
Abstract
Background
MRSA and PRSP resistance has surged over 30 years, threatening clinical outcomes; China-developed cefathiamidine sodium, with enhanced pharmacokinetics, offers potent activity against these Gram-positive pathogens.
Purpose
This study evaluates the pharmacokinetic profile of injectable ceftriamidine sodium in healthy volunteers and compares its pharmacokinetics with those of cefathiamidine.
Materials and Methods
This clinical trial was a randomized and controlled study. The ceftriamidine sodium group (administered ceftriamidine sodium or placebo) employed a double-blind design with multiple administrations and dose escalation, whereas the cefathiamidine group (administered cefathiamidine) utilized an open-label design with single and multiple continuous administrations. The clinical trial involved ceftriamidine sodium at doses of 3.0 and 4.0 g, corresponding to cefathiamidine doses of 0.5 and 2.0 g. Volunteers received the corresponding drug infusions as per the protocol, and a series of blood samples were collected at specified time points for pharmacokinetic analysis.
Results
In the 3.0 and 4.0 g dose groups of ceftriamidine sodium, the t1/2, Tmax, and Cmax were 1.98–2.11 h, 0.50 h, and 321.14–448.80 µg/mL, respectively. Upon reaching steady state after multiple doses of 3.0–4.0 g, no significant drug accumulation was observed. Following multiple administrations of cefathiamidine at 0.5 and 2.0 g, the peak time at steady state was 0.50 h, t1/2 was 1.26–1.17 h, and Cmax was 48.11–194.40 µg/mL.
Conclusion
The half-life of ceftriamidine sodium (1.98–2.11 h) is almost twice as long as that of cefathiamidine (1.17–1.26 h), indicating its pharmacokinetic superiority in reducing the frequency of administration.
Introduction
In the past 30 years, the infection rates and drug resistance of Gram-positive bacteria have been increasing, which is not only manifested in the increase of hospital-acquired infections, but also in the increase of community-acquired infections.1, 2 In particular, the emergence and spread of multidrug-resistant bacteria such as methicillin-resistant Staphylococcus aureus (MRSA) and penicillin-resistant Streptococcus pneumoniae (PRSP) have brought great risks to clinical anti-infective treatment. 3 Finding effective drugs for Gram-positive bacteria has always been the focus of research and development of anti-infective drugs.4–6 Among the more than 50 listed cephalosporin antibiotics, cefathiamidine is the only cephalosporin antibiotic independently developed and applied in clinical practice in China, which fills the gap in the development and production of cephalosporin antibiotics in China.7, 8 Cefathiamidine is the first-generation cephalosporin approved by the China Food and Drug Administration for the treatment of sensitive bacterial infections in adults and children. 9 The anti-bacterial activity of cefathiamidine against Gram-positive cocci is better than that of the first- to fourth-generation cephalosporins, such as cefazolin, cefuroxime, ceftriaxone, and cefepime, especially for methicillin-sensitive Staphylococcus (MSS), Streptococcus [including Streptococcus pneumoniae (PSSP, PISP, and PRSP)], and other Gram-positive cocci. It is widely used in the treatment of community-acquired pneumonia (CAP), acute exacerbation of chronic bronchitis (AECB), skin and soft tissue infection, and sepsis caused by these sensitive bacteria.8, 10, 11
Ceftriamidine sodium is a derivative of cefathiamidine. The purpose of structural modification is to overcome the shortcomings of cefathiamidine, which has a short half-life in vivo and requires a large number of medications (intravenous (IV) drip 2.0 g/time, 2–4 times/day). 12 It is preliminarily predicted that ceftriamidine sodium has a good clinical application prospect for CAP caused by penicillin pneumococcal, methicillin-sensitive Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus viridans, non-hemolytic Streptococcus, Haemophilus influenzae, and Moraxella catarrhalis.
Materials and Methods
Study Design
This is a single-center, randomized, controlled trial. The experimental group (ceftriamidine sodium and placebo) was a multi-dose, dose-increasing, double-blind design, and the active control group (cefathiamidine) was a single + multiple continuous administration, open-label design. It has been registered at
The study drug was ceftriamidine sodium for injection, the active control was cefathiamidine for injection, and the placebo was 0.9% sodium chloride injection without the test drug. The single-dose study of ceftriamidine sodium for injection showed that doses from 0.1 to 8.0 g were well tolerated. Based on the single-dose PK/pharmacodynamic (PD) analysis, when the target (% fraction of time (fT) > minimum inhibitory concentration (MIC) = 50%) was met, the probability of target attainment (PTA) 90% corresponded to an MIC of 4 mg/L, indicating that the projected clinically effective human dose of ceftriamidine sodium is 6 g/day (3.0 g every 12 h). Taking into account the clinical dose ranges and PK profiles of similar drugs, the trial will use escalating multiple-dose regimens of 3.0 and 4.0 g. According to the approved data and package insert, the recommended IV dose of cefathiamidine for injection is 2 g per administration, 2–4 times daily for adults, and 50–100 mg/kg/day, divided into 2–4 doses for children. Therefore, based on the lowest and highest recommended doses, the positive-control group will consist of two dose cohorts: 0.5 and 2.0 g.8, 11
The ceftriamidine sodium 3.0 g group was planned to include 8 subjects receiving the study drug, 2 subjects receiving a placebo, and 10 subjects receiving 0.5 g cefathiamidine as an active control. The ceftriamidine sodium 4.0 g group was planned to include 8 subjects receiving the study drug, 2 subjects receiving a placebo, and 10 subjects receiving 2.0 g cefathiamidine as an active control. In the group receiving ceftriamidine sodium, subjects were given the drug twice daily on days 1–6 at 12-h intervals, followed by a single morning dose on day 7. A total of 13 doses were administered by IV infusion. In the cefathiamidine group, subjects received a single morning dose on day 1; on days 4–6, they were given four doses at 6-h intervals; and on day 7, they received one final morning dose, for a total of 14 IV infusions (Supplement Table S1).
Subjects
Qualified subjects were screened according to the inclusion and exclusion criteria. Inclusion criteria are as follows: (a) age ≥ 18 years old, both healthy males and females; (b) male body weight ≥ 50 kg or female body weight ≥ 45 kg, and body mass index (BMI) was 19.0–24.0 kg/m2 (including the two-end boundary value); (c) the subjects had no fertility plan in the next 3 months, voluntarily took effective contraceptive measures, and had no sperm/egg donation plan. Exclusion criteria are as follows: (a) glomerular filtration rate is less than the lower limit of the normal value of 90 mL/min; (b) subjects with known history of drug allergy (especially β-lactam drugs such as cephalosporins, penicillins, and other drug allergy history), ceftriamidine sodium (suitable for the experimental group) or cefathiamidine (suitable for the positive control group) skin (or intradermal) sensitivity test positive, or patients with allergic diseases (such as allergic rhinitis, asthma, urticarial, and eczema); (c) patients who received any drugs or health products within 28 days before administration were studied.
Study Assessments
Pharmacokinetics
Ceftriamidine sodium group D1: 1 h before administration in the morning, 15 min, 30 min (when the infusion was completed), 35 min, 45 min, 1 h, 1.5 h, 2 h, 4 h, 6 h, 8 h, and 12 h after administration; D6 within 1 h before administration in the morning and evening; D7 within 1 h before administration, 15 min, 30 min after administration (when the infusion was completed), 35 min, 45 min, 1 h, 1.5 h, 2 h, 4 h, 6 h, 8 h, 12 h, and 16 h; and on D8 (24 h after the last administration), 4 mL venous blood was collected with a vacuum blood collection tube containing dipotassium ethylenediaminetetraacetic acid (EDTA-K2). In the cefathiamidine group, within 1 h before administration in the morning, 10 min, 20 min, 30 min (when the infusion was completed), 35 min, 45 min, 1 h, 1.5 h, 2 h, 3 h, 4 h, and 6 h after administration; within 1 h before the third and fourth administration of D6, within 1 h before the first administration of D7, 10 min, 20 min, 30 min (when the infusion was completed), 35 min, 45 min, 1 h, 1.5 h, 2 h, 3 h, 4 h, and 6 h after the administration, 3 mL of venous blood was collected by vacuum blood collection tube containing EDTA-K2 precooled for at least 15 min in advance and stored in ice water bath. Blood samples were centrifuged within 1 h after collection, and centrifuged at 2°C–8°C and 1,700g for 10 min. The plasma samples were stored in an ultra-low temperature refrigerator at −60°C to 90°C. The plasma concentrations of ceftriamidine sodium and cefathiamidine were determined by a validated liquid chromatography–tandem mass spectrometry (LC–MS/MS) method. The linear range of ceftriamidine sodium standard curve was 1.50–1,500 µg/mL, and the lower limit of quantitation was 1.50 µg/mL. The linear relationship was good, and the extraction recovery range was 95.2%–96.1%. The intra-batch and inter-batch precision (% CV) were in the range of 3.5–10.6, and the accuracy was in the range of −1.2 to 5.1.
Statistical Analysis
Phoenix WinNonlin (ver 8.3) software was used for statistical analysis of PKs. Blood drug concentration data were analyzed by descriptive statistics according to dose and gender. It provides N, mean, standard deviation (SD), CV%, median, max, and min.
The non-compartmental model (NCA) method was used to calculate the main PK parameters, Cmax, ss, Tmax, ss, Cmin, ss, Cavg, ss, AUC0– t , ss, AUC0–∞, ss, AUC0–tau, ss,t1/2, ss, clearance (CL)ss, degree of fluctuation (DF), accumulation Index (AI), and others. For NCA, missing concentration values were left blank and not interpolated. Infusions that deviated >±5 min from the scheduled 30-min duration were accepted without adjustment; samples drawn >±2 min from the nominal time were adjusted to the actual recorded time before NCA. λz was estimated only when R² ≥ 0.85 and the extrapolated area under the curve (AUC) fraction was <20%. The PK parameters of each subject were calculated, and the descriptive statistical analysis of each parameter was performed according to gender and dose, including N, mean, SD, CV%, min, median, max, GeoNean, GeoCV%, and others. Student’s t-test was used to compare the significant differences in the main PK parameters between the sexes in each dose group.
Safety Evaluation
Performed with SAS version 9.4. Subjects were grouped by ceftriamidine sodium dose, cefathiamidine dose, or placebo; all placebo recipients were pooled into a single placebo cohort, hereafter referred to as the “treatment groups.” Findings were presented in summary tables (or figures) and listings, using descriptive statistics. Continuous variables were summarized with N, mean, SD, median, minimum, and maximum; categorical variables were summarized with counts and percentages. The evaluation criteria include adverse events (AEs), serious adverse events (SAEs), concomitant medications, changes in clinical laboratory results (hematology, blood chemistry, coagulation/hemolysis function, urinalysis, pregnancy test, and others), clinical signs and symptoms, vital-sign measurements, 12-lead electrocardiogram (ECG), and physical examination findings.
Results
Subjects
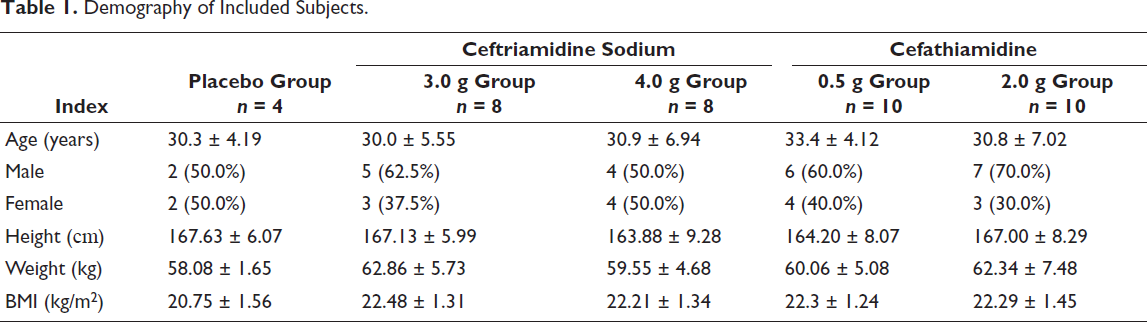
A total of 41 healthy subjects were enrolled in this study. The age was (31.3 ± 5.70) years old. There were 24 males and 16 females. The height was (165.76 ± 7.623) cm. The body weight was (60.89 ± 5.619) kg. The BMI was (22.16 ± 1.375) kg/m2. The experimental groups were balanced (Table 1).
Demography of Included Subjects.
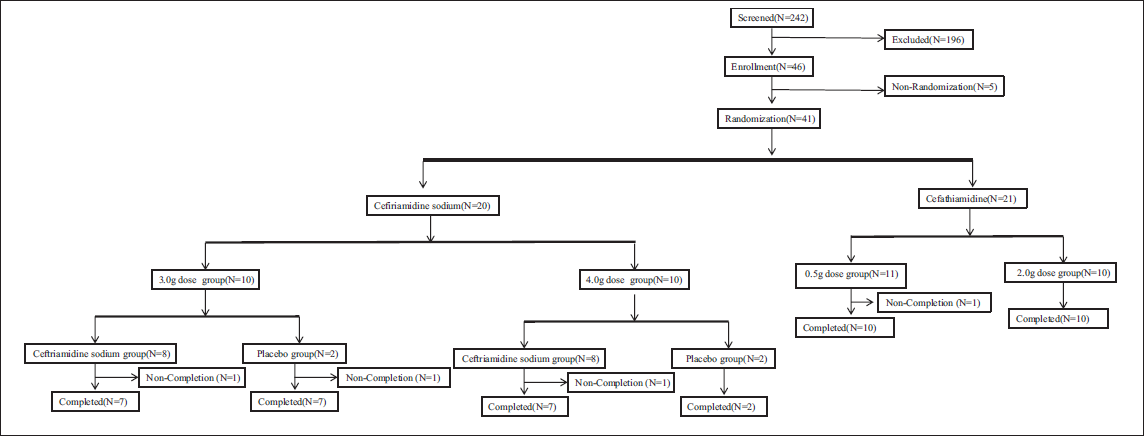
Among the 41 subjects enrolled in the group, 1 subject (0.5 g cefathiamidine group) withdrew from the trial early because the male-to-female ratio was less than 1/3, and did not receive the study drug administration. In the 3.0 g dose group of ceftriamidine sodium, two subjects withdrew from the test in advance, that is, one in the ceftriamidine sodium group, and one in the placebo group; in the 4.0 g dose group, three subjects withdrew from the trial in advance, all of which were in the ceftriamidine sodium group. One subject in the 0.5 g dose group of cefathiamidine group withdrew from the trial in advance, and 10 subjects in the 2.0 g dose group completed the trial (Figure 1).
The Flowchart of Clinical Study.
Pharmacokinetics
Pharmacokinetic Results of Ceftriamidine Sodium Group
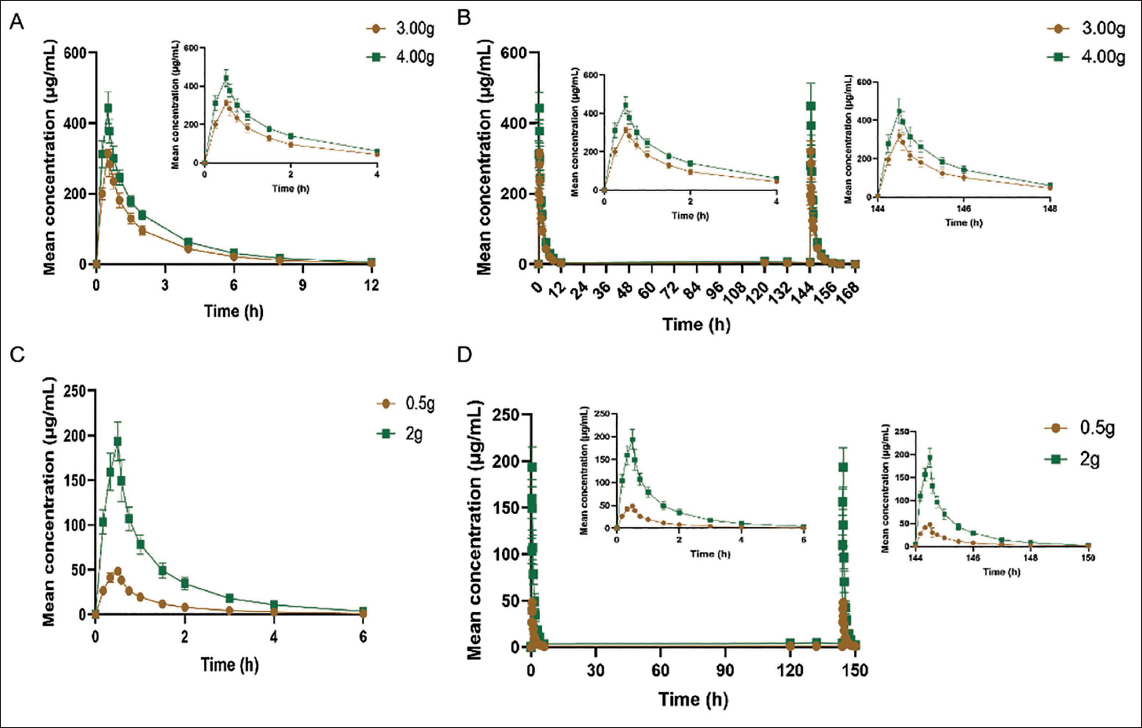
Based on the population pharmacokinetic study (PKCS), mean plasma concentration–time curves of ceftriamidine in blood were plotted for each dose cohort after single (Figure 2A) and multiple (Figure 2B) IV infusions of 3.0 and 4.0 g ceftriamidine sodium at the scheduled sampling times.
Mean Plasma Concentration–Time Curves of Ceftriamidine in Blood After Single (A) and Multiple (B) Intravenous Infusions of 3.0 and 4.0 g Ceftriamidine Sodium; Mean Plasma Concentration–Time Curves of Cefathiamidine in Blood After Single (C) and Multiple (D) Intravenous Infusions of 0.5 and 2.0 g Cefathiamidine.
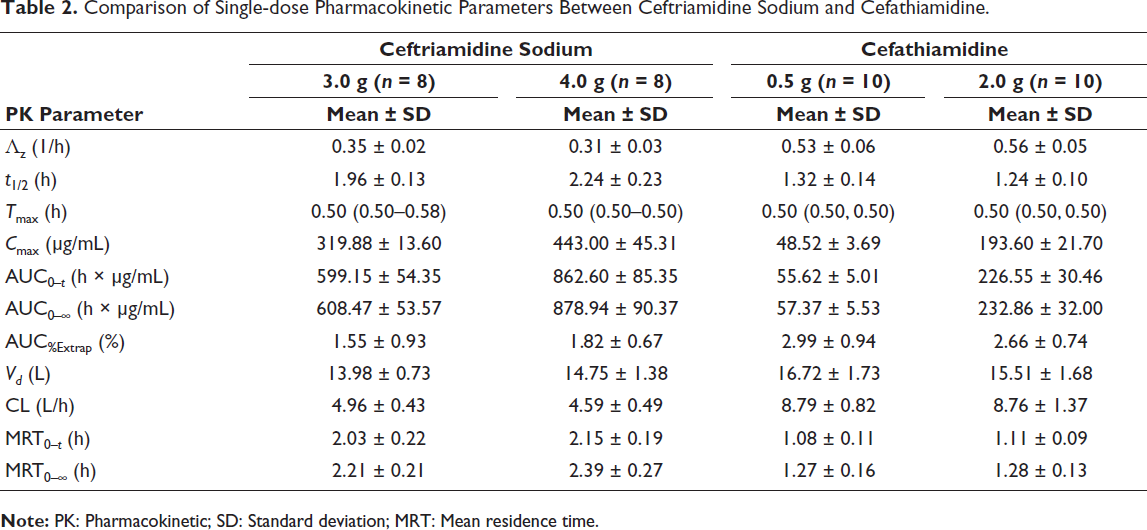
The 90% confidence interval (CI) of Cmax, AUC0– t , and AUC0–∞ in the first administration was 0.80–1.25, which was determined to be linearly proportional to the dose and had linear kinetic characteristics (Table 2). The 90% CI of Cmin, ss and AUC0–tau, ss at the last administration was 0.80–1.25, which was determined to be linearly proportional to the dose and had linear kinetic characteristics (Table 3). The 90% CIs of Cmax, ss, AUC0– t , ss, and AUC0–∞, ss were not in the range of 0.80–1.25, but the upper limit of the interval was within 1.25, and the lower limit of the interval was very close to 0.80. Therefore, it can be determined that although the dose and PK parameters do not show a strict linear proportional relationship, it can be considered to have linear kinetic characteristics. The main PK parameters of ceftriamidine sodium in the 3.0 g dose group for the first time and the last time and 4.0 g dose group for the first time were not significantly different between male and female by Student’s t-test (p > .05). The main PK parameters of ceftriamidine sodium in the 4.0 g dose group were not detected (ND) by Student’s t-test between male and female (Supplement Table S2).
Comparison of Single-dose Pharmacokinetic Parameters Between Ceftriamidine Sodium and Cefathiamidine.
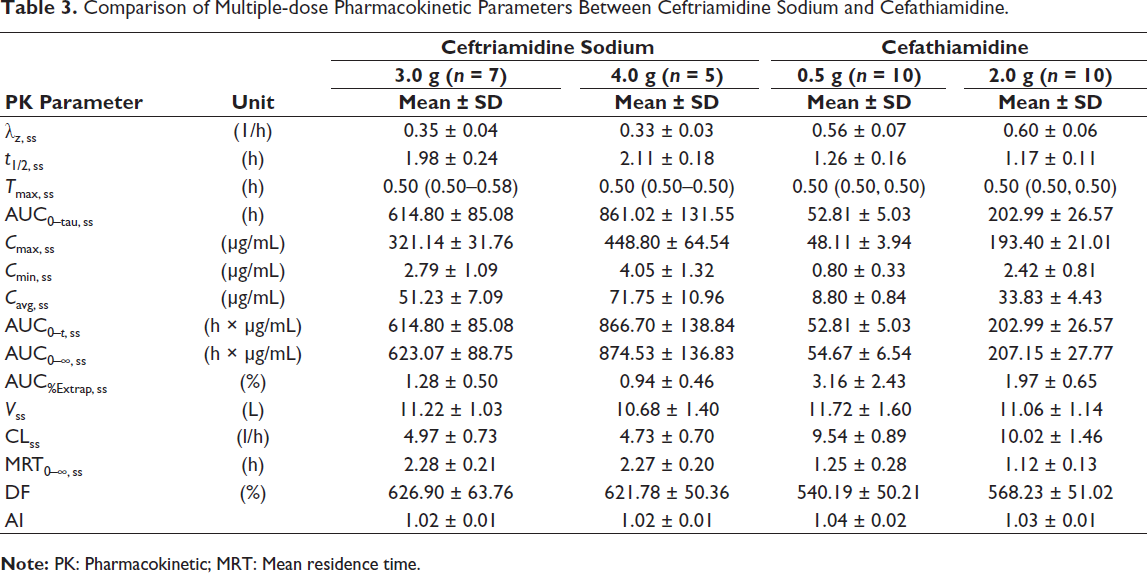
Comparison of Multiple-dose Pharmacokinetic Parameters Between Ceftriamidine Sodium and Cefathiamidine.
Pharmacokinetic Results of Cefathiamidine Group
Based on the PKCS, mean plasma concentration–time curves of cefathiamidine in blood were plotted for each dose cohort after single (Figure 2C) and multiple (Figure 2D) IV infusions of 0.5 and 2.0 g cefathiamidine at the scheduled sampling times.
The 90% CI of Cmax, AUC0– t , and AUC0–∞ in the first administration was 0.80–1.25, which was determined to be linearly proportional to the dose and had linear kinetic characteristics (Table 2). In addition to Cmin, ss, the 90% CI of Cmax, ss, AUC0– t , ss, AUC0–∞, ss, and AUC0–tau, ss was 0.80–1.25 at the last administration, which was linearly proportional to the dose and had linear kinetic characteristics (Table 2). The first and last main PK parameters of cefathiamidine in 0.5 and 2.0 g dose groups were significantly different between male and female by Student’s t-test, except for Cmin, ss in the 0.5 g dose group (p < .05; Supplement Table S2).
Comparison of PK Parameters Between Ceftriamidine Sodium and Cefathiamidine
The PK parameter comparisons of ceftriamidine sodium 3.0 and 4.0 g versus cefathiamidine 0.5 and 2.0 g after single and multiple administrations are shown in Tables 2 and 3.
The single and multiple administration exposures of ceftriamidine sodium 3.0 and 4.0 g dose groups were similar: single administration t1/2 was 1.96–2.24 h, and multiple administration t1/2 was 1.98–2.11 h; the tmax of single administration was 0.50 h, and the tmax of multiple administration was 0.50 h. The Cmax of a single dose was 319.88–443.00 µg/mL, and the Cmax of multiple doses was 321.14–448.80 µg/mL. There was no obvious drug accumulation after multiple doses of 3.0 and 4.0 g reached steady state.
The single-dose and multiple-dose exposures of cefathiamidine 0.5 and 2.0 g dose groups were similar: single-dose t1/2 was 1.24–1.32 h, and multiple-dose t1/2 was 1.17–1.26 h; the tmax of single administration was 0.5 h, and the tmax of multiple administration was 0.5 h. The Cmax of a single dose was 48.52–193.60 µg/mL, and the Cmax of multiple doses was 48.11–193.40 µg/mL. There was no obvious drug accumulation after multiple doses of 0.5 and 2.0 g reached steady state. Based on the t1/2 data of multiple administrations of the two drugs, the half-life of ceftriamidine sodium (1.98–2.11 h) was nearly twice as long as that of cefathiamidine (1.17–1.26 h).
Safety Evaluation
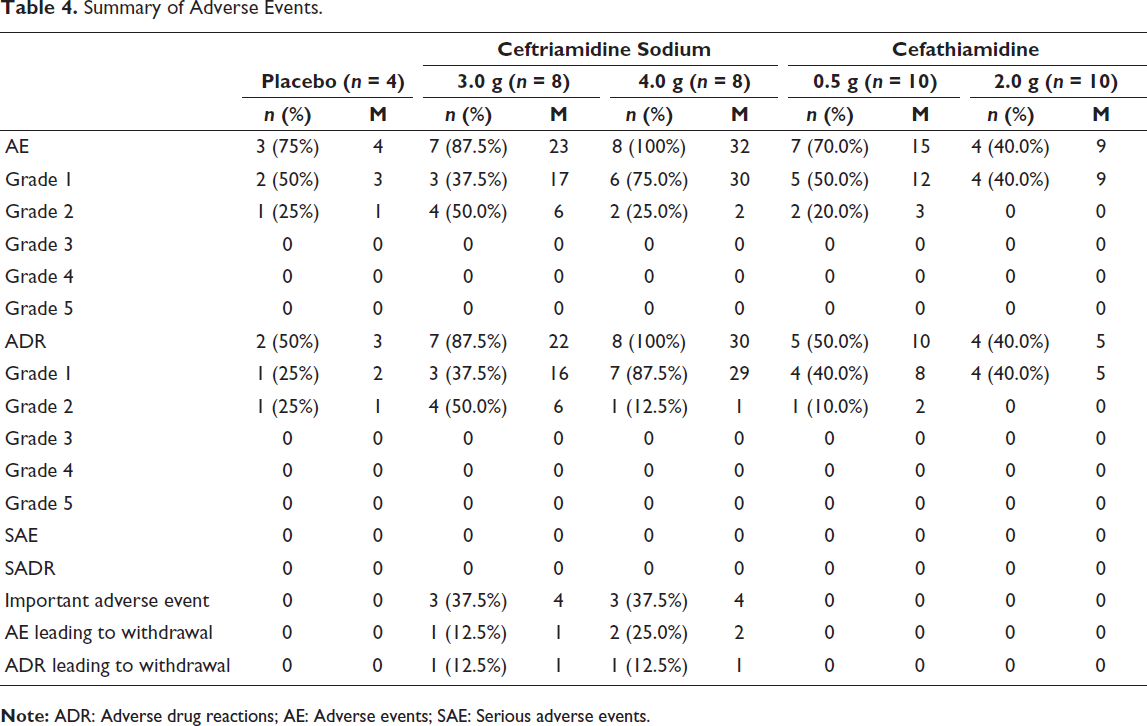
After multiple IV infusions of 3.0–4.0 g ceftriamidine sodium for injection in healthy volunteers, all AEs and adverse drug reactions (ADRs) were Grade 1 or 2; no AE or ADR of Grade ≥3 occurred. Except for one event whose outcome remained unknown (still present at the final visit), all other AEs resolved completely. Following multiple IV infusions of 0.5–2.0 g cefathiamidine in healthy volunteers, all AEs and ADRs were also Grade 1 or 2, with no Grade ≥3 events reported, and every AE resolved. Regarding tolerability, Grade ≥2 tolerability-related ADRs were observed in the ceftriamidine sodium, cefathiamidine, and placebo groups; no subject experienced Grades 3 and 4 tolerability-related ADRs or serious reactions (Table 4). The spectrum of AEs/ADRs reported for ceftriamidine sodium was consistent with the known safety profile of the drug. Common cephalosporin-class reactions include hypersensitivity, gastrointestinal disturbances and dysbiosis, hepatotoxicity, hematologic toxicity, renal impairment, and coagulation disorders.
Summary of Adverse Events.
Discussion
At present, cefathiamidine is the first-line drug for clinical anti-Gram-positive cocci infection.13, 14 The anti-bacterial activity of cefathiamidine against Gram-positive cocci is better than the representative drugs of the first to fourth generations of cephalosporins, such as cefazolin, cefuroxime, cefepime, and others. 15 Ceftriamidine sodium is a derivative of cefathiamidine. The introduction of N,N-diisopropylthiourea at the C7 position of cefathiamidine ensures the anti-bacterial activity against Gram-positive bacteria; at the same time, the C3 functional group is structurally modified to change its PK properties in vivo, thereby broadening the anti-bacterial range and improving drug stability. PD studies showed that ceftriamidine sodium especially enhanced the anti-bacterial effect on Streptococcus (including penicillin-insensitive Streptococcus pneumoniae), and the inhibitory effect on some negative bacilli, such as Haemophilus and Moraxella catarrhalis, was also enhanced.
The PK results obtained at present can basically reflect the exposure characteristics of ceftriamidine sodium in healthy subjects. The single and multiple administration exposures of ceftriamidine sodium 3.0 and 4.0 g dose groups were similar: single administration t1/2 was 1.96–2.24 h, and multiple administration t1/2 was 1.98–2.11 h; the tmax of single administration was 0.50 h, and the tmax of multiple administration was 0.50 h. The Cmax of a single dose was 319.88–443.00 µg/mL, and the Cmax of multiple doses was 321.14–448.80 µg/mL. There was no obvious drug accumulation after multiple doses of 3.0 and 4.0 g reached steady state.
The single-dose and multiple-dose exposures of cefathiamidine 0.5 and 2.0 g dose groups were similar: single-dose t1/2 was 1.24–1.32 h, and multiple-dose t1/2 was 1.17–1.26 h; the tmax of single administration was 0.5 h, and the tmax of multiple administration was 0.5 h. The Cmax of a single dose was 48.52–193.60 µg/mL, and the Cmax of multiple doses was 48.11–193.40 µg/mL. There was no obvious drug accumulation after multiple doses of 0.5 and 2.0 g reached steady state.
According to the t1/2 data of multiple administrations of the two drugs, it was verified that the half-life of ceftriamidine sodium was significantly longer than that of cefathiamidine, suggesting that the number of daily administrations could be reduced.
Conclusion
In summary, this study can fully reflect the PK characteristics of ceftriamidine sodium in healthy subjects after multiple administrations (3.0 and 4.0 g) and support the subsequent PK/PD characteristics of ceftriamidine sodium in patients with community-acquired bacterial pneumonia.
Footnotes
Acknowledgments
This study was a registered clinical trial, which was funded by Baiyunshan Pharmaceutical Factory of Guangzhou Baiyunshan Pharmaceutical Group Co., Ltd. The authors thank the trial participants, their families, and all investigators involved in this trial.
Abbreviations
Authors’ Contributions
Huan Zhou and Fei Qin participated in the conception and experimental design of the article, and Zihan Liu, Ganmi Wang, Ning Chen, Jiarong Wu, and Yueyuan You participated in the writing of the article.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The development of this clinical trial will strictly follow the test plan, the Helsinki Declaration, and the “Good Clinical Practice” (GCP) promulgated by the National Drug Administration (NMPA) and the relevant laws, regulations, and guidelines. This experiment was approved by the Ethics Committee of the First Affiliated Hospital of Bengbu Medical College, Ethical No. 2023026. All subjects signed the informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Guangdong Science and Technology Program (2020A1515111195) and Longhu Talent Project of Bengbu Medical University (LH250101002).
Trial Registration
Registered 03/17/2023 (
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.