
Abstract
Mushroom poisoning has been identified as a primary cause of both foodborne disease outbreaks and related fatalities in China. Depending on the mushroom species ingested, target-organ damage can usually be attributed to the toxins presenting in the mushroom species ingested, which can ultimately lead to organ failure and death. Developing a joint risk prediction model for death caused by acute mushroom poisoning could accurately predict the risk of mortality in such cases, early initiation of bundled treatment could significantly reduce mortality.
Methods
This single-center, retrospective observational study was conducted on 455 patients with Undergoing Treatment for Mushroom Poisoning at Affiliated Hospital of Zunyi Medical University (AHZMU), the tertiary governmental hospital of China, between January 2013 and December 2020. We investigated the impact of prognostic factors, including the mortality rate of patients who completed treatment at AHZMU versus those transferred to AHZMU, average length of hospital stay, mortality rate for a latency period of > 6-h, major damaged organs, HOPE6-TALK scoring and established a predictive model to assess the severity of acute mushroom poisoning.
Results
In 2013-2020, there are 455 patients of mushroom poisoning at AHZMU. Mushroom poisonings mainly concentrated in the summer and autumn months, resulted in 47 patients deaths. The first diagnosis cases at AHZMU resulting in a case fatality rate of 12.77% (6/47), Non-first diagnosis patients fatality accounting for 87.23% (41/47). The majority of deaths (89.36%) were attributed to liver injury. Death with incubation period >6-h accounting for 70.21% (33/47) of the total mortality rate. Logistic regression analysis revealed age and HOPE6 scores as independent risk factors, thereby establishing the logistic model equation, an examination via the ROC curve analysis indicates that a combination predictor values (Ycoalition) of 289.6 is the cut-off values for death resulting from acute mushroom poisoning.
Conclusion
The attending physician should conduct an early HOPE6-TALK scoring and calculate the Ycoalition for patients with acute mushroom poisoning, as well as promptly identify the toxic mushrooms through morphological and molecular biological identification. Identify mushroom species and further infer the clinical type and clinical characteristics. For example, amanitoxion can cause acute liver injury with high mortality. Identify mushroom species that may cause organ damage so that timely implementation of the bundled therapy for poisonous mushrooms will increase the cure rate and reduce the mortality rate (Lu et al., 2019).
Introduction
Mushrooms are known for their umami taste and high nutritional value, making them a popular food source worldwide. However, mistaking poisonous mushrooms for edible ones is a global food-safety issue posing a significant threat to human health, and one of the leading causes of death from food poisoning. There are approximately 14,000 types of mushrooms worldwide, with 1020 edible, 692 medicinal, and 480 toxic mushrooms having been identified in China alone.1–3 Mushroom poisoning is relatively common in China, with the highest incidence rates reported in the southwest and central regions. Outbreaks typically occur during the warm and rainy summer and autumn months, often due to the self-harvesting and consumption of mushrooms.1,4 Identifying toxic mushrooms based on their appearance is not an easy task. While gastrointestinal symptoms are the most common among mushroom-poisoning cases and typically have a good prognosis, poisoning can also lead to hepatic and renal impairment, rhabdomyolysis, and other serious conditions that can contribute to death. Fatal amanita poisoning is responsible for over 90% of all fatal mushroom-ingestion cases globally. Amatoxin mushroom poisoning accounts for 90% of the total mushroom-poisoning deaths in China.5–7 Due to its rapid progression, complex mechanism of action, and high case-fatality rate, it is critical to recognize, diagnose, and treat this disease early.
Thus, to address this issue, We collected data on 455 patients with mushroom poisoning admitted to the Affiliated Hospital of Zunyi Medical University (AHZMU) between 2013 and 2020. We aimed to describe the epidemiological characteristics of these patients, analyze and explore risk factors, propose early identification methods for critically ill patients, and suggest effective control measures.
Methods
This single-center, retrospective observational study was conducted at AHZMU, the tertiary governmental hospital of China, between January 2013 and December 2020. The objective of this study was to evaluate the prognostic impact of treating patients directly at AHZMU versus transferring them to AHZMU, and to establish a predictive model for assessing the severity of acute mushroom poisoning. The study adhered to the principles of the Declaration of Helsinki, and received approval from the Affiliated Hospital of Zunyi Medical University Ethics Committee [KLL-2022-610]. The study findings were reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 8
Data sources and research methods
Included a total of 455 patients of mushroom poisoning treated at the AHZMU from January 2013 to December 2020. All patients were selected based on their history of consuming mushrooms and relevant symptoms of mushroom poisoning. We excluded patients with a previous history of chronic respiratory, liver, kidney, and hematologic diseases and other similar conditions. Such as patients with COPD, cirrhosis, uremia, etc. that cause respiratory, liver and kidney function, and coagulation function abnormalities.
Analyzed clinical data from all enrolled patients, including the following: age, sex, home address, admission date, latency period, prognosis, blood work, biochemical tests, coagulation function, and inflammatory response following admission. Additionally, we recorded the HOPE6-TALK scoring and assessed patients for organ damage. All patients were initially treated based on the severity of their poisoning and clinical symptoms. Subsequently, their organ functions were assessed to determine the need for blood-purification intervention, including hemoperfusion, plasma exchange, and continue renal replacement therapy (CRRT). The study was conducted following the guidelines set by the Basic and Clinical Pharmacology and Toxicology Policy for Experimental and Clinical Research.
Statistical analysis
Statistical analyses were performed using SPSS version 25.0 for Microsoft Windows (SPSS, Inc, Chicago, IL, USA). For measurements that met the normal distribution, the t test was used for comparison between groups and presented as the mean ± standard deviation; the quality of measurement that did not meet a normal distribution was presented as the median (interquartile range); the Mann–Whitney U test was used for comparison between groups as well as to analyze continuous variables. A Chi-squared test was used for the analysis of categorical variables. One-way analysis of variance and binary logistic regression were used to determine the odds ratio (OR) and confidence interval (95% CI) with respect to death caused by acute mushroom poisoning. For variables with p < 0.05 in the univariate analysis, we adopted a binary logistic regression analysis to identify the risk factors for death caused by acute mushroom poisoning to establish a predictive model; the diagnostic value was analyzed using receiver operating characteristic (ROC) curves to obtain the ROC area under the curve (AUC), with 95% CI, sensitivity, and specificity. Intermediate values were used to determine the cut-off values, defined as (sensitivity) + (specificity) −1, providing equal weight to sensitivity, specificity, positive and negative predictive values, and accuracy. p < 0.05 was considered to be statistically significant.
Results
General data analysis
Between January 2013 and December 2020, 455 patients with mushroom poisoning were admitted to the AHZMU. The number of patients poisoned increased every year with some fluctuations, resulting in dozens of cases annually. Of the patients admitted, 260 were male and 195 were female, with no significant difference in sex distribution, and a peak incidence of poisoning occurred between the ages of 40 and 70 (Figures 1 and 2). Annual distribution of presentations due to mushroom poisoning at the affiliated hospital of Zunyi Medical University, 2013–2020. Age distribution of mushroom poisoning cases at the affiliated hospital of Zunyi Medical University, 2013–2020.

Time distribution
Mushroom poisoning occurs most frequently during two peaks, in June–July and September–October, which is consistent with previous reports in the literature. The incidence of mushroom poisoning varies depending on the region, climate, and species of mushroom. Accordingly, in Guizhou Province, the clinical onset characteristic of Amanita subpallidorosea is during the peak of September–October (Figure 3). Monthly distribution of presentation for mushroom poisoning cases at the affiliated hospital of Zunyi Medical University, 2013–2020.
Regional distribution
Zunyi City was divided into county units to analyze the incidence of mushroom poisoning. The counties with the highest incidence rates were Zunyi, Tongzi, Wuchuan, Zheng’an, and Yuqing. Similarly, in the vicinity of Tongren District, the county was also taken as the unit area. The distribution of poisoning peak areas, such as Dejiang, Yinjiang, and Yanhe counties, fluctuated every year (Figure 4). Incidence statistics of toxic mushroom poisoning in various counties of Zunyi, 2013–2020.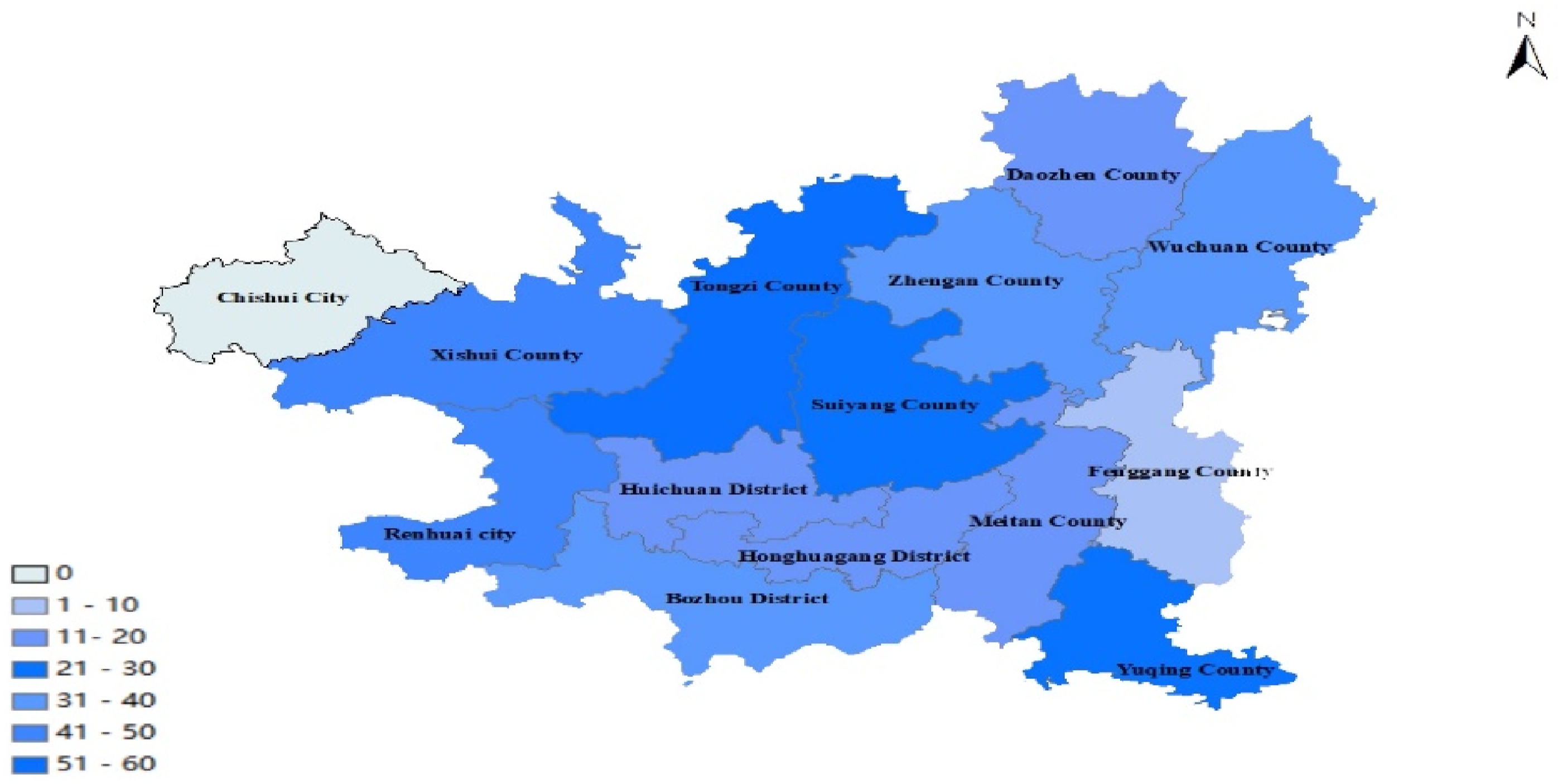
Fatality rate and hospital lengths of stay between first diagnosis (initial diagnosis made at the AHZMU) and non-first diagnosis (initial diagnosis made at an outside facility) groups
The first diagnosis cases at the AHZMU consisted of 126 cases with six deaths, resulting in a case fatality rate of 4.77% and accounting for 12.77% of the total deaths. In contrast, there were 329 Non-first diagnosis cases with 41 deaths, with a case fatality rate of 12.46% and accounting for 87.23% of the total deaths. Furthermore, hospital stays were longer and mortality rates were higher for Non-first diagnosis patients (Figure 5). Fatality rate and hospital lengths of stay between first diagnosis and non-first diagnosis groups.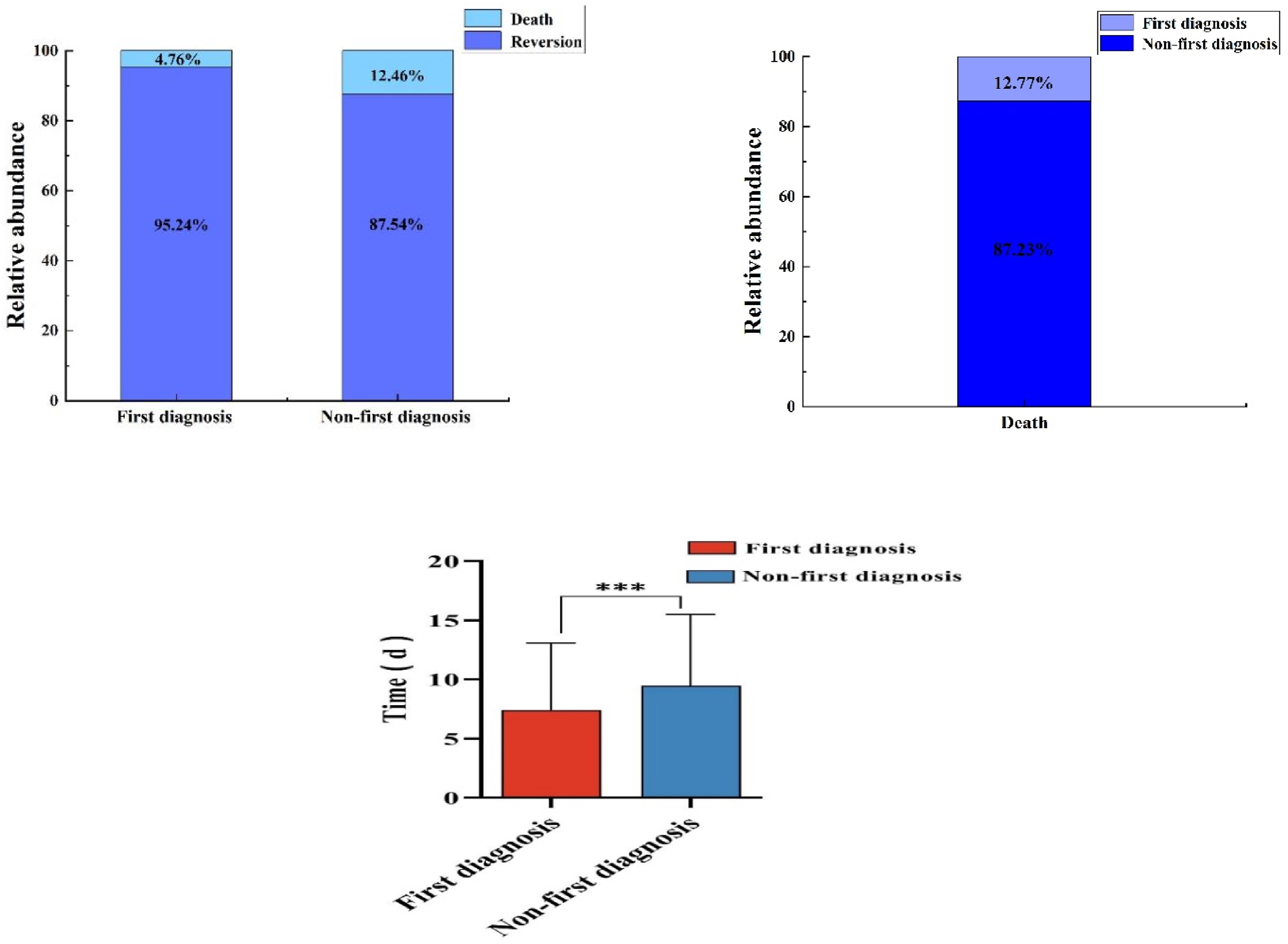
Fatality rate in patients presenting with early (within 6 h of ingestion) versus delayed symptoms (>6 h after ingestion)
In our study, we analyzed 455 cases of mushroom poisoning, of which 164 (36.04%) showed ES. Among these cases, there were 14 deaths resulting in a case fatality rate of 8.54%. In contrast, 291 cases (63.96%) exhibited DS, among which there were 33 deaths, resulting in a case fatality rate of 11.34%. Our findings suggested that the mortality rate was higher in patients who presented with DS (Figure 6). Fatality rates between early symptoms and delayed-symptoms groups.
Fatality rate between blood purification and non-blood purification treatments
Effect of blood purification treatments on acute mushroom poisoning.


Fatality rates in blood purification versus non-blood-purification groups.
Comparison of symptoms in patients presenting with mushroom poisoning who survived versus those who died
Mushrooms have varying types of toxins and toxin components, resulting in diverse clinical symptoms upon poisoning. However, patients present most commonly with gastrointestinal symptoms, followed by abnormalities in the liver, kidneys, myocardium, central nervous system, and the coagulation system. In this retrospective study we analyzed 455 cases of mushroom poisoning and found that in 198 cases (43.51%), hepatogenic injury occurred, resulting in 42 deaths (21.21%). Nephrogenic injuries occurred in 110 cases (24.17%), with five deaths (4.54%). Based on these findings, we concluded that acute hepatogenic injury was the primary cause of death in approximately 89.36% of mushroom poisoning cases (Figures 8 and 9). Patient symptoms characteristic of mushroom poisoning. Symptom characteristics of patients with fatal mushroom poisoning.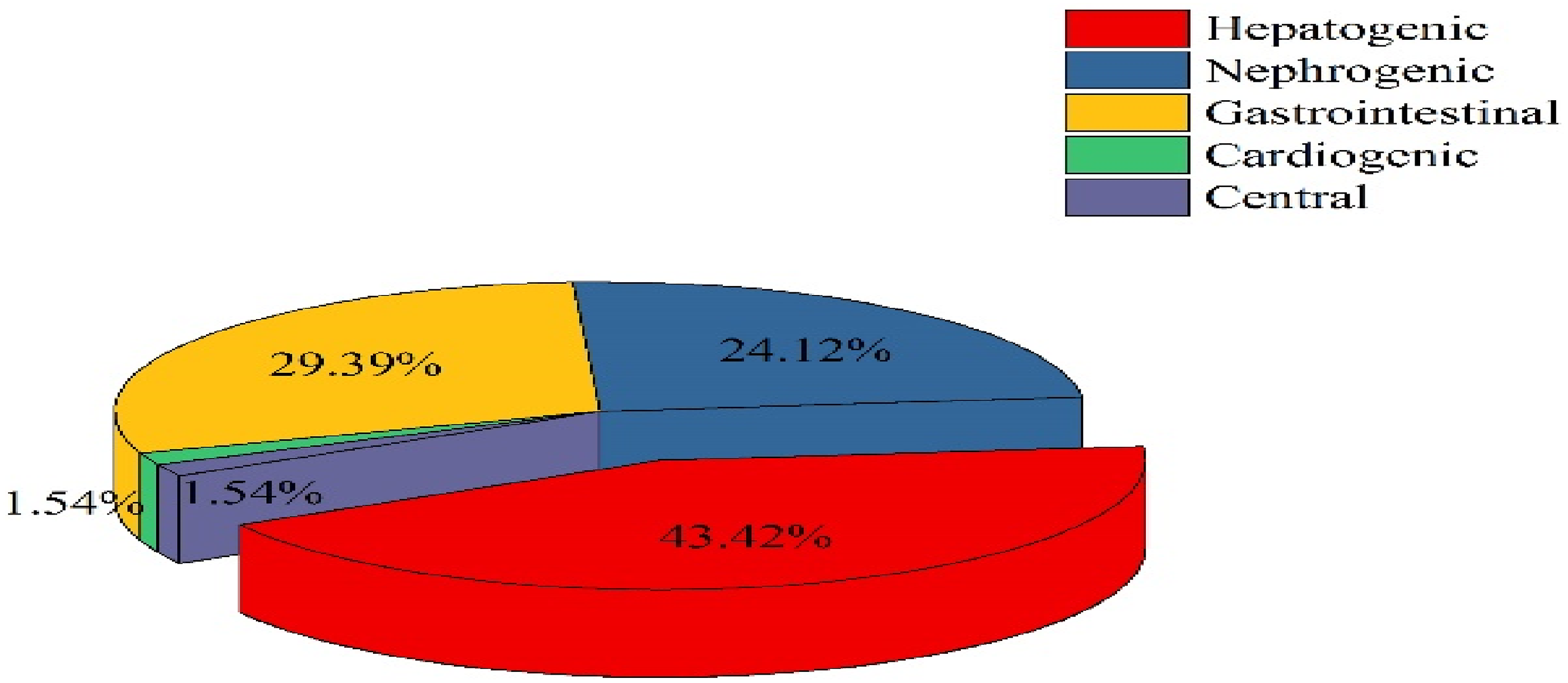

Prediction of risk factors for death in patients with acute mushroom poisoning
Comparison of clinical characteristics in fatal mushroom poisoning.

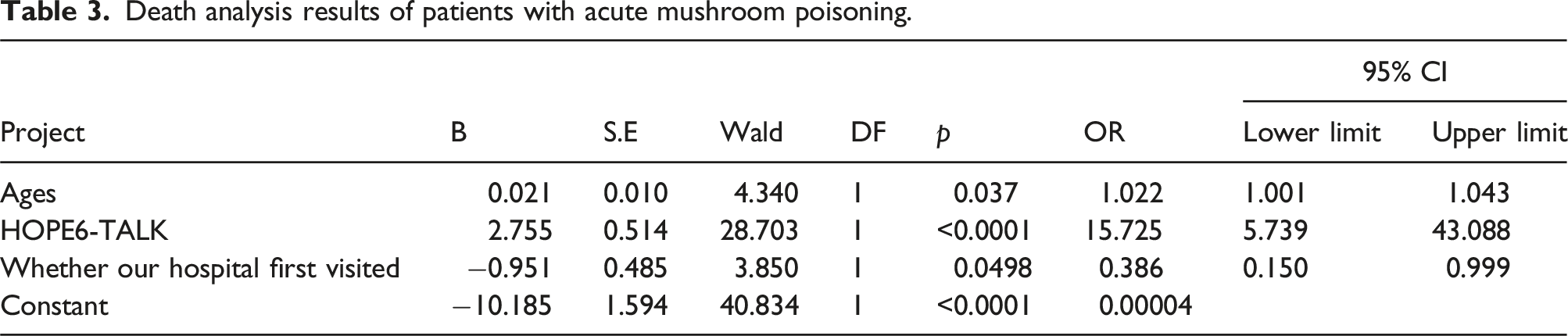
Death analysis results of patients with acute mushroom poisoning.
The calculation formula for Ycoalition was derived by transformation from the above logistic regression equation, Ycoalition = χAge + 82.87χHOPE6; and we calculated the Ycoalition of 455 cases and plotted the ROC curve, as shown in Figure 10. We calculated the measurement values through the ROC curve: age, HOPE6 score, and area under the AUC. Among them, the joint predictive factor AUC was the largest and exhibited a higher predictive effect than other indicators; with the maximal Youden index, an optimal critical value of 289.6, sensitivity of 0.7234, and specificity of 0.7892, the ROC curve analysis showed that the critical value for death caused by acute mushroom poisoning was when the age was 42.5 years, the HOPE6 score was 2.5 points, and the Ycoalition was 289.6 (Table 4 and Figure 10). Multivariable ROC analysis of prognostic factors in amanita phalloides poisoning. Multivariable logistic analysis predictive probability of independent risk factors for the fatality of patients with mushroom poisoning.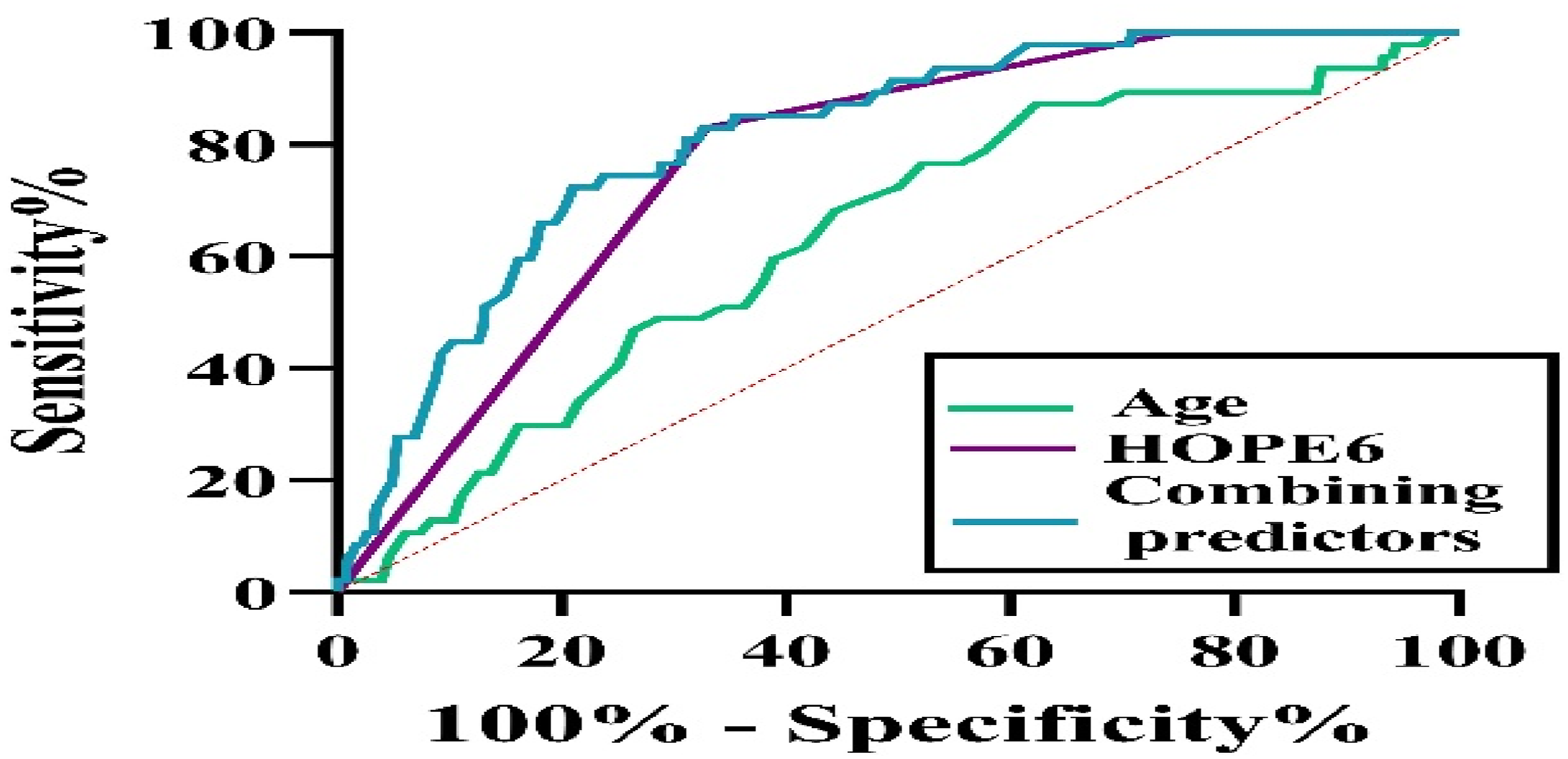

Discussion
The incidence of mushroom poisoning is not uncommon and varies globally, with numerous annual reports of toxic mushroom consumption.9,10 Despite the high incidence of mushroom poisoning in China, there is a lack of public reporting. From 2010 to 2020, the foodborne disease-outbreak monitoring system recorded a total of 10,036 cases of mushroom poisoning. Notably, Yunnan, Hunan, Guizhou comprised 79.7% of total outbreaks, 80.3% of total illnesses, and 74.6% of total deaths. 4 Guizhou Province has a warm and humid climate, making it a suitable environment for mushroom growth during the summer and autumn seasons. However, it is important to note that Amanita accounts for 90% of the mortality rate from various types of mushroom poisoning. The common highly toxic Amanita species found in Guizhou include Amanita pallidorosea, Amanita subpallidorosea, Amanita fuliginea and Galerina sulciceps. Unfortunately, mushroom pickers and consumers in this region often lack the necessary knowledge and experience to properly identify poisonous mushrooms. Moreover, the high mortality rate of mushroom poisoning can be attributed to the low reporting rate of cases, the difficulty in collecting and identifying specimens, and the delay in treatment. To reduce the incidence of mushroom poisoning, it is necessary to promote knowledge about toxic mushrooms and to increase awareness of the dangers thereof. 11
We retrospectively analyzed the clinical data of 455 hospitalized patients with mushroom poisoning admitted to the AHZMU from 2013 to 2020, comprising 260 male and 195 female cases. There was no significant difference in sex distribution in mushroom poisoning patients, and the peak age of poisoning was between 40 and 70 years of age, with the majority of the affected population being agricultural workers. Most patients under 40 years of age worked in non-agricultural jobs, and the incidence age was common among left-behind middle-aged and elderly patients. Based on our review, the highest incidence of mushroom poisoning occurred during the summer and autumn seasons, which aligns with other reports in the literature. The peak periods were observed from June to July and September to October. However, it is important to note that the timing of high incidence periods may vary depending on the region, climate, and species of mushrooms present. A new lethal mushroom species named Amanita subpallidorosea was discovered in Wuchuan County, Guizhou Province in 2014, distributed in the eastern, southern, and southwestern regions of China. The appearance of this mushroom is that of Amanita subpallidoroseaand its peak season is in September to October in Guizhou Province. 12 Each year, several dozen people suffer from mushroom poisoning, often due to mistakenly picking poisonous mushrooms; and this number has been increasing and showing a fluctuating trend. In our study, data from 455 patients were collected, of whom 47 patients died (10.33%), which was a significantly higher mortality rate than currently reported data in China. It is important to note that only inpatient cases were included in this study, and mild outpatient cases were excluded. Of the 455 patients diagnosed at the AHZMU, 126 received first diagnoses whereas 329 were initially diagnosed at other facilities. It was found that patients who did not receive first-time diagnoses at our hospital had longer hospital stays and higher mortality rates compared to those who had first diagnoses. A clinician’s lack of experience in identifying patients with fatal mushroom poisoning may result in missing the optimal treatment period during early incubation and false-recovery stages, ultimately leading to an increased mortality rate.
The clinical characteristics of lethal Amanita mushroom poisoning can be divided into four stages: the incubation period, gastroenteritis period, sham-healing period, and visceral-damage period. The incubation period typically lasts between 6 h and 12 h, with symptoms appearing in some cases after 20 h, which is within 2 h of most other mushroom-poisoning cases; the characteristics of the incubation period are particularly useful in diagnosing Amanita poisoning. In our study, we analyzed 455 cases of mushroom poisoning. Of these cases, 164 patients (36.04%) displayed early symptoms (≤6 h), and 14 of the cases resulted in death (8.54%). The majority of cases, 291 (63.96%), exhibited delayed symptoms (>6 h), with 33 resulting in death. Our findings suggested that mortality rates were higher in cases where patients exhibited delayed symptoms. The most commonly observed clinical manifestation of mushroom poisoning was gastroenteritis. The main factors contributing to death were poisoning leading to liver and kidney function damage, as well as rhabdomyolysis, among others. Approximately 68.13% of the patients experienced symptoms of gastroenteritis, which was associated with a favorable prognosis when limited to a single gastrointestinal symptom. Of the total cases, 156 cases (42.0%) were diagnosed with hepatogenic damage, and 42 cases (21.21%) resulted in fatalities. The highest mortality rate was observed in cases of hepatogenic dysfunction, accounting for 89.36% of the total deaths. Blood purification is a crucial treatment method for severe mushroom poisoning cases, with common techniques such as blood perfusion, plasma exchange, and hemodialysis. With continuous advancements in medical technology, blood-purification treatments have been improving from year to year. For the patients with severe organ injury caused by mushroom poisoning, plasma replacement is the first considered to remove amanita toxin and other harmful substances in the blood, reduce the toxic load and protect important organs. In addition, hemoperfusion is performed with an H330 perfusion device to adsorb toxins and small molecule metabolites from the blood, with the frequency adjusted according to symptoms and laboratory results. When kidney damage is severe and oliguria or anuria occurs, continue renal replacement therapy (CRRT) can not only remove small molecular toxins, but also maintain fluid balance and prevent metabolic disorders. Recent research reports have demonstrated the efficacy of Molecular adsorbent recirculating system (MARS) treatment in this regard. 13
When treating a patient with mushroom poisoning in clinical practice, it is crucial to swiftly conduct morphological and molecular biological identification of the mushrooms. This helps to clarify the poisoning characteristics, makes an accurate clinical diagnosis possible, and initiates prompt and effective treatment.14–16 Moreover, this approach can significantly improve the prognosis of mushroom poisoning cases involving Amanita toxin peptide. While the current clinical classification facilitates determining patient prognosis, it may not be effective for the early diagnosis of mushroom poisoning. Recent studies suggest that grading the severity of the condition using HOPE6 and TALK scores aids in identifying cases of fatal mushroom poisoning. 17 Patients with mushroom poisoning may initially present with gastrointestinal symptoms, but those who are critically ill may develop multiple-organ dysfunction over time. This can result in missed opportunities for diagnosis and treatment. As such, it is recommended that physicians complete the HOPE6 score within 1–2 h of the patient’s admission and perform an initial assessment of patients with suspected mushroom poisoning. The univariate analysis in this study showed that there was a statistically significant difference in three indicators: age, HOPE6 score, and whether our hospital was the first diagnosis. Based on the results of binary logistic regression analysis, these were independent risk factors for death caused by acute mushroom poisoning; however, there is currently no risk prediction model available. We thus aimed to address this gap by constructing a logistic model equation using age and HOPE6 score. In the study, we utilized econometric data to plot the ROC curve and determine the optimal critical value of the combined predictive factor, which was 289.6. Analysis of the ROC curve indicated that the age of 42.5 years, HOPE6 score of 2.5 points, and Ycoalition value of 289.6 were critical values for death caused by acute mushroom poisoning. If a patient’s baseline value was greater than the critical value, their risk of death caused by acute mushroom poisoning was increased. Our study indicated that the HOPE6 and TALK scores were important predictors of mortality in cases of mushroom poisoning. However, incomplete medical records may have impacted the accuracy of our findings. We also observed that when the HOPE6 score exceeded 3, mortality rates tended to be higher. Although the scores may not always provide timely indicators to physicians regarding the severity of the patient’s condition, the correlation between HOPE6 and TALK scores and mortality in mushroom-poisoning patients can still be predicted. This indicated the importance of using these scores in clinical practice to guide the diagnosis and treatment of mushroom poisoning. Additionally, cluster therapy for mushroom poisoning containing Amanita toxin peptide can be carried out based on these scores. We also observed a significant increase in the mortality rate among non-first diagnosis patients in our hospital, which was an independent risk factor for death caused by acute mushroom poisoning. This highlights the lack of awareness among the initial clinician regarding lethal mushrooms, leading to a delayed understanding of the severity of mushroom poisoning and delayed referrals to hospitals equipped to provide effective treatment. Patients experiencing mushroom poisoning should be admitted to a hospital for appropriate treatment. It is also important to promptly calculate the initial HOPE6 score and TALK score, as well as to consult with relevant experts to identify cases of potentially fatal mushroom poisoning. At present, the evaluation of the severity of acute amanitoxin mushroom poisoning patients is mainly directed HOPE6 includes: medical history, organ injury, picture recognition and incubation period greater than 6 h, each item is 1 point, the first doctor must complete within 1 ∼ 2 h after admission, if greater than or equal to 2 points, consider fatal mushroom poisoning; If HOPE6 score is less than 2, TALK score should be completed again within 12 ∼ 24 h, which includes: toxic detection is clear as fatal toxin type, coagulation dysfunction, liver dysfunction and renal dysfunction, each score is 1 point, if greater than or equal to 1 point consider fatal mushroom poisoning. 17
Incidence statistics of toxic mushroom poisoning in various counties of Zunyi, 2013–2020.

Incidence statistics of toxic mushroom poisoning in various counties of Zunyi, 2013–2020.

Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was financially supported by National Natural Science Foundation of China (82460385); Guizhou Provincial Basic Research Program-ZK [2023] General 579; The Zunyi Municipal Bureau of Science, Technology, and Big Data--Zunyi Scienific and Technological Program-HZ (2022) 242; Peking Union Medical Foundation Rui Yi Emergency Medicine Research Foundation (22322012022).