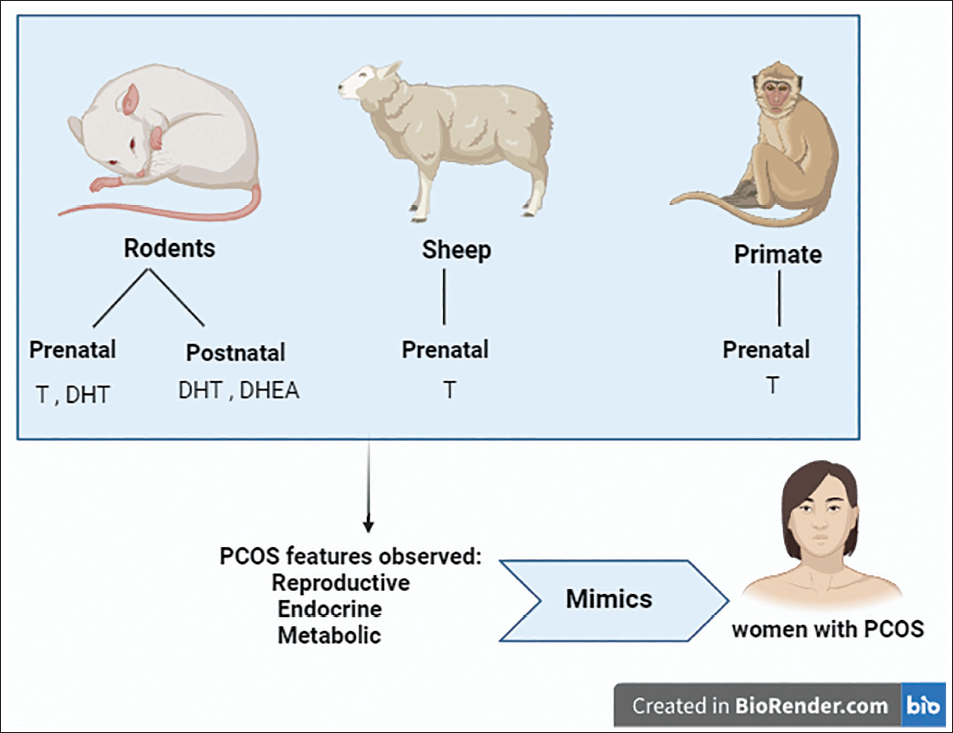
Figure 3 illustrates how these hormones might lead to PCOS-like phenotypes in rodents, sheep, and non-human primates via prenatal and postnatal administration. Prenatal therapy with testosterone or other steroids, which include DHT, EV, and steroid production inhibitors, is a common practice in animal models created to investigate PCOS. 8 The adult beginning of PCOS-like features occurs when testosterone is administered during the prenatal period in sheep and macaques and during the late prenatal and early postnatal period in rodents. 9 Prenatal exposure to testosterone causes a variety of adult reproductive disorders, especially in female sheep, such as functional hyperandrogenism, LH hypersecretion, altered neuroendocrine feedback mechanisms, multi-follicular ovarian morphology leading to early reproductive failure, and elevated pituitary sensitivity to gonadotropin-releasing hormone, also known as GnRH. 10 The endocrine precursors of the adult PCOS-like phenotype may include hyperandrogenism and LH hypersecretion, as evidenced by the observation of these traits in female rhesus monkeys treated with testosterone during pregnancy. Prenatal testosterone therapy in female sheep changes the balance of steroid receptors, causing the pituitary gland, ovaries, and brain to express more androgen receptors. 11
Pathophysiology of PCOS-induced Infertility
A PCOS patient’s primary reasons for seeking medical attention are hirsutism and infertility. Hyperandrogenism and menstrual cycle abnormalities, most often amenorrhea or oligomenorrhea, are present in a large number of individuals with PCOS-induced anovulation cases. 12
Several theories have been proposed to explain the pathogenesis of PCOS:
Endometrial progesterone resistance, A unique defect in insulin action and secretion, A primary neuroendocrine defect leading to an exaggerated LH pulse frequency and amplitude, A defect of androgen synthesis that results in enhanced ovarian androgen production, and An alteration in cortisol metabolism resulting in enhanced adrenal androgen production.
13
Hyperinsulinemia may also result in suppression of hepatic generation of sex hormone binding globulin (SHBG), which in turn increases androgenicity. In women with PCOS, there will be an imbalance between follicle-stimulating hormone (FSH), which stimulates the ovary to develop an egg, it ripens but does not rupture. Instead, it starts accumulating in the ovaries. By this time, LH level increases, egg may start to grow and remain as a cyst in the ovary as a result of occultation, which does not take place. Unruptured follicles produce testosterone. 14
Factors Affecting PCOS
Role of AMH in Placental Function in PCOS Women
Following the first trimester, AMH levels in PCOS women decrease; only in slim PCOS women do AMH levels stay noticeably higher during pregnancy. Maliqueo et al. demonstrated that placental Cyp19a1 expression was dramatically decreased by a daily dose of AMH between E16.5 and E18.5 of pregnancy. To shield the fetus from fetal androgen-induced virilization and to stop large amounts of androgens from building up in the mother’s bloodstream, placental aromatization is crucial. Remarkably, it has also been noted that PCOS women have higher placental 3-beta-hydroxysteroid-dehydrogenase-1 (3βHSD1) expression and lower placental Cyp19a1 expression. 15
Hyperandrogenism (Ovarian and Extra Ovarian)
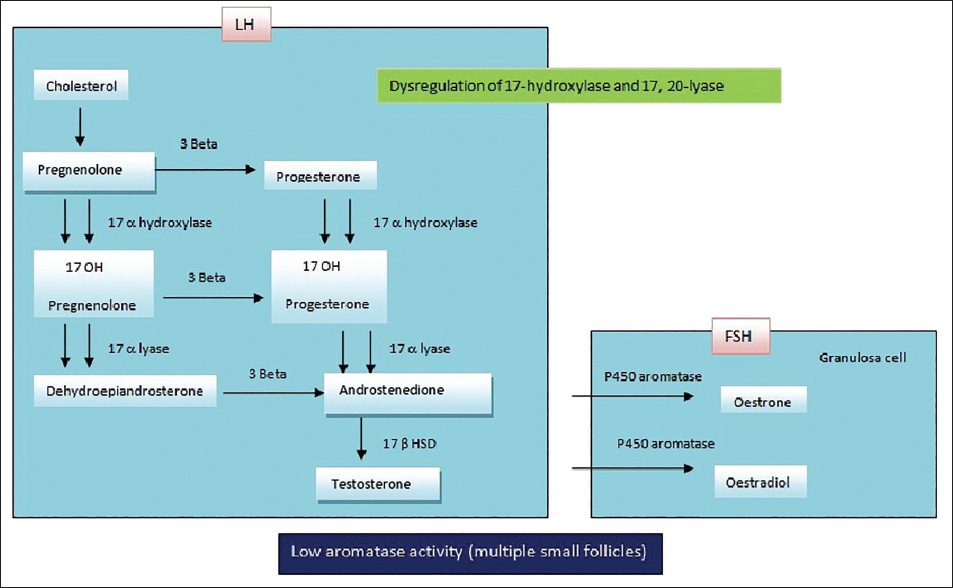
Hyperandrogenism is the most common hormonal change associated with PCOS. Biochemically, hyperandrogenism is typically measured by measuring the levels of androstenedione (A), dehydroepiandrosterone sulfate (DHEAS), SHBG, free testosterone (T), total testosterone (TT), and 17-hydroxyprogesterone (17-OHP) in serum, as well as by calculating the free androgen index. Microsomal P450c17 catalyzes 17–20 lyase activities (Figure 4), which is how androgens are biosynthesized. The pathophysiology of PCOS has been associated with transcriptional and post-transcriptional changes in P450c17. 16 There is a noticeable rise in the 17-OHP/A ratio in these women due to a relative inhibition of 17–20 lyase activity in comparison to 17-hydroxylase. 17-OHP is produced excessively when GnRH or HCG is administered to women with PCOS. High testosterone may be detrimental to the development of the ovaries, preventing meiotic maturation by reducing cytoplasmic calcium level oscillations inside the cell, and to follicular growth, resulting in atresia. 17
Role of Oxidative Stress (OS)
Reactive oxygen species (ROS) are physiologically implicated in numerous processes where they mediate various signal transduction pathways. When these compounds are overindulged, they can harm cells. Low egg maturation and poor embryo quality are closely linked to increased ROS in follicular fluid (FF) and decreased antioxidant capacity in PCOS-affected women. Through changes in follicular fluid factors (FFF) balance within the follicular milieu, these chemicals may lower the quality of oocytes. The documented mitochondrial malfunction in PCOS patients is explained by a decrease in glutathione (GSH) levels and mitochondrial O2 consumption, as well as an increase in ROS generation. Consequently, there is a further rise in the amounts of tumor necrosis factor-alpha (TNF-α), which is a known arbiter of insulin resistance. Inflammation brought on by the ensuing OS increases insulin resistance and fuels hyperandrogenism. 18
Insulin Resistance
Insulin resistance affects up to 70% of women with PCOS. The ovaries release more masculinizing hormones when there is an excess of insulin. One’s risk for type 2 diabetes can be elevated by obesity and insulin resistance, respectively. It can result in numerous obstetric difficulties and is a factor in infertility on its own. Anovulation is associated with obesity, in which body mass index (BMI) is >30 kg/m2, which raises the risk of infertility by increasing the androgen concentration. 19
PCOS and Pregnancy (Gestational Complications)
Pre-eclampsia, miscarriage, hypertension, gestational diabetes, and other pregnancy problems are more likely to occur in women with PCOS compared to normal women. They run a greater risk of an early birth and cesarean section because of these issues. Adipokines produced by adipose tissue include TNF-α, resistin, interleukin-6 (IL-6), adiponectin, and visfatin. These substances may be associated with the activation of insulin resistance during the gestational period. Additionally, changes in uterine vascularization observed in these women may indicate a decrease in trophoblastic invasion, which could result in a higher risk of hypertension and small for gestational age (SGA) births. 20
Diagnosis of PCOS
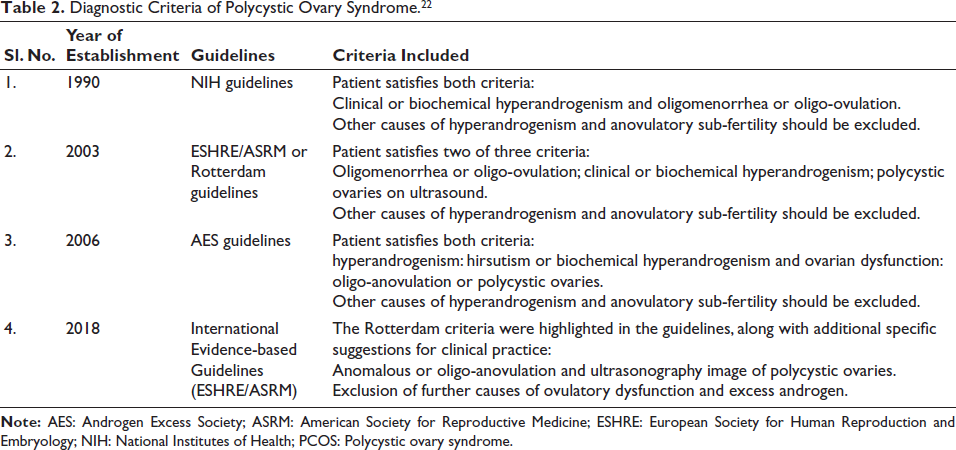
The NIH initially suggested a PCOS diagnostic standard in the early 1990s. After accounting for every other cause of anovulatory infertility, it classified PCOS as oligo-anovulation plus androgen excess. The NIH criteria were revised in 2003 by the ASRM and the ESHRE, who added the ultrasonography characteristics of polycystic ovaries as the third diagnostic criterion. 21 Based on expert advice from the 2003 Rotterdam conference, the AES stated in 2006 that the actual criteria established by the NIH in the 1990s can be credited with certain adjustments. The AES evaluated the available evidence for this purpose. The 2018 global PCOS guideline supported the Rotterdam criteria. 22 The numerous diagnostic criteria are listed in Table 2.
Diagnostic Criteria of Polycystic Ovary Syndrome. 22
Newer Biomarkers Used in the Diagnostic Process
Numerous proteins, hormones, metabolites, and genes can be employed as biochemical indicators for PCOS diagnosis and therapy. A significant contribution to the finding of biomarkers is made by proteomics associated with both phenotype and genotype. 23 The integration of a vast quantity of new data from proteomics might help clarify cellular changes that lead to PCOS illness, such as those involving multiple metabolisms, androgen biosynthesis, or chronic inflammatory pathways. In individuals with PCOS, copeptin levels are elevated in relation to lipids, insulin resistance, obesity, androgenic profile, and carotid intima-media thickness. 24 Different levels of copeptin are associated with different phases of PCOS that can therefore be used to predict the disease’s implications. Since serum kisspeptin levels are strongly correlated with androgenic profiles and have been found to be considerably higher in women with PCOS than in controls, kisspeptin may be a useful diagnostic for hyperandrogenism in PCOS. Metastin hormone levels have been found to increase in non-obese PCOS patients, and this can be used as a diagnostic sign. 25
A new protein called zonulin is a non-invasive indicator of intestinal permeability, and the lactulose/mannitol ratio is closely linked to serum zonulin levels. It serves as a biomarker for intestinal permeability in people with PCOS. Patients with obesity and insulin-resistant PCOS appear to have considerably higher blood zonulin levels, and the marker is linked to metabolic abnormalities and disruptions. 26 Complications of PCOS are also linked to SHBG. SHBG is a homodimeric glycoprotein that is mostly made by hepatocytes, although it is also found in the uterus, brain, testis, breast, ovaries, placenta, and prostate. A peptide hormone released from adipose tissue, leptin, is also increased in PCOS patients and has a role in controlling energy expenditure and long-term food consumption. Obese female PCOS patients have been found to have leptin and leptin receptors, and their free leptin index is greater than that of control subjects. Visfatin is shown to be increased in women with PCOS and may contribute to insulin resistance. 27
Imaging Techniques Used in the Diagnostic Process
Medical imaging techniques, including ultrasonography and MRI, are used to evaluate the ovaries in order to identify PCOS. It creates pictures of tissues and other interior organs using ultrasonic waves, which are high-frequency sound waves with a frequency of 2–15 MHz. Gray and white/black two-dimensional ovarian pictures are produced by the ultrasound instrument. There have been differences between the normal ultrasound pictures and the produced polycystic ovarian ultrasound images. The existence of follicles will next be ascertained by analyzing the ultrasonography. 28
miRNAs as Diagnostic Biomarkers
In PCOS-granulosa cells (GCs), free testosterone and free androgen index had a favorable correlation with miR-21 and miR-93. Similar effects on relative estrogen insufficiency were linked to miR-27a-3p, which may play a role in the pathogenesis of PCOS and promote GC apoptosis. 29 In PCOS-GCs, the expression of miR-93 is increased, while the cyclin-dependent kinase inhibitor 1A (CDKN1A), which is its expected target, is inhibited. 30 Therefore, in PCOS, miR-93 targets CDKN1A to enhance ovarian GC growth. According to this, women with PCOS may benefit from miRNA modification in terms of follicular health. Women with PCOS had significantly lower levels of miR-92a and miR-92b expression in their theca cells, according to case-control research by Lu et al. 31 According to research, PCOS theca cells have considerably greater levels of GATA6 and IRS-2. The protein of the significant androgen-production-related gene GATA6 has been demonstrated to increase the activity of the human CYP17 promoter. 32 By controlling the activity of thecal 17α-hydroxylase, the compounds produced by the insulin receptor gene IRS-2 raise PI3K activity and may further boost testosterone synthesis. In women with PCOS, the dysregulation of androgen production in theca cells may thus be related to the downregulation of miR-92a and miR-92b. In the adipose tissue of thin PCOS women, a number of miRNAs, including miR-123, miR-143, and miR-144, were overexpressed, suggesting that miRNAs play a part in insulin signalling. 33
Treatment and Management
As of right now, PCOS has no known cure. Although leading a healthy lifestyle would not cure PCOS, it will help manage related illnesses like obesity, heart disease, and infertility. PCOS patients may choose to use oral contraceptive pills (OCPs) in addition to anti-androgens to treat hirsutism, which is a prevalent symptom of the disease. 34
Chemical Treatments
Metformin
For women with extremely high BMIs or who are unable to lose weight, metformin can help to accelerate the rate of ovulation, pregnancy, or menstrual cycles. In contrast to estrogen antagonists, metformin treatment has been shown to enhance ovulation and pregnancy rates in PCOS women who are resistant to CC medication. If PCOS women used metformin during their pregnancies, the risk of miscarriage was significantly reduced. 35
CC
CC, an anti-estrogen, is the first medicine of choice for women who have been diagnosed with PCOS if the goal of treatment is pregnancy. It causes a rise in pituitary gonadotropin release, which attracts follicles. These medications will cause the ovulation of 75% of PCOS-afflicted women. 36
Gonadotropins
In order to induce ovulation in PCOS patients, gonadotropins are utilized as a second line of treatment. Several factors must be taken into account before PCOS patients begin gonadotropin therapy: low treatment response can be caused by ovarian volume, age, BMI, free androgen index, and length of amenorrhea. 37
Letrozole
As an aromatase inhibitor, letrozole functions by reversibly preventing androgens from being aromatized into estrogen. Because of this, the pituitary gland secretes more FSH as an outcome of blocking the negative feedback mechanism loop of estrogen on the hypothalamus. Starting from the 3rd to the 7th day of the menstruation, letrozole is administered for 5 days at a constant dose of 2.5–7.5 mg/day. 38
OCPs
Since OCPs are the first-line medication for concurrent treatment of hirsutism, acne, and irregular menstruation in women with PCOS, they are crucial in helping PCOS people control their symptoms. By inhibiting 5 alpha-reductase, estrogen also stops testosterone from being converted to the more powerful DHT. 39 Combinations of progesterone and estrogen do the following:
Decreasing the synthesis of ovarian androgen by decreasing the release of gonadotropin. Lower levels of free testosterone are the outcome of rising SHBG levels.
Preventing the production of androgens by the adrenal glands. 40
Cyproterone acetate (CPA), which has been used as an effective therapy for hirsutism, has significant progestogenic and anti-androgenic qualities. It also lowers circulation levels of testosterone and androstenedione by reducing circulating LH. 41
Adjunctive Therapy with Herbal Medications
One of the forms of alternative and complementary treatment is herbal medications, and over the past 10 years, women have used it much more frequently. 42
Cinnamon
A common herbal therapy in conventional medicine is cinnamon, which helps PCOS patient’s menstrual cycles to normalize. In females with PCOS, this clinical investigation showed that supplementing with cinnamon significantly lowers weight, fasting blood sugar (FBS), total cholesterol, fasting insulin, and low-density lipoprotein (LDL) levels when compared to a placebo. 43 The insulin-responsive tissues of individuals with extreme obesity or non-insulin-dependent diabetes mellitus (NIDDM) exhibit a substantial reduction in insulin receptor kinase autophosphorylation and consequent phosphorylation of its primary substrate. Tyrosine phosphatase inhibition by cinnamon would demonstrate that increased tyrosine phosphatase activity might be the cause of insulin resistance. By blocking glycogen synthase kinase 3β and activating glycogen synthase, cinnamon extract promotes the production of glycogen. It also decreases the absorption of glucose in the small intestine by reducing intestinal ATPase and enhancing glucosidase enzymes. 44
Curcumin
Among the active ingredients in the rhizome of the turmeric plant (Curcuma longa) is curcumin. A decrease in TNF-α expression was noted in the ovaries. Studies have demonstrated that curcumin lowers the elevated levels of androgen in PCOS. The amount of DHEA was lower in 67 PCOS-afflicted women who received 500 mg of curcumin powder three times a day for 12 weeks in a randomized controlled clinical study than in the placebo group. 45 In experiments on animals, the decrease in estradiol and progesterone levels in rats with PCOS was restored by treatment with 50 mg/kg nano curcumin and 200 mg/kg curcumin. Vascular endothelial growth factor (VEGF) is a proangiogenic factor that is intimately linked to the development of PCOS. 46
Surgical Approaches
In PCOS-affected women, laparoscopic ovarian drilling (LOD), ovarian wedge resection, and vaginal ovarian drilling (VOD) are the surgical methods used to promote ovulation. The increased risk of adhesion formation following surgery has led to the abandonment of ovarian wedge resection. 47
Newer Adjunctive Agents in PCOS Treatment
Resveratrol
As a natural defense mechanism in reaction to fungal, bacterial, and ultraviolet irradiation, plants create resveratrol, a naturally occurring polyphenol that may be found in peanuts, berries, and grapes. Resveratrol has been shown in several clinical trials to improve insulin sensitivity in people with type 2 diabetes by increasing liver fatty acid oxidation and reducing OS. 48 The concept that resveratrol could be helpful in PCOS treatment was motivated by the possible roles that persistent inflammation and resistance to insulin play in the etiology of PCOS. Resveratrol medication may enhance ovarian function and decrease the synthesis of testosterone by theca-interstitial cells, according to a recent review. Resveratrol has been found in vitro to improve PCOS (decreased androgen production), which may enhance the benefits of simvastatin. 49
Glucagon-like Peptide-1 (GLP-1) Receptor Agonist (RA)
A couple of minor randomized trials suggested that GLP-1 RA could be an appealing, novel treatment option for obese women with PCOS, particularly those with diabetes or insulin resistance. GLP-1 is a neuropeptide that boosts glucose-stimulated secretion of insulin and inhibits appetite and gastrointestinal motility. The agonists of the GLP-1 receptor (e.g., liraglutide) have been found to decrease body mass and levels of androgen and to improve insulin sensitivity. 50
Current Recommendations and Future Updates
New developments in PCOS are apparent from recent research in the following aspects. Trends indicate a growing recognition of PCOS as a multisystem disorder, with increasing emphasis on metabolic dysfunction, insulin resistance, and long-term cardiovascular risk alongside reproductive abnormalities. Consistencies across studies include the central role of hyperandrogenism, ovulatory dysfunction, and PCOM, as well as the frequent association with obesity and metabolic syndrome. Controversies persist regarding the most appropriate diagnostic criteria, the relative contribution of insulin resistance versus primary ovarian dysfunction in disease pathogenesis, and the heterogeneity of PCOS phenotypes across different ethnic and age groups.
Imbalance in the composition and function of the gut microbiota has been implicated in the promotion of systemic inflammation and insulin resistance, the two critical factors in the development of PCOS. Both probiotics and prebiotics are still studied concerning their ability to modulate the dysbiosis of the gut microbiota and decrease the impact of PCOS. The new development that is going to revolutionize treatment approaches in PCOS is going to be the concept of personalized medicine with special emphasis on the genetic and epigenetic variations. A lack of conclusive biomarkers, the paucity of longitudinal studies evaluating life-course outcomes, the underrepresentation of various groups, and the inadequate integration of genetic, environmental, and lifestyle variables are among the gaps in current research. By addressing these elements, the present PCOS research may be critically and systematically understood, and future research can be directed.
Conclusion
PCOS is a heterogeneous endocrine disorder with significant reproductive, metabolic, and neuropsychological consequences. Accurate diagnosis requires a differential approach based on the Rotterdam criteria, reflecting the interplay between genetic susceptibility and acquired disturbances such as insulin resistance and hyperandrogenism. Lifestyle modification remains the first-line intervention, while pharmacological therapies target metabolic and endocrine abnormalities. Advances in genetic markers, epigenetic regulation, and gut microbiota research have refined the understanding of PCOS pathophysiology and phenotypic variability. Integration of these molecular insights may facilitate precision-based therapeutic strategies and reduce long-term metabolic and cardiovascular complications associated with PCOS.
Footnotes
Abbreviations
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study did not require ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.