
Abstract
Background
Intraoperative hypothermia is a common complication in elderly patients undergoing joint replacement surgery that can lead to adverse outcomes.
Objectives
This study aimed to analyze the pertinent risk factors influencing intraoperative hypothermia in elderly patients undergoing joint replacement and to develop and validate a risk prediction model.
Materials and Methods
A retrospective analysis was conducted on clinical data from 302 elderly patients undergoing hip joint replacement surgery. These patients were divided into two groups: the hypothermia group (intraoperative hypothermia (IH) group) and the non-hypothermia group (non-IH group) based on the presence of intraoperative hypothermia. Single-factor and multivariate logistic regression analyses were employed to identify the risk factors associated with intraoperative hypothermia in elderly joint replacement patients and to establish a predictive model for hypothermia risk. The receiver operating characteristic curve (ROC) was utilized to assess and validate the model.
Results
Among the 302 patients, 92 experienced intraoperative hypothermia, resulting in an incidence rate of 30.46%. Multivariate logistic regression analysis revealed that age and fasting time were independent risk factors for hypothermia, whereas body mass index (BMI), baseline temperature, preoperative heart rate, and anesthesia method were identified as protective factors (p < .05). ROC curve analysis demonstrated an area under the curve (AUC) of 0.902, sensitivity of 71.4%, and specificity of 93.0%. The calibration of the prediction model exhibited satisfactory consistency between actual hypothermia occurrences and predicted outcomes.
Conclusion
The risk prediction model developed in this study exhibits robust predictive performance and holds significant clinical utility.
Introduction
Total hip arthroplasty is a well-established surgical procedure replacing the artificial joint of the femur and acetabulum, representing a mature and reliable treatment modality. 1 Reports indicate a 45% incidence of knee joint lesions in individuals over 60 years old in China, with this demographic comprising the primary group undergoing hip arthroplasty. 2 Intraoperative hypothermia (IH) occurs when a patient’s body temperature drops below 36°C during anesthesia and surgery due to various factors. 3 This condition can have numerous adverse effects, including metabolic slowdown, diminished cardiopulmonary function, reduced blood circulation, and heightened risk of postoperative complications such as infection, shock, and bleeding.4, 5 Moreover, it may impede postoperative recovery, prolong rehabilitation duration, and escalate hospitalization and medical costs. Therefore, vigilant monitoring of elderly total hip arthroplasty patients’ body temperature during surgery is imperative to promptly detect and rectify hypothermia, thus mitigating the risk of complications. 6 Preoperative assessment of patients’ overall condition and implementation of hypothermia prevention measures are pivotal in enhancing surgical success rates and facilitating patient recovery. 7 This study aims to develop a risk prediction model for anticipating intraoperative hypothermia during elderly total hip arthroplasty and assessing its efficacy. Through this model, high-risk patient groups can be identified beforehand, preventive measures can be instituted, intraoperative hypothermia can be reduced, and ultimately, surgical success rates and postoperative recovery quality can be improved.
Materials and Methods
General Information
A retrospective analysis of patients undergoing surgery in our department from January 2018 to June 2023 was conducted. Inclusion criteria comprised age ≥60 years, all having undergone hip arthroplasty, complete clinical data, and patient consent. Exclusion criteria included concurrent cerebrovascular diseases, traumatic brain injury, temperature regulation dysfunction, allergy to anesthetic drugs, and previous hip joint surgery. Approval from the ethics committee was obtained. Collected clinical data encompassed age, gender, body mass index, diabetes mellitus, hypertension, surgical history, fasting duration, baseline temperature, preoperative heart rate, preoperative systolic blood pressure, preoperative hemoglobin, American Society of Anesthesiologists (ASA) classification of anesthesia, anesthesia method, intraoperative core temperature, and so on. Patients were categorized into hypothermia and non-hypothermia groups based on intraoperative core temperature (<36°C).
Temperature Measurement and Hypothermia Criteria
Intraoperative hypothermia was determined based on core body temperature, typically measured at sites like the esophagus, rectum, tympanic membrane, or nasopharynx. This study used a monitor to measure nasopharyngeal temperature as the core body temperature measurement site, recorded every 5 min from anesthesia induction to operating room exit. Intraoperative hypothermia was defined as nasopharyngeal temperature ≤36.5°C at any time point.
Statistical Analysis
SPSS 21.0 software facilitated statistical analysis. Count data were presented as rates and assessed using the chi-square test. Ranked data were analyzed using the rank-sum test, while measurement data were expressed as mean ± standard deviation and analyzed via the t-test. Single-factor and multivariate logistic regression analyses identified influencing factors and constructed the risk prediction model. The receiver operating characteristic (ROC) curve evaluated the model’s predictive value, with p < .05 indicating statistical significance.
Results
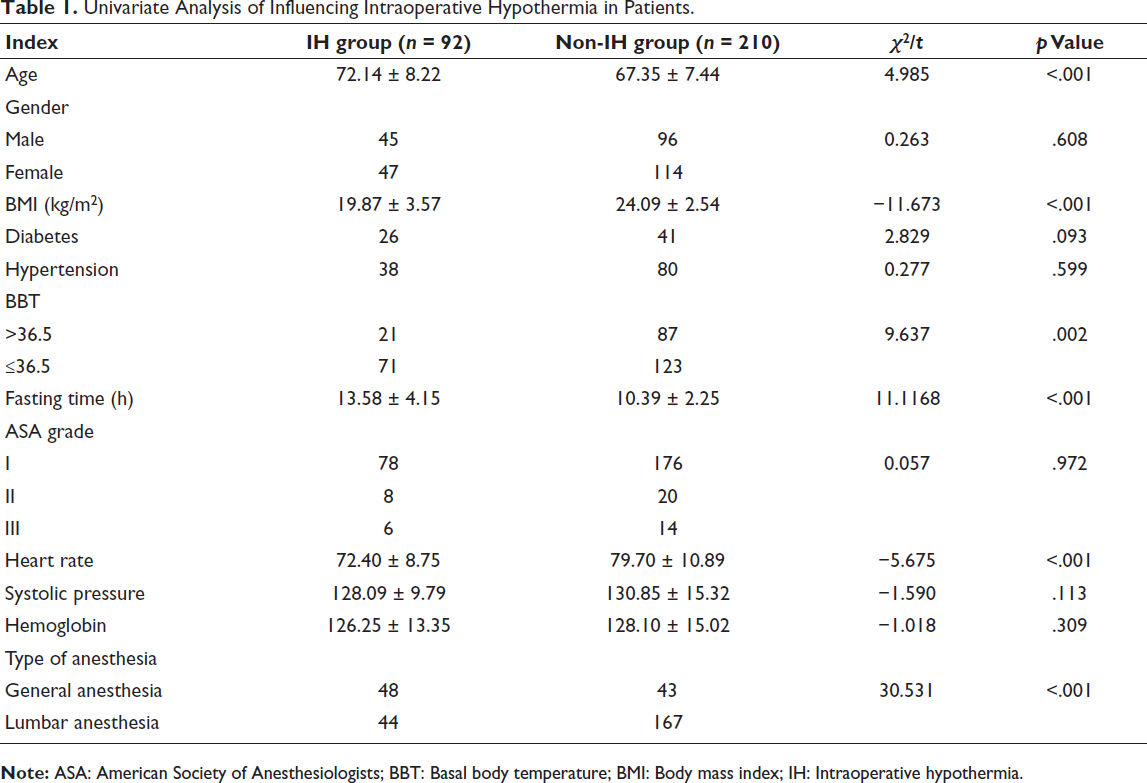
Univariate Analysis of Influencing Intraoperative Hypothermia in Patients
Out of the 302 patients, 92 experienced intraoperative hypothermia, yielding an incidence rate of 30.46%. The single-factor analysis revealed significant differences in age, body mass index (BMI), baseline temperature, fasting time, preoperative heart rate, and anesthesia method between the two groups (p < .05). Refer to Table 1 for details.
Univariate Analysis of Influencing Intraoperative Hypothermia in Patients.
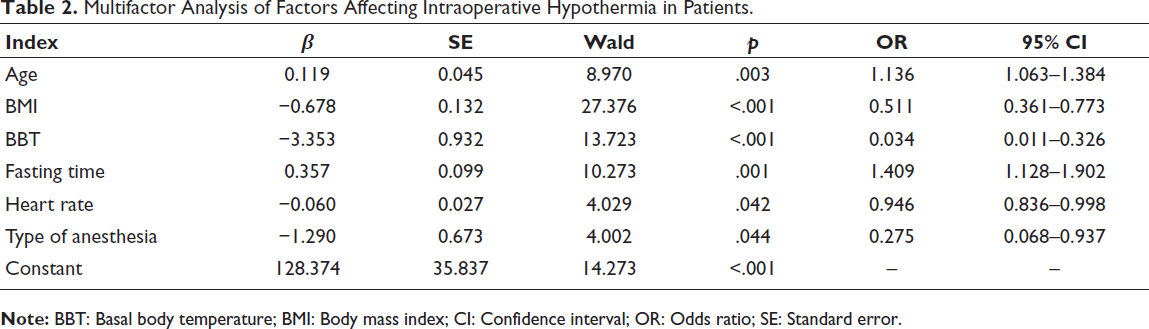
Multifactor Analysis of Factors Affecting Intraoperative Hypothermia in Patients
The multifactor logistic regression analysis included all significant indicators identified in the single-factor analysis. The results demonstrated that age and fasting time independently posed risks for intraoperative hypothermia, whereas BMI, baseline temperature, preoperative heart rate, and anesthesia method acted as protective factors (p < .05) (Table 2).
Multifactor Analysis of Factors Affecting Intraoperative Hypothermia in Patients.
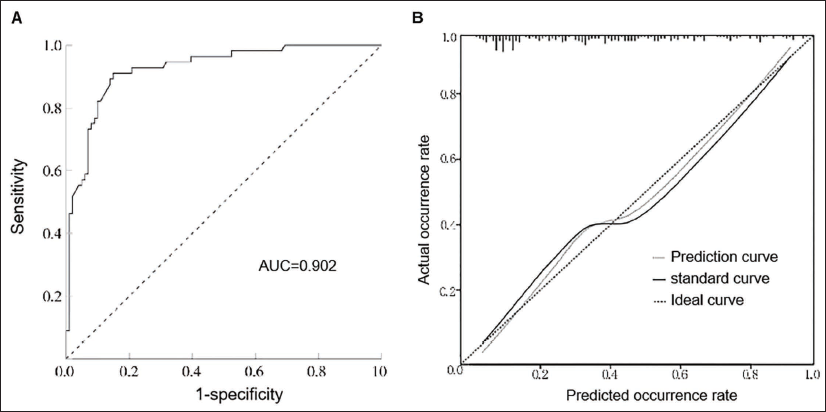
Development and Validation of a Risk Prediction Model for Intraoperative Hypothermia in Elderly Hip Arthroplasty
The model was established based on the findings of multifactor logistic regression analysis: Logit (P) = 128.374 + 0.119 (Age) − 0.678 (BMI) − 3.353 basal body temperature (BBT) + 0.357 (Fasting time) − 0.060 (Heart rate) − 1.290 (Type of anesthesia). Internal validation of the model was performed using the ROC curve and calibration plot. Results indicated an AUC of 0.902 for the ROC curve (Figure 1A), with a cutoff value of 0.516, sensitivity of 71.4%, and specificity of 93.2%. The calibration plot of the prediction model (Figure 1B) exhibited strong alignment between the predicted probability of intraoperative hypothermia in elderly hip arthroplasty patients and the actual occurrence probability.
Discussion
Intraoperative hypothermia, characterized by an unplanned decrease in body temperature below 36°C during surgery, represents a common complication. 8 While perioperative hypothermia in surgical patients is often overlooked due to mild symptoms, its severe form can lead to adverse outcomes. For example, a mere 0.5°C reduction in body temperature can trigger shivering, with shivering severity correlating with the degree of temperature decline. Shivering elevates oxygen consumption and CO2 levels and exacerbates cardiac workload, heightening the risk of cardiovascular diseases. 9 Furthermore, hypothermia diminishes circulating blood volume, alters coagulation function, and consequently impacts wound healing and increases postoperative infection rates. Hence, preventing perioperative hypothermia is paramount. 10
Orthopedic surgeries are particularly susceptible to hypothermia due to factors such as indoor environmental conditions, exposure to abdominal and limb areas, and prolonged general anesthesia. 11 Additionally, general anesthesia can suppress metabolism, thus augmenting the risk of hypothermia and resulting in intraoperative bleeding, shivering, incisional pain, and potentially cardiovascular complications. Conventional perioperative temperature management, such as blanket coverage and room temperature adjustment, often overlooks other hypothermia-contributing factors, leading to suboptimal insulation. 12
Intraoperative temperature monitoring and warming are standard nursing practices. However, the occurrence of IH in joint replacement surgery patients remains challenging. The majority of such patients are elderly, making them more susceptible to IH, which is associated with increased perioperative complication rates and mortality. 13 Consequently, predictive models are crucial for preventing IH in patients. While many medical professionals recognize the dangers of IH and are beginning to use predictive models, research on IH prediction models for joint replacement surgery is lacking. 14 This study aims to identify IH risk factors in joint replacement surgery and develop a tool for identifying high-risk patients. Multifactor regression analysis revealed that age and fasting time are independent IH risk factors. BMI, baseline body temperature, preoperative heart rate, and anesthesia method (epidural anesthesia) act as protective factors. Advanced age, low BMI, patient physiological factors, and anesthesia are identified as IH risk factors.
The body’s dynamic temperature equilibrium is upheld by various systems, which naturally decline with age. 15 Aging diminishes skin temperature receptor sensitivity, reduces skeletal muscle heat production in cold environments, and accelerates heat dissipation due to decreased skin vascular elasticity, rendering elderly patients more susceptible to IH. Moreover, body fat serves as thermal insulation; higher fat content reduces temperature differences between the skin and the external environment, thereby maintaining normal body temperature. Individuals with lower BMI are thus more prone to IH. Baseline body temperature significantly impacts IH risk, correlating with core heat redistribution. Patients with lower baseline body temperature exhibit greater core skin temperature differences, leading to increased core heat redistribution and subsequent IH. Preoperative warming measures mitigate IH occurrence, while preoperative heart rate reflects the sympathetic nervous system’s regulation of blood flow to maintain body temperature. 16 Prolonged fasting results in inadequate calorie intake and reduced calorie conversion, leading to decreased body temperature. Low body temperature can cause coagulation dysfunction, increased intraoperative blood loss, and decreased body temperature during general anesthesia, resulting in peripheral vasodilation, accelerated heat dissipation, and subsequent hypothermia. 17
Conclusion
The predictive model developed in this study demonstrates good accuracy and discriminative ability, serving as a reference for personalized IH prevention. However, being a single-center study limited to patients in our hospital, it may suffer from sample selection bias due to its relatively small sample size. Future research will involve multicenter collaboration, expanded sample sizes, incorporation of additional variables, and ongoing optimization of the predictive model for intraoperative hypothermia risk in such patients.
Footnotes
Abbreviations
ASA: American Society of Anesthesiologists; AUC: Area under the curve; BBT: Basal body temperature; BMI: Body mass index; IH: Intraoperative hypothermia; Non-IH: Non-intraoperative hypothermia; ROC: Receiver operating characteristic.
Acknowledgments
The authors appreciate the helpful technical assistance provided by the staff of the Orthopedics Department of Dongtai People’s Hospital.
Authors’ Contribution
YC: Conceptualization, project administration, data curation, formal analysis, investigation, methodology, software, writing—original draft; JZ: Conceptualization, formal analysis, methodology, supervision, writing—review & editing.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Human Ethics Committee of Dongtai People’s Hospital (Approval No. 22-117). This study was conducted in accordance with the guidelines of the International Medical Journal Editorial Board and the Helsinki Declaration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Due to the retrospective nature of this study, each patient’s consent to withdraw was obtained, and detailed information can be found on our hospital’s bulletin board.