
Abstract
Background
Vitamin D deficiency poses significant health risks globally, impacting bone health and immune function. In Saudi Arabia, where environmental and lifestyle factors limit sun exposure, vitamin D deficiency is especially prevalent. This study assesses vitamin D deficiency in Al-Madinah, focusing on differences between Saudi nationals and non-Saudi residents.
Objectives
The primary aim was to determine the prevalence of vitamin D deficiency among Saudis and non-Saudis and identify lifestyle and dietary factors contributing to deficiency.
Materials and Methods
Conducted from October 2017 to May 2018, this cross-sectional study included 65 non-diabetic male participants aged 18–65, divided into two groups: Saudi (n = 33) and non-Saudi (n = 32). Exclusion criteria included conditions affecting vitamin D metabolism. Data were collected on demographics, dietary habits, sun exposure, and anthropometric measurements. Serum 25-hydroxyvitamin D levels were measured, and logistic regression was used to identify predictors of deficiency.
Results
Vitamin D deficiency was significantly higher in Saudis (91%) than in non-Saudis (47%). Limited sun exposure, lower intake of vitamin D-rich foods, and occupation type were associated with higher deficiency rates among Saudis. Logistic regression revealed that occupation was a positive predictor, while liver consumption was a negative predictor of deficiency.
Conclusion
This study highlights the urgent need for targeted public health interventions in Saudi Arabia to address vitamin D deficiency, recommending dietary changes and vitamin D supplementation. Further research should investigate genetic and environmental factors affecting vitamin D levels across different populations in the region.
Background
Vitamin D is one of the vitamins that are soluble in fat. It is also classified as a prohormone steroid. 1 Vitamin D has important functions in the endocrine, paracrine, and autocrine systems, as so, it is regarded as the “sunshine” vitamin.2, 3 Naturally, only two forms of vitamin D are available: vitamin D2, also known as ergocalciferol, and vitamin D3 (cholecalciferol). Photosynthesis of vitamin D in the skin by the induction of sunlight produces only cholecalciferol, while the dietary sources of vitamin D can provide the vitamin in the two forms. 3
Globally, vitamin D deficiency is among the major public health issues.4, 5 The deficiency in vitamin D in children leads to a disease called rickets, in which bone tissue fails to mineralize properly, causing skeletal deformities and brittle bones. While the deficiency in vitamin D in adults leads to weakness in the muscles and consequently, increasing the risk of falls and fractures. In adults, vitamin D deficiency causes another disease called osteomalacia, leading to the weakness of bones and exacerbating osteoporosis.1, 6–8
Numerous data have been documented on the link between ethnicity, the color of skin, and vitamin D serum levels. In the United States, 90% or more of the non-Hispanic African Americans were found to have vitamin D levels around 15 ng/mL, the mean vitamin D level of Hispanics was 20 ng/mL, while that of the non-Hispanic Whites was 26 ng/mL, whereas those individuals residing the traditional counties in Central Africa were shown to have mean plasma 25(OH) D levels of about 46 ng/mL.9–11
In the Middle East and North Africa (MENA), especially the Kingdom of Saudi Arabia (KSA), a high prevalence of vitamin D deficiency has been reported despite the abundance of sunshine.12, 13 In 2015, a cross-sectional national multistage survey reported that the prevalence of vitamin D deficiency was 40.6% in male Saudis and 62.65% in female Saudis. 14 Similar results were found in other studies that were conducted in various places in KSA. Two studies that were conducted in Riyadh indicated that vitamin D deficiency among Saudi men was 87.8%, 15 and 78.1% in Saudi females and 72.4% in Saudi males, respectively. 16 In Damam, the prevalence of vitamin D deficiency was found to be greater than 65%. 17 Furthermore, Dabbour et al. conducted in Makkah estimated that vitamin D levels were very low among the healthy Saudi population (5.26 ± 2.59 ng/mL). 4
Objectives
To the best of our knowledge, this is the first study to directly compare the prevalence of vitamin D deficiency between these two populations: Saudis and non-Saudis living in the same area. This addresses a significant gap in understanding how regional and lifestyle factors influence deficiency rates by directly comparing vitamin D deficiency between Saudi and non-Saudi populations residing in the same region, Al-Madinah Al-Munawwarah.
This will be the first study to document vitamin D status in Al-Madinah Al-Munawwarah. Also, this article will examine predictors of such deficiency.
Methods
Subjects and Study Design
This was a cross-sectional study conducted in Al-Madinah Al-Munawwarah, KSA, from October 2017 to May 2018. This period of 8 months was chosen to reduce seasonality bias as June, July, August, and September are the hottest summer months in KSA.
Non-diabetic male Saudis and non-Saudis nationalities aged between 18 and 65 years old who attended the Medical Unit, Taibah University were included in this study. Participants were excluded from the study if they consumed vitamin D supplementations, were diagnosed with renal, liver or cancer, thyroid or parathyroid diseases, and received any drug interacting with vitamin D, such as steroids, orlistat, cholestyramine, phenytoin, and phenobarbital. Based on the sample size calculation, a sample size of 65 encounters per study arm, 33 in group one (Saudis) and 32 in group two (non-Saudis), would detect the degree of difference with 80% power at α = .05.
Prior to participants’ enrollment commenced, demographic data, a detailed history of diabetes (if present), socio-economic data, information about intake of vitamin D-containing diets, and exposure period to sunlight per day were collected. Completion and return of written informed consent before participating in the study indicated voluntary agreement to participate in this study.
Data Collection
Anthropometric Data
The weight was measured in kilograms and rounded to the nearest 100 g. A standard beam scale was used to measure the weight of participants. The participants weighed wearing light clothes and barefoot.
A calibrated height board was attached to the scale to measure the height in centimeters. Weight in kilograms was divided by the square of height in meters to calculate the body mass index (BMI). The BMI was used to evaluate obesity. Participants with a BMI between 25 and 29.9 kg/m2 were considered overweight, and participants with a BMI between 30 and 39.9 kg/m2 were considered obese participants. When BMI was found to be >40 kg/m2, then they were considered morbidly obese. Determination of the waist circumference was done by measuring the broadest area between the edge of the lower ribs and the iliac crest.
Blood Sample Collection and Laboratory Analysis
Five milliliters of blood were collected by trained technicians. This was done under the supervision and guidance of the primary care physicians. Blood tubes were preserved in a cooler or refrigerator immediately. The time of preservation was not less than 30 min and did not exceed 4 h before the technicians centrifuged them. The centrifugation process was done for about half an hour at 3,000 RPM at 4°C. Following that, the technicians immediately separated the serum from the whole blood and froze them at –20°C. This was done at the biochemistry laboratory at the Medical Unit, Faculty of Medicine, Taibah University, Al-Madinah.
The 25-hydroxyvitamin D levels were measured by electrochemiluminescence immunoassay (ECLIA) assay by cobas machine e 411. The levels were considered deficient (<20 ng/mL), inadequate (20–30 ng/mL), and adequate (30 ng/mL) as recommended by the American Endocrine Society Clinical Practice Guidelines.2, 18
Results
Data analysis was conducted using Statistical Package for the Social Sciences (SPSS) version 25.0 (IBM Corp., Armonk, NY, USA).
A total of 65 healthy participants were recruited in the study, subdivided into two groups: 33 Saudis and 32 non-Saudis. The sample size was estimated to provide 80% power to detect a difference in vitamin D deficiency between the two groups at a two-sided 0.05 significance level. The mean age of the Saudi group was 33.6 ± 7.2 years, and the median and mode were found to be 32 years, while the mean age of the non-Saudi group was 46.8 ± 8.1 years, with a median 45.5 and mode 43 years, respectively.
The Marital Status
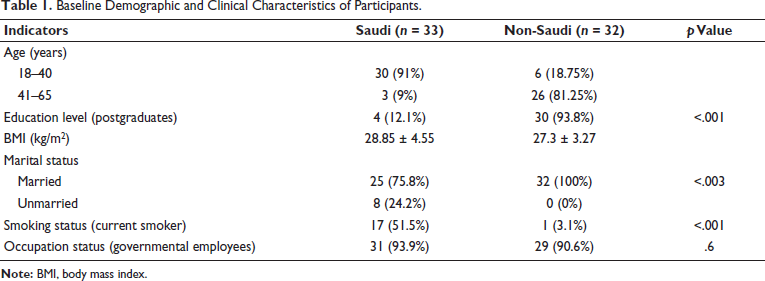
All the non-Saudi groups were married (100%) versus only 75.8% (n = 25) of the Saudi group were married. A significant difference was found between the two groups in their marital status (Table 1).
Baseline Demographic and Clinical Characteristics of Participants.
Smoking Status
The results of the present study showed that a high percentage of the Saudi participants were current and active smokers (n = 17, 51.5%) compared to the non-Saudi participants (n = 1, 3.1%). Statistical analysis showed that there is a significant variation in the smoking status between Saudi and non-Saudi participants (p < .001).
Education Status
The majority of the non-Saudi participants were postgraduates (n = 30, 93.8%), while only 12.1% (n = 3) in the Saudi group were postgraduates. Therefore, a significant variation was detected between the two groups in their education status (p < .001) (Table 1).
Occupation Status
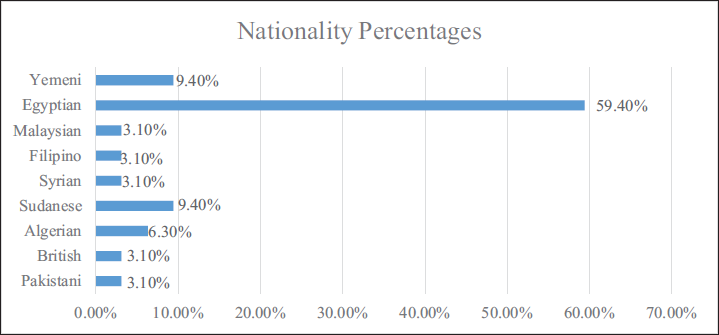
The majority of both groups were governmental employees, individuals working in public sector institutions under the Saudi government, including administrative, educational, and healthcare sectors, that is, 93.9% (n = 31) Saudi and 90.6% (n = 29) non-Saudi, while only 6.2% (n = 2) of Saudi and non-Saudi participants were students. Besides that, 3.1% (n = 1) of the non-Saudi group were without a job. However, the occupation status did not differ significantly between the two groups (p = .6). The majority of the non-Saudi participants were Egyptians (n = 19, 59.40%), followed by the Sudanese and Yemenis, 9.40% (n = 3) each, as shown in Figure 1.
Nationalities of the Non-Saudi Participants (n = 32).
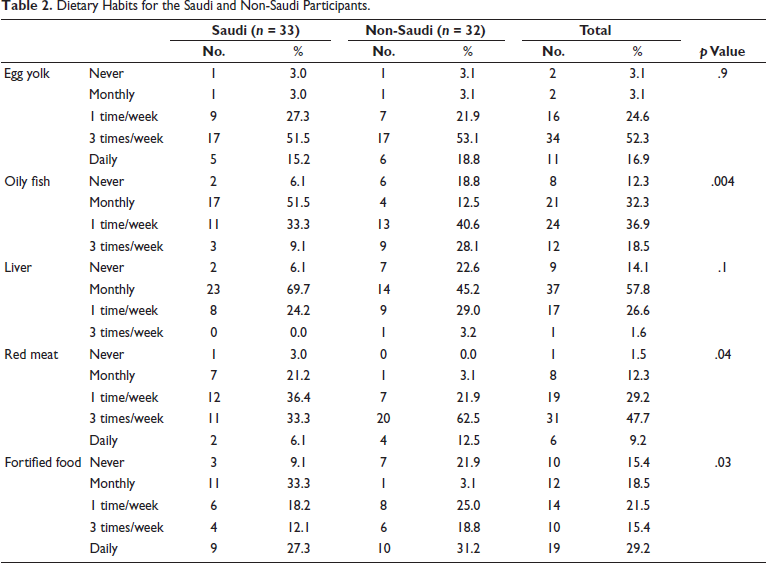
Results of this present study showed that egg yolk consumption in both groups was almost the same (51.5% vs. 53.1%, 3 times/week, 3% vs. 3.1% monthly, 15.2% vs. 18.8% daily).
The statistical analysis of oily fish consumption showed that the non-Saudi population consumed more significantly than the Saudi population did. There was not much difference between the two groups regarding liver intake, but the ingestion of both red meat and fortified food was significantly lower among the Saudi population compared with the non-Saudi (Table 2).
Dietary Habits for the Saudi and Non-Saudi Participants.
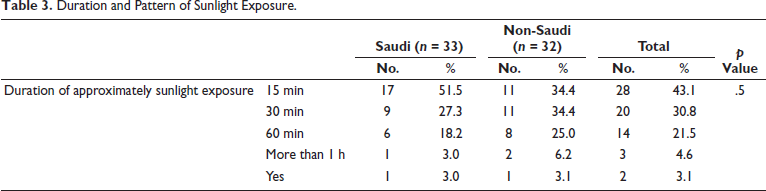
In the Saudi nationality group, it was observed that 27.3% were exposed to sunlight 15 min daily compared to 34.4% in the non-Saudi group, while 18.2% of the Saudi nationality group were exposed to sunlight 60 min daily versus 25% in the non-Saudi group.
Noteworthy, the positive exposure to sunlight in this study was defined as the direct exposure (not indoors via windows) of at least some uncovered body parts, such as the arms and some parts of the legs, during the time period between 10 am and 3 pm for not less than 5 min (Table 3).
Duration and Pattern of Sunlight Exposure.
The occupation status was found to be positively correlated with vitamin D deficiency, while the consumption of liver was observed to be negatively correlated with vitamin D deficiency among the Saudi population, as revealed by logistic regression.
Vitamin D Levels
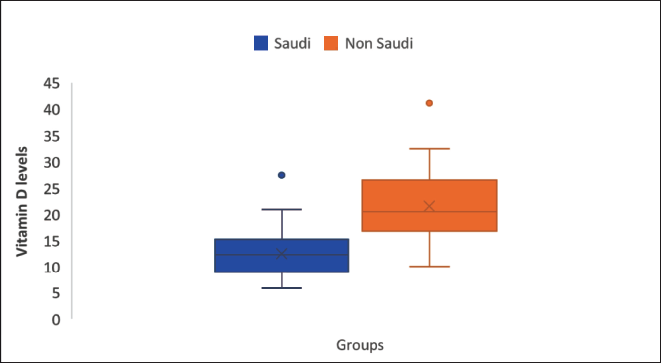
A significant percentage of the participants in the Saudi group (n = 30, 91%) suffered from a deficiency in vitamin D levels [25 (OH) D < 20 ng/mL] 12.57 ± 4.82 [Mean ± Standard Deviation (SD)], compared to only 47% (n = 15) in the non-Saudi group [21.56 ± 6.82 (Mean ± SD)]. Vitamin D deficiency was found to be significantly higher in the Saudi group than in the non-Saudi group, with p = .001 (Figure 2).
Box and Whisker Plots Showing Vitamin D Levels.
Discussion
This study explored the prevalence of vitamin D deficiency among Saudi and non-Saudi populations in Al-Madinah Al-Munawwarah, examining sociodemographic factors, dietary habits, and lifestyle patterns. The findings contribute to understanding the drivers of vitamin D deficiency and highlight the differences between the two groups.
Anthropometric and Sociodemographic Features
Age
Non-Saudis were predominantly older due to postgraduate education and work experience requirements, while Saudis, engaged mostly in administrative jobs, were younger. This aligns with studies such as Naugler et al., 19 which found vitamin D deficiency less prevalent in older age groups. However, urbanization and dietary westernization in Saudi Arabia have contributed to deficiency across all age groups.19–22
BMI
Saudi participants had higher BMI than non-Saudis, with no statistically significant difference noted. This finding aligns with Alqarni, who observed rising obesity rates in Saudi Arabia due to high-carbohydrate diets and low physical activity.23–25 Obesity negatively impacts vitamin D levels due to sequestration in fat tissues, as noted by Al-Daghri et al. and Bettencourt et al.26–29 Increased catabolism of vitamin D in fat tissues further exacerbates deficiency, and Chakhtoura et al. recommended higher vitamin D supplementation doses for obese individuals to address reduced bioavailability. 13
Sociodemographic Factors
Marital Status
Non-Saudis were more likely to be married, consuming healthier diets that positively impacted vitamin D levels. Single participants tended to rely on fast foods, typically low in vitamin D content.
Education
A significant proportion of non-Saudis held postgraduate degrees (93.85%), compared to 12.1% of Saudis. Higher education correlated with greater awareness of vitamin D’s health benefits, as shown in previous studies.12, 19 This awareness likely contributed to better dietary practices and vitamin D levels among non-Saudis.
Smoking
Smoking rates were higher among Saudis, consistent with Al-Nozha et al., 30 who reported high smoking prevalence in urban areas. Smoking adversely affects vitamin D levels, as noted in studies by Mulligan et al. 31
Dietary Habits
Oily Fish
Non-Saudis consumed significantly more oily fish, a key source of omega-3 fatty acids and vitamin D, than Saudis (p = .004). Cultural preferences and lack of nutritional education contributed to poor fish consumption among Saudis. 32
Red Meat
Non-Saudis also consumed more red meat (p = .04), which is a moderate source of vitamin D. Traditional Saudi diets, rich in carbohydrates and low in fat, coupled with urbanization, have led to increased reliance on fast foods. This aligns with findings from Moradi-Lakeh et al. on dietary patterns in Saudi Arabia. 33
Fortified Foods
Non-Saudis consumed more fortified foods, such as vitamin D-enriched milk, orange juice, and cereals, likely due to greater awareness and cultural dietary habits. In contrast, Saudis had lower intake, consistent with Al-Daghri’s findings on poor fortified food consumption in Saudi populations. This may be influenced by limited public health campaigns, traditional dietary preferences, and gaps in food fortification policies. Increasing awareness and accessibility of fortified foods could help address vitamin D deficiency among Saudis. 20
Egg Yolk and Liver
Both groups showed limited consumption of egg yolk and liver despite their vitamin D content. Urbanized dietary habits and increased consumption of processed foods were contributing factors.
Vitamin D Deficiency Prevalence
Vitamin D deficiency was significantly higher among Saudis (91%) compared to non-Saudis (47%). The mean serum levels for Saudis (12.57 ± 4.82 ng/mL) were notably lower than those for non-Saudis (21.56 ± 6.82 ng/mL) (p = .001). Logistic regression identified office-bound jobs and poor liver consumption as key predictors of deficiency. These findings align with Ardawi et al. (2012), who noted poor sunlight exposure and other factors contributing to deficiency among Saudis.34, 35
Factors Influencing Deficiency
Sunlight Exposure
Both groups had poor sunlight exposure, with less than 20% exposed for 1 h daily. Factors such as extreme heat, indoor lifestyles, and cultural clothing limited Saudis’ sun exposure. Studies like Ardawi et al. supports these findings.34, 35
Obesity and Type 2 Diabetes Mellitus (T2DM)
Saudis showed higher rates of obesity and overweight, which correlated with lower vitamin D levels. Obesity and vitamin D deficiency were identified as potential indicators for T2DM. Studies by Bani-Issa et al. found similar associations in Middle Eastern populations. 12
Genetic Factors
High consanguinity rates among Saudis may contribute to genetic mutations affecting vitamin D metabolism, such as calcium-sensing receptor gene polymorphisms (33). Darker skin pigmentation, which reduces ultraviolet B (UVB) absorption, and cultural clothing further compounded the deficiency. Although genetic factors and high consanguinity rates may contribute to vitamin D metabolism differences, this study did not directly investigate these aspects. Future research should explore these potential influences.
Comparison with Regional Studies
The findings corroborate previous studies on vitamin D deficiency in Saudi Arabia. Al-Daghri reported 81% deficiency in Saudis, linking it to various comorbidities, including obesity and diabetes. Studies in Riyadh, Makkah, and other regions showed similar prevalence rates, though this study is unique in comparing Saudi and non-Saudi populations and evaluating dietary influences on deficiency.4, 16, 34
Conclusion
Vitamin D deficiency was significantly higher in the Saudi population than in the non-Saudi population. The occupation status was found to be the only factor positively correlated with vitamin D deficiency.
Early screening for vitamin D serum levels is recommended for the Saudi population, and rapid correction of vitamin D deficiency with vitamin D supplements should be considered.
The study highlights the urgent need for public health interventions, including targeted education programs and food fortification strategies, to address vitamin D deficiency in Saudi populations.
Limitations
The multi-center study might have provided more generalizable results.
Footnotes
Acknowledgments
The authors would like to thank Dr. Sherif Monir for his advice on statistical analysis, Dr. AbdelMannan Aman for the assessment of participants invited to this study, and all the laboratory staff for their help with the data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study was conducted in accordance with the ethical standards set forth by Taibah University College of Dentistry Research Ethics Committee (TUCD-REC)], with the approval reference number [TUCD-REC/20171022/Nsr] obtained on October 22, 2017. Informed consent was obtained from all participants prior to their inclusion in the study. All procedures followed were in compliance with the Helsinki Declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.