
Abstract
Background
Acneiform eruption is a dermatological condition resembling acne vulgaris, with a similar clinical presentation that is often difficult to differentiate. Several medications like corticosteroids, anti-convulsants, anti-psychotics, anti-depressants, vitamin B12, and testosterone have all been linked to acneiform outbreaks. This case highlights the need for awareness of potential drug-induced dermatological side effects in the management of postpartum psychosis.
Case Presentation
A 3-month postpartum psychosis female patient, around 30 years old, was admitted to the psychiatric department and treated with tablet Olanzapine and Clonazepam, but later developed new complaints of pain in the lower limbs and a burning sensation over the foot, and thus was treated with injection vitamin B complex. Within 30 min of receiving vitamin B complex, she developed cutaneous eruptions without comedones. A dermatological examination revealed a papulopustular eruption over her hand, neck, and face. Based on the subjective findings, the patient was diagnosed with vitamin B complex acneiform eruption. The treatment options start with discontinuing the offending medication, vitamin B complex. They were treated with tablet Ebastine 20 mg hora somni (HS), tablet Prednisolone 10 mg/day, and topical salicylic acid for a month, and gradually, the condition resolved.
Conclusion
This report highlights a rare dermatological adverse event in a postpartum psychosis patient on vitamin B complex and Olanzapine. The sudden onset of acneiform eruptions underscores the importance of recognizing potential drug interactions and their dermatological manifestations, especially in postpartum patients, who may already be vulnerable to various physiological changes.
Introduction
Acneiform eruption is a dermatological problem, similar to acne vulgaris, where the clinical presentation is identical and difficult to differentiate. 1 A 30-year-old postpartum patient receiving psychotropic medication developed acneiform eruptions, raising concerns about drug-induced dermatological reactions. Acne vulgaris features comedones, while acneiform eruptions are clinically distinguished by the absence of comedones.2, 3 Some characteristics of acneiform eruptions are as follows: (a) they typically affect adults; (b) the onset is often acute and characterized by papules and pustules that may involve the face, neck, shoulders, chest, and upper back; (c) comedones and cysts are usually absent; (d) the eruption may be accompanied by more or less severe pruritus; (e) the remission is spontaneous and complete after discontinuation of the responsible medication; however, the length of remission is determined by the rate of drug clearance; (f) no scar formation; and (g) no relapses.4–6 Postpartum psychosis is a rare but severe mental health illness that can happen suddenly in the days or weeks after birth and is typically associated with symptoms like hallucinations, delusions, disorganized thinking, and mood disorders. In the treatment of postpartum psychosis, anti-psychotic medications are often used; however, these can have adverse dermatologic effects. 7
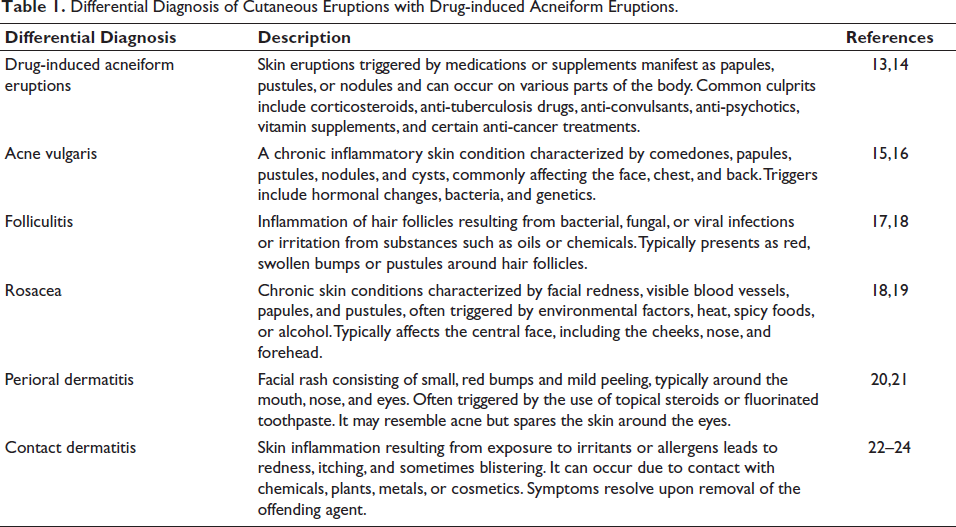
Several medications like corticosteroids, epidermal growth factor receptor (EFGR) inhibitors, cyclosporine, anti-convulsants, anti-psychotics, anti-depressants, tumor necrosis factor-alpha (TNF-α) inhibitors, anabolic steroids, danazol, anti-tubercular drugs, quinidine, azathioprine, and testosterone have all been linked to acneiform outbreaks.8–10 Certain literature supports the claims of dietary supplements linked to acneiform eruptions. The literature reviews revealed that the prevalence of acneiform eruptions is drastically higher with vitamin B12 when compared to other medications. Vitamin B12 is linked to acneiform eruptions due to its ability to modulate skin flora and immunological response. 11 Olanzapine and other anti-psychotics have also been reported to induce dermatological reactions, even though these problems appear less frequently. 12 In dermatological disorders, it is crucial to consider a range of conditions, including drug-induced acneiform eruptions, when evaluating patients presenting with cutaneous manifestations. Table 1 provides a comprehensive overview of the key differential diagnoses to consider alongside drug-induced acneiform eruptions.
Differential Diagnosis of Cutaneous Eruptions with Drug-induced Acneiform Eruptions.
In this report, we present a case of an acneiform eruption in a 3-month postpartum female patient with psychosis, likely induced by the administration of vitamin B12 and Olanzapine. This case highlights the need for awareness of potential drug-induced dermatological side effects in the management of postpartum psychosis.
Case Report
A 3-month postpartum female patient, around 30 years old, was admitted to the psychiatric department with the chief complaints of irrelevant talk, sleep disturbance, talking to herself, and restlessness for 3 days, and was diagnosed with postpartum psychosis. She was treated with tablet Olanzapine 5 mg BD and tablet Clonazepam 0.5 mg hora somni (HS), but later developed a new complaint of pain in the lower limbs and a burning sensation over the foot, and thus were treated with injection vitamin B complex 2 cc (Mecobalamine IP 1,000 mcg, Pyridoxine hydrochloride IP 100 mg, Nicotinamide IP 100 mg, Benzyl alcohol IP 2% w/v) as a STAT order via intramuscular injection on the 5th day of admission. Thirty minutes after receiving an intramuscular injection of vitamin B complex, the patient developed papulopustular lesions without comedones. A dermatological examination revealed papulopustular lesions on her hand, neck, and face, as shown in Figure 1. On examination, the patient’s vitals, systemic assessment, and physical examination findings were all within normal limits. The patient’s complete blood count, routine biochemistry, including hepatic and renal function tests, and erythrocyte sedimentation rate, fall within normal limits. Based on the subjective findings, the patient was diagnosed with vitamin B complex-induced acneiform eruption. The treatment options start with discontinuing the offending medication, vitamin B complex. She was treated with tablet Ebastine 20 mg HS, tablet Prednisolone 10 mg/day, and topical salicylic acid for a month. After a week of therapeutic intervention, the patient’s condition gradually resolved, supporting the success of the administered medication. Many studies report that tablet Olanzapine is also responsible for causing acneiform eruptions, but in this case, the eruption happened because of the synergistic activities of vitamin B complex and Olanzapine. The patient was suffering from psychosis, and hence systemic isotretinoin was not suggested, as it may aggravate suicidal thoughts when combined with Olanzapine. So, Olanzapine was continued as monotherapy to treat postpartum psychosis by discontinuing the vitamin B complex. After a month of treatment, the patient was prescribed a tablet of vitamin B complex under observation and has not resumed having the acneiform outbreaks. The adverse event associated with drug-induced acneiform eruptions in this case report depicts a score of five, indicating a probable adverse event according to Naranjo’s Causality Assessment Scale.
Clinical Manifestation on Face and Upper Limb.

Discussion
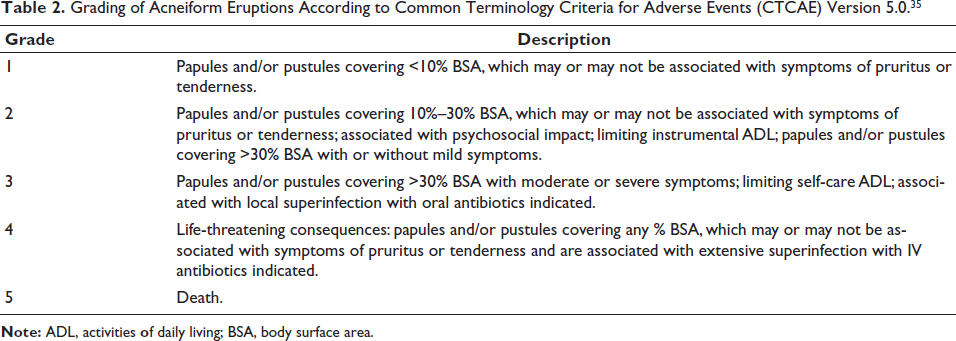
The first vitamin B12-induced acneiform eruption was reported in 1958 by Jadassohn. 25 Consequently, this eruption is considered to be rare. It was proposed that prolonged vitamin B12 medication, 26 or high daily doses, 27 of the vitamin may have contributed to these eruptions. In the past, this vitamin was mostly utilized during pregnancy; adult (or older) women were shown to be more susceptible to vitamin B complex-induced eruptions. 28 This patient has also undergone tablet Olanzapine 10 mg/day for psychosis, and some literature supports Olanzapine-induced acneiform eruption.29–32 In this case, there was no skin eruption while starting Olanzapine on the 1st day, but on the 3rd day of treatment, an injection of vitamin supplement (methylcobalamin, Pyridoxine, Nicotinamide) was given as STAT, and then within half an hour, she developed skin eruptions over her hand. Although vitamin B complex was identified as the primary trigger, Olanzapine has also been associated with acneiform eruptions in some cases, warranting further investigation. The literature report suggests that B vitamins, including B3, B6, and B12, cause acneiform eruptions, but in this case, the patient was administered vitamin B complex along with Olanzapine. The synergistic activity of these medications is suspected for the acneiform eruptions.33, 34 The activity of vitamin B3-induced acneiform eruptions is quite interesting because it, when taken orally or intravenously, may cause skin eruptions, but, when taken orally, can treat skin eruptions. 35 Table 2 provides the grading of acneiform eruptions.
Grading of Acneiform Eruptions According to Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. 35
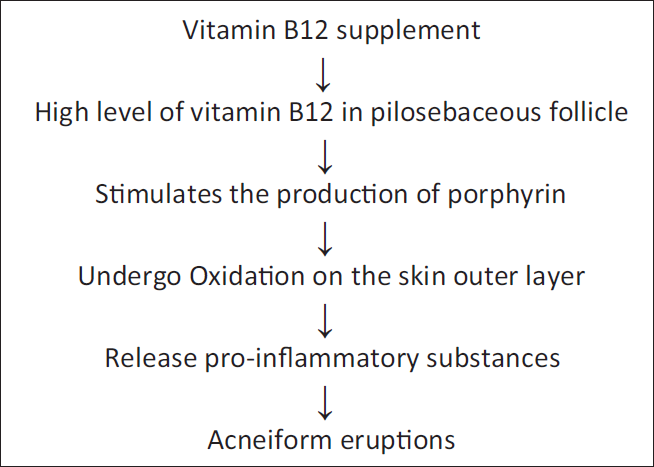
The exact mechanism of disease occurrence is not well established with other medicines, but the vitamin B12 mechanism alone is explained (Figure 2). The Propionibacterium acnes colonies are located in the pilosebaceous follicle in the skin. The high level of vitamin B12 causes transcriptome change in Propionibacterium acnes and fosters the production of porphyrin, which undergoes oxidation on the surface of the skin, resulting in the release of proinflammatory mediators that simultaneously commence acneiform eruptions.36, 37 Olanzapine, an atypical anti-psychotic, has been reported to alter hormonal levels, particularly by increasing prolactin secretion, and may modulate immune responses. These changes could potentially enhance the effect of vitamin B12 on skin microbiota, leading to acneiform eruptions. Further research is required to explore possible drug interactions between Olanzapine and vitamin B complex in dermatological conditions.
Pathophysiology of Vitamin B12-induced Acneiform Eruptions.
Based on the clinical findings and drug history, our patient was diagnosed with either Olanzapine or vitamin B complex-induced acneiform eruptions. There was no necessity for a histopathologic investigation in this case. In many cases of drug-induced acne, the eruption is clinically and histologically comparable to acne vulgaris. As a result, histological testing is not required in all situations, as it was in ours. For the diagnosis of drug-induced acne, a comprehensive medical history and physical examination are more valuable than a histopathologic investigation. Intrafollicular inflammation, nuclear dust in the follicular lumen, and an irregular patterns of keratin plugging support the diagnosis of acneiform eruptions. 38
Therapeutic Interventions
The first and foremost treatment option is to cease exposure if organisms or drugs cause acneiform outbreaks; the lesions often go away in 2–3 weeks, though they may reappear once it is resumed.37, 39 Avoiding mechanical and occupational acne can be achieved by reducing contact or friction. 40 The treatment option for acneiform eruptions depends on the etiologic factors. 41 Skin cleaners like benzoyl peroxide or salicylic acid may be recommended to minimize greasy skin, but the conventional treatments for acne vulgaris rarely work on people with acneiform outbreaks. 42 If eruptions occur by EFGR inhibitors, dapsone exerts the desired pharmacological action. 42 The most effective preventative treatment for acneiform eruption is oral tetracycline antibiotics; however, improvement with Azithromycin was grim.43, 44 The review conducted by Bierbrier et al. concluded that systemic retinoids are a safe and effective therapy for acneiform eruptions when compared to topical administration.40, 45
Genetic Testing
A skin deoxyribonucleic acid (DNA) test is a precise test to validate the genetic mutations of the skin and helps to analyze the risk of allergies, inflammations, tone, photosensitivity, texture, skin aging, skin tone, and oxidative stress, along with the requirements of nutritional supplements for healthy skin.46–49 The systematic review and meta-analysis conducted by Heng concluded that the TNF-α-308 gene is responsible for altering the inflammatory responses, and the CYP17A1 and FST are responsible for altering the activity and functions of sebaceous glands.50, 51 The mutation in heterozygous CYP21A2 has contributed to the clinical manifestation, reported in a study conducted by Gao et al. 52
Comparative Insights from Literature
There are currently no specific studies addressing vitamin B-induced acneiform eruptions in postpartum patients. Drawing parallels with similar case reports and clinical studies provides invaluable insights into the spectrum of drug-induced acneiform eruptions and their management. For instance, Sutar and Ganjekar 33 reported a comparable case of a postpartum patient developing acneiform eruptions following Olanzapine, highlighting the significance of recognizing and addressing drug interactions in this vulnerable population. Furthermore, Gouda et al.53, 54 documented a series of cases wherein Olanzapine therapy was associated with dermatological adverse events, emphasizing the need for vigilant monitoring and tailored interventions in psychiatric patients. By contrasting our findings with these studies, we underscore the broader implications for clinical practice and patient care in diverse medical settings.
Limitations of the Study
This study has certain limitations. The patient received a combination of vitamin B3, B6, and B12, making it difficult to determine whether vitamin B12 alone was the main trigger for the eruption. Additionally, the potential contribution of Olanzapine to acneiform eruptions remains uncertain and requires further studies with a larger sample size.
Conclusion
This case report sheds light on a rare but significant adverse dermatological event in a postpartum psychosis patient treated with vitamin B complex and Olanzapine. The sudden onset of acneiform eruptions underscores the importance of recognizing potential drug interactions and their dermatological manifestations, especially in postpartum patients who may already be vulnerable to various physiological changes. By documenting this case, we aim to enhance clinical awareness and encourage more focused research on the dermatological impacts of psychotropic and vitamin therapies, ultimately contributing to improved patient care and outcomes in similar clinical scenarios.
Footnotes
Abbreviations
EGFR: Epidermal growth factor receptor; NCC-PvPI: National Coordination Centre—Pharmacovigilance Program of India; TNF-α: Tumor necrosis factor-alpha.
Acknowledgments
The authors would like express their sincere gratitude to the patient and their family members. The authors also acknowledge and thank the logistic and technical support provided by the Pharmacovigilance Programme of India (PvPI), Indian Pharmacopoeia Commission, Ghaziabad, India; JSS College of Pharmacy, JSS Academy of Higher Education & Research, Ooty, Nilgiris, Tamil Nadu, India; and the Karpagam Faculty of Medical Sciences & Research, for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Duly signed informed consent has been obtained from the patient for publication of clinical details and images, wherever applicable. No objection certificate was obtained from the Karpagam Hospital for the purpose of journal submission and publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
Informed Consent
Informed consent was obtained from the patient, NCC-PvPI and Karpagam Faculty of Medical Sciences and Research.