
Abstract
Background
After the restoration of COVID-19 lockdowns and the relaxation of general public health restrictions, an upswing in the incidence of respiratory diseases was observed. Respiratory illnesses have been soaring among children with the easing of public health measures and because of the “immunity debt” that they are experiencing now.
Objectives
To identify and compare the incidence of respiratory tract infections in hospitalized children aged 1 month to 13 years in a tertiary care hospital from 2018 through 2023, covering three periods. To examine the difference in epidemiological characteristics such as age predilection, sex predilection, condition, mortality, and clinical and diagnostic investigations of community-acquired respiratory infections in three time periods (2018–2023).
Materials and Methods
A retro-prospective observational study was conducted. Hospital records of the pediatric department were the source of data.
Results
The total number of pediatric admissions in KIMS Al Shifa Hospital from August 2018 to May 2023 was 1,815, of which only 1,536 case files met the inclusion criteria. Among 1,536 cases, 642 admissions (pre-COVID period = 193 (41.9%), COVID period = 58 (19.8%), and post-COVID period = 391 (50.1%)) were due to non-COVID respiratory tract infections. This difference was found to be statistically significant (Chi-square = 80.2, p = 0.001).
Conclusion
Most of our study group was affected under 5–10 years of age, and most were affected with lower respiratory tract infections and required hospitalization. The reason behind this resurgence was the relatively feeble immune system.
Introduction
On January 30, 2020, WHO declared this outbreak a public health emergency of international concern and a pandemic on March 11, 2020. The pandemic had caused more than 633 million cases and 6.6 million confirmed deaths by November 9, 2022, making it one of the deadliest pandemics in history. 1 The first COVID cases in India were reported in Kerala on January 30, 2020. Public lockdowns were announced in Kerala on March 23 and nationally declared on March 25. COVID-19 infection rates started to drop by September 2021, 1 but the impact of these lockdowns presumptively contributed to a variation in the incidence and seasonal pattern of respiratory infections in children. 2 After the removal of lockdowns and moderation of public health restrictions, an increase in respiratory diseases was observed, mostly by viral etiology. 2 In August 2022, clinicians in several geographical areas notified the Centers for Disease Control and Prevention of an increase in hospitalization of pediatric patients with severe respiratory illnesses mostly due to viral etiology. 3 In a news report by “The Hindu,” a former superintendent of Sree Avittam Thirunal (SAT) Hospital, Trivandrum, found that respiratory illnesses have been soaring among children with the easing of public health measures and because of the “immunity debt” that they are experiencing now, which refers to the hypothesis that prolonged reduction in exposure to common pathogens during lockdowns and school closures may reduce immunity in certain populations, particularly children. Reduced exposure could limit immune system priming against routine pathogens, making individuals more susceptible to infections when exposure increases. During the pandemic, children had little exposure to the respiratory viruses that they might have normally encountered. All children are thus susceptible to new infections, and in schools, it is observed that entire classes fall sick. 4 A similar scenario of a surge in the case of severe respiratory infections in children was reported all over India and other countries. Similarly, an unusual rise in hospital admission for respiratory infection in pediatrics has been observed in hospital—KIMS Al-Shifa Hospital, Perinthalmanna, a tertiary care hospital in Malappuram. There is a lack of research regarding the same in the South Indian context, and further studies can be done using immunological evaluation in order to obtain physical evidence. Respiratory tract infections (RTIs) are generally one of the most common pediatric diseases, thus are identified as a major public health concern in both developing and developed countries and they possess a hectic economic burden globally. 5 This study hypothesizes that prolonged non-pharmaceutical interventions (NPIs) during the COVID-19 pandemic, including school closures and social distancing measures, reduced children’s exposure to common respiratory pathogens. The primary objective of this research is to assess trends in respiratory infection incidence and severity during three distinct periods: pre-COVID, during-COVID, and post-COVID. By comparing these periods, the study aims to determine whether the relaxation of NPIs impacted respiratory infection patterns in the pediatric population.
Materials and Methods
The retro-prospective observational study was conducted in a tertiary care hospital located in Perinthalmanna in Malappuram district. People from all over the country come and avail hospital facilities, providing a diverse sample population. All children aged 1 month to 13 years admitted in the pediatric department of the study setting whose records were available from August 2018 through May 2023 were included. Records that were incomplete and did not satisfy the definition criteria of respiratory infection were excluded. The retrospective phase included the data from April 2018 to December 2022, and we could retrieve the anonymized data from electronic medical records at KIMS Al-Shifa Hospital, Perinthalmanna. In the prospective phase, data were collected after obtaining informed consent for the inclusion of each patient. The prospective phase lasted 6 months, starting from December 2022 to May 2023. This design enabled a longitudinal analysis of existing records with prospective observational insights during the study’s ongoing phase.
All data were collected using a purpose-designed form, which is a standardized data collection form designed to capture demographic, clinical, and treatment-related information consistently across phases. The form was designed in collaboration with healthcare professionals and underwent preliminary validation through pilot testing to ensure relevance and clarity, which included the variables considered for the study. Initially, an analysis was performed on overall visits to the pediatric department, focusing on patient demographics, reasons for admission, vital signs, abnormal lab data, and diagnoses. Subsequently, diagnoses of airborne infections such as lower and upper airway infections, pneumonia, bronchitis, bronchiolitis, streptococcal infections, and acute otitis media were collected from the total number of cases in the pediatric department. Cases diagnosed with fever of unknown origin (FUO) were also included in the analysis as suspected infectious conditions. Additionally, certain other variables were subjected to analysis.
Seasonal variations in respiratory infections were acknowledged, as respiratory admissions typically increase during the winter months. The study was conducted over several seasons, allowing for some level of seasonal variation in infection rates to be considered. Additionally, concurrent health interventions, such as vaccination campaigns during the post-COVID period, may have influenced infection trends. These factors were considered during the study design, although explicit control for seasonality and other interventions was not part of the analysis.
The study was conducted in four phases:
Phase 1: Retrospective data collection
During the retrospective data collection phase, the data were pooled since pre-COVID and up to the end of COVID timelines, that is, 2018–2022. The data were obtained from the hospital’s medical records department and recorded in the data collection form. To ensure completeness and accuracy, data were cross-verified with electronic medical records and hospital logs where available, ensuring consistent representation across the study period. The data were sorted into two groups: respiratory infections and others. The data pertinent to respiratory infection were transferred into the data collection form with all the characters on it.
Phase 2: Prospective data collection
In the prospective study, all the pediatric cases were collected and followed up in real-time from the nursing station and the respective wards from the period December 2022 to May 2023, and the data obtained were copied into the working chart. The cases were taken and observed during hospital visits, and data about them were collected based on their characteristics. The process of sorting data was similar to that of phase 1.
Phase 3: Documentation of data
The collected data were documented in the data collection forms and added to a spreadsheet chart for the convenience of analysis and segregation. The data were taken from the medical records department with prior permission and in the presence of the respective officers, and they were confidentially noted down.
Phase 4: Evaluation and epidemiological characterization of collected data
In this phase, the collected data were thoroughly verified and analyzed with respect to the criteria. The data were evaluated and converted into different classes based on their epidemiological characters by using different software, including Microsoft Excel. Classified data were again converted into different representation charts for convenient identification and understanding.
Source of Data and Statistical Analysis
The data for the study were taken from patient case sheets, treatment charts, laboratory findings, discharge cards, and personal interviews with the patient. A well-designed patient data collection form was developed to record patient-related information. It mainly covers aspects like patient demographics, which includes the basic information of the patient along with sex, age, hospital medical records department (MRD) number, date of hospital admission and date of discharge, vital signs, characteristics of RTI, final diagnosis, diagnostic investigations, laboratory data, discharge details, and duration of hospital stay. Our study initiated with a null hypothesis that there is no significant difference in the proportion of RTIs in hospitalized children aged 1 month to 13 years during the three time periods: before and during the emergence of COVID-19 and after the easing of COVID-19 social restrictions. Our alternative hypothesis was that there was a significant increase in the proportion of RTIs in hospitalized children aged 1 month to 13 years during the period of easing COVID-19 social restrictions. All consecutive case records of the pediatric department satisfying the inclusion and exclusion criteria were included as samples. Graphical presentations were made to identify trends in the proportion of respiratory infections and other epidemiological characteristics in different periods. The Chi-square test was done to test a significant difference in the proportion of respiratory infections during the three time periods.
Results
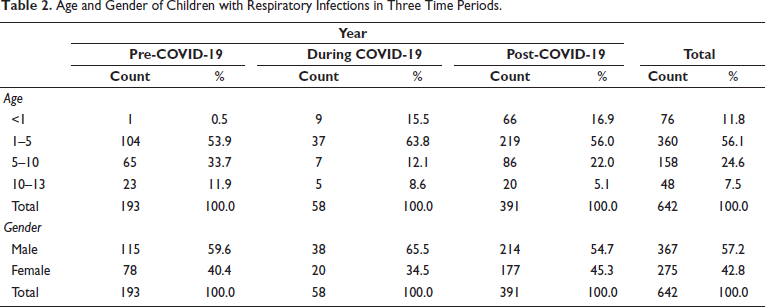
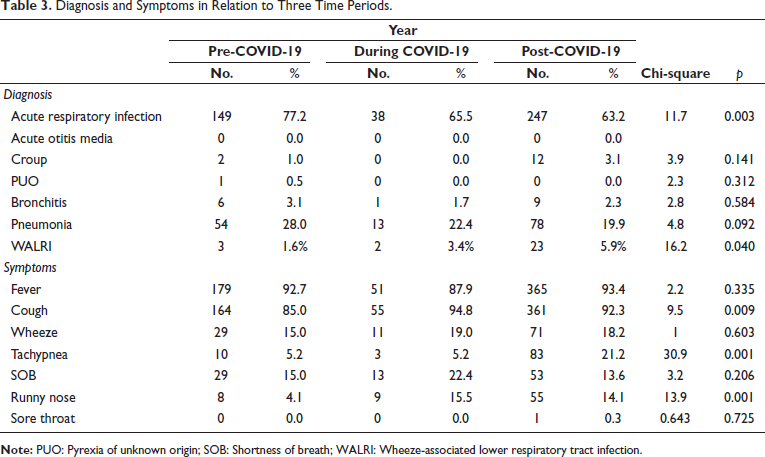
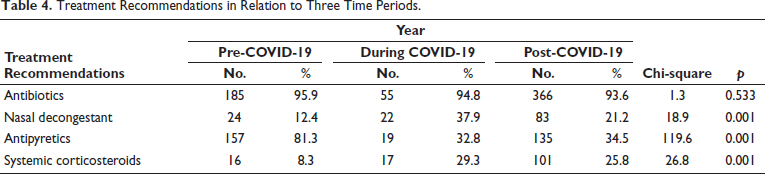
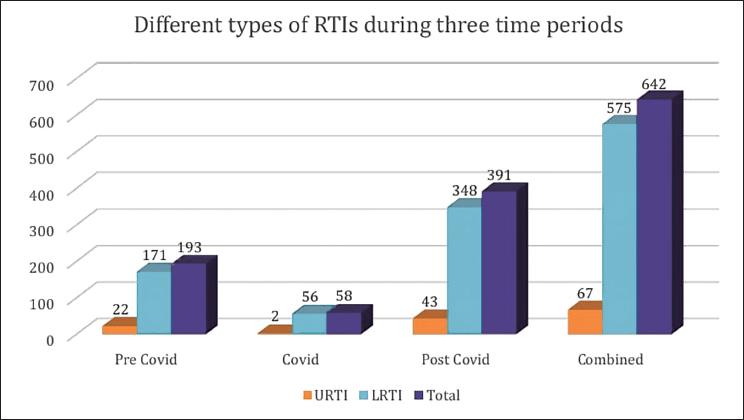
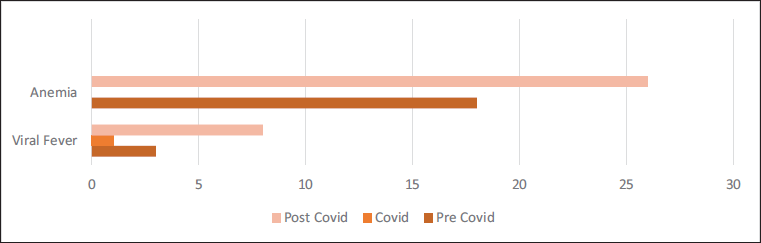
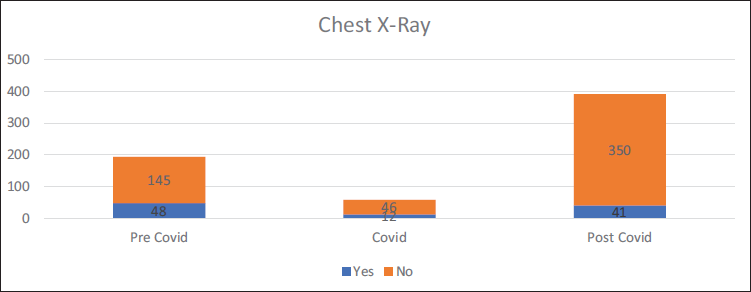
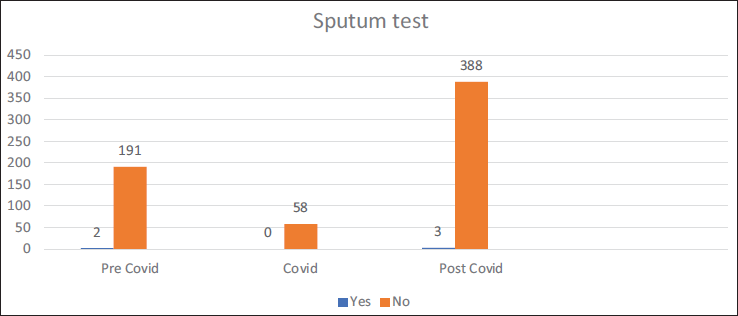
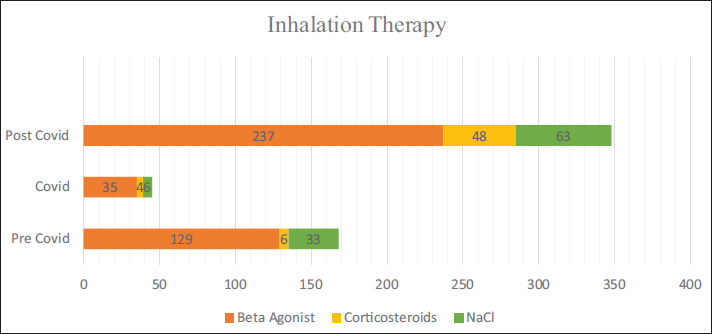
Total pediatric admissions in the hospital from August 2018 to May 2023 were 1,815, of which only 1,536 case files met the inclusion criteria and were complete with respect to demographic data, clinical diagnoses, and treatment records. Among 1,536 cases, 642 admissions (pre-COVID period = 193, COVID period = 58, and post-COVID period = 391) were due to non-COVID RTIs. According to Table 1, non-COVID respiratory infections were observed more during the post-COVID period, 50.1% (n = 391) as compared to pre, 41.9% (n = 193) and the period, 19.8% (n = 58). This difference was found to be statistically significant (Chi-square = 80.2, p = 0.001). A comparison of the ages of children with respiratory infections in the three time periods is shown in Table 2. It was observed that 79.3% (n = 46) of children with respiratory infections during the COVID period were under 5 years of age. The corresponding percentages in the pre- and post-COVID periods were 54.4% (n = 105) and 72.9% (n = 285). The observed difference was found to be statistically significant (Chi-square = 50.0, p = 0.001). The gender-wise classification, as in Table 2, shows that the number of male children infected more than females, as high as 65.5% (n = 38) during COVID as compared to 59.6% (n = 115) and 57.2% (n = 214), respectively, during the pre- and post-COVID periods. The difference was found to be not statistically significant (Chi-square = 3.0, p = 0.217). Out of a total of 642 RTIs, 10.4% (n = 67) were upper respiratory tract infections (URTIs) and 89.6% (n = 575) were lower respiratory tract infections (LRTIs); thus most of the RTIs were found to be LRTIs during all three time periods. The pre-COVID period showed 88.6% (n = 171) of LRTIs, while it became 96.6% (n = 56) and 89.0% (n = 348) during the COVID and post-COVID, respectively (Figure 1), which showed no significant difference among them (p = 0.187, Chi-square = 3.5). Diagnosis about three time periods is shown in Table 3. The corresponding percentage of children with acute respiratory infection (ARI), croup, pyrexia of unknown origin (PUO), bronchitis, and pneumonia in the pre- and post-COVID periods were 77.2% (n = 149) and 63.2% (n = 247) (Chi-square =11.7, p = 0.003), 1.0% (n = 2) and 3.1% (n = 12) (Chi-square = 3.9, p = 0.141), 0.5% (n = 1) and 0.0% (n = 0) (Chi-square = 2.3, p = 0.312), 3.1% (n = 6) and 2.3% (n = 9) (Chi-square = 2.8, p = 0.584), 28.0% (n = 54) and 19.9% (n = 78) (Chi-square = 4.8, p = 0.092), and 1.6% (n = 3) and 5.9% (n = 23), respectively. Other associated diagnoses, such as anemia and viral fever during the pre-COVID and post-COVID periods, were 9.3%, 8.1%, 1.6%, and 2%, respectively (Figure 2). The difference in the corresponding percentage of ARI, croup, bronchitis, and pneumonia in the pre- and post-COVID periods was statistically significant. Symptoms in relation to the three time periods are shown in Table 3. The corresponding percentage of children with fever in the pre- and post-COVID periods was 92.7% (n = 179) and 93.4% (n = 365) (Chi-square = 2.2, p = 0.335), cough 85.0% (n = 164) and 92.3% (n = 361) (Chi-square = 9.5, p = 0.009), wheeze 15.0% (n = 29) and 18.2% (n = 71) (Chi-square = 1.0, p = 0.603), tachypnea 5.2% (n = 10) and 21.2% (n = 83) (Chi-square = 30.9, p = 0.001), shortness of breath (SOB) 15.0% (n = 29) and 13.6% (n = 53) (Chi-square = 3.2, p = 0.206), runny nose 4.1% (n = 8) and 14.1% (n = 55) (Chi-square = 13.9, p = 0.001), respectively. Other symptoms such as rhinitis, rhonchi, vomiting, and cold were also observed. The difference in the corresponding percentage of cough, tachypnea, and runny nose was found statistically significant. Chest X-rays were more performed during the pre-COVID period 24.9% (n = 48) as compared to the post-COVID period 10.5% (n = 41). From Figure 3, we can observe the decline in chest X-ray suggestions along with the time. This difference was found to be statistically significant (Chi-square = 21.3, p = 0.00). From Figure 4, it is clear that the sputum test rate is very negligible in our hospital; from these periods, only five patients were prescribed to test sputum (Chi-square = 0.621, df = 2, p = 0.733). Treatment recommendation in relation to three time periods is shown in Table 4. The corresponding percentage of children who received antibiotics, nasal decongestants, antipyretics, and systemic corticosteroids during the pre- and post-COVID periods were 95.9% (n = 185) and 93.6% (n = 366) (Chi-square = 1.3, p = 0.533), 12.4% (n = 24) and 21.2% (n = 83) (Chi-square = 18.9, p = 0.001), 81.3% (n = 157) and 34.5% (n = 135) (Chi-square = 119.6, p = 0.001), 8.3% (n = 16) and 25.8% (n = 101) (Chi-square = 26.8, p = 0.001), respectively. The observed difference in the corresponding percentage of nasal decongestants, antipyretics, and systemic corticosteroids was statistically significant. There were several other medications given alongside the primary treatments, but while comparing the data, most of the treatments declined in the post-COVID period compared to pre-COVID. Anti-tussives 1.5% (n = 3) to 3.5% (n = 14), leukotriene receptor antagonist (LTRA) 5.1% (n = 10) to 7.4% (n = 29), and cough suppressants 1.0% (n = 2) to 10.2% (n = 40) were the only treatments which increased at post-COVID compared to pre-COVID period. The need for oxygen during the three time periods was 7.3% (n = 14), 29.3% (n = 17), and 11.3% (n = 44) (Chi-square = 21.2, p = 0.000), respectively. The corresponding percentage of children who received oxygen therapy was found to be significantly increased during the COVID period but came back to normal after the COVID-19 pandemic (Chi-square = 21.2, df = 2, p = 0.001). The inhalation therapy showed some significant changes in the application of the drugs during the three periods. From Figure 5, the use of corticosteroids increased from 3.1% (n = 6) during pre-COVID to 12.3% (n = 48) in post-COVID (Chi-square = 13.6, p = 0.001). Even though the percentage of beta-agonists decreased from 66.8% to 60.6%, the number of patients significantly increased from 129 to 237 (Chi-square = 2.2, p = 0.323). The need for an intensive care unit (ICU) during three time periods was 6.2% (n = 12), 22.4% (n = 13), and 9.7% (n = 38) (Chi-square = 13.2, p = 0.001), respectively. The observed difference during the pre- and post-COVID was found to be not statistically significant. Almost all patients were relieved of symptoms, and no significant difference was observed during the three time periods. 100% of patients were relieved during the pre-COVID period (n = 193). It became 98.3% (n = 57) and 99.2% (n = 388) during the COVID and post-COVID periods.
Incidence of Respiratory Infections During Pre-COVID, COVID, and Post-COVID Periods.

Age and Gender of Children with Respiratory Infections in Three Time Periods.
Diagnosis and Symptoms in Relation to Three Time Periods.
Treatment Recommendations in Relation to Three Time Periods.
Associated Diagnosis in Relation to Three Time Periods.
Chest X-ray in Relation to Three Time Periods.
Sputum Test in Relation to Three Time Periods.
Inhalation Therapy in Relation to Three Time Periods.
Discussion
Following the contingency of the COVID pandemic, the government is obligated to adopt some strict NPIs to constrain the same. Social distancing, recurrent sanitization, wearing masks, and closing schools, along with others, all of these precautions were helpful in reducing the spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Also, they altered the pattern of incidence of other commonly occurring respiratory infections. The incremental relaxation of NPIs affected the rate of respiratory infections over time, and the recent implementation to relax mask usage came out in March 2021, causing a surge in a variety of non-COVID respiratory infections. Similarly, an unusual rise in hospital admissions for respiratory infections in children has been observed in the tertiary care hospital in Perinthalmanna, Malappuram. This retrospective study investigated the number of hospital admissions and the epidemiological characteristics of patients aged 3–13 years who were evaluated at tertiary care level hospitals.
This study showed a significant impact of NPIs adopted to constrain the COVID pandemic on the circulation of other common respiratory viruses. The results found regarding the incidence of non-COVID RTIs were that non-COVID respiratory infections were more prevalent during the post-COVID period (50.1%, n = 391) as compared to the pre-COVID period (41.9%, n = 193) and the COVID period (19.8%, n = 58). The difference was found to be statistically significant. This resurgence of respiratory infections during the post-COVID period was also reported in several countries like Japan, the UK, Austria, and New Zealand.6–9
This out-of-season resurge was observed mainly 2 weeks after the reopening of schools in early September and found a steep increase in the number of diagnoses of respiratory syncytial virus (RSV) infections. Since children have much more difficulty with the physical distancing rules, the reopening of schools resulted in a sharp increase in the number of infections detected, comparable to the same in 2019. While comparing the age groups of the children, which seems to support the abovementioned point, the children belonged to the age groups of 1–5 and 5–10. The vast majority of cases (79.3%, 54.4%) occurred during the COVID and pre-COVID periods, respectively. These two groups combined made an increase after the pandemic too (72.9%). Most of the children in these categories are supposed to be in correspondence with the public, and as they neglected physical distancing and other guidelines, this caused a significant rise in their specific age category. The prevalence in age groups of RSV infection in our study followed the same trend of international and local, as it was found to be more prevalent in children of small age and decreased with the ascendence of age. The out-of-season resurgence of RSV was justified with the hypothesis that the diminished exposure of children to the virus may lead to a reduced immune stimulation needed to keep the humoral immune response efficient against the virus and, therefore, increase the number of susceptible individuals.10, 11 A study conducted by Liu et al. states that children were exposed to pathogens at lower frequencies during the lockdown, which might have affected the development of “trained immunity.” 12 The incomplete innate immune responses might result in a higher vulnerability to viruses such as RSV during the post-COVID-19 period. However, a study by Pletz et al. quantified the anti-RSV antibodies in a population of a small rural town and found that the decrease in the anti-RSV antibodies was not significant and could not alone be responsible for the increase of cases. 13 They assumed that the resurgence of RSV to a time-related pressure led to a delay in the initial catch-up of the usual infection rate due to COVID restrictions, which caused the surge in the same. 13 From our study results, it was quite evident that male patients (59.6%, 65.5%, and 54.7%) during the pre-COVID, COVID, and post-COVID periods were comparatively in higher proportions than females, though this was not statistically significant. The trend of higher infection rates in male children aligns with findings in similar studies, such as the study by Jeon et al. in the northern United Arab Emirates. 14 However, we did not specifically collect data on healthcare access or gender-based utilization, which future research could explore. Our study showed a change in the distribution of the types of non-COVID respiratory infections diagnosed. We have classified the infections as LRTI and URTI. The main diagnoses we recognized were ARI, otitis media, croup, PUO, bronchitis, wheeze-associated lower respiratory tract infection (WALRI), and pneumonia. A few associated diagnoses, such as anemia and viral fever, were also observed. Since LRTI typically lasts longer and is more serious than URTI, most of the observed RTIs were LRTI (88.6%, 96.6%, and 89.0%) during the pre-COVID, COVID, and post-COVID, respectively, in all time periods, with no significant difference among them. The hospitalization count for ARIs has increased in the post-COVID period, while pneumonia cases decreased during the same period, which may be influenced by multiple factors. Although we did not conduct pathogen-specific lab analyses for each case, clinical diagnoses pointed to common pathogens, including RSV, adenovirus, influenza, and Streptococcus pneumoniae. The relaxation of COVID-19 public health measures likely contributed to the resurgence in viral infections such as RSV and influenza, which are associated with ARIs rather than pneumonia. The results of our study are similar to those of a study conducted in Italy by Maglione et al., where they evaluated the changing epidemiology of acute viral respiratory infections in hospitalized children. 15 During these periods, the children were not compatible with the vaccine administration, and most of them never appeared or were even suggested for the lab tests to identify the COVID-19 infection; this may also have confounded the selection. The symptom-based segregation revealed a significantly higher rate of cough (7.3% increase), tachypnea (16.0% increase), and runny nose (10.0% increase). A study conducted by Song et al. found increased cases of patients suffering from a fluctuating or persistent cough months after recovery from COVID-19. 16 This result supports the hypothesis that pathways of neuroimmunomodulation, neurotropism, and neuroinflammation through the vagal nerves, featured in SARS-CoV-2 infection, lead to a state of cough hypersensitivity. The other relevant symptoms like wheezing, tachypnea, SOB, runny nose, rhinitis, rhonchi, vomiting, and cold were observed to sustain a significant occupation but did not show any significant increase in rate during any of the three phases of the study.
Treatment recommendations in relation to the three time periods reveal that antibiotics, nasal decongestants, antipyretics, and systemic corticosteroids were the most implemented treatment options during these periods in our study setting. The observed increase in the corresponding percentage of nasal decongestants, antipyretics, and systemic corticosteroids from our results shows a change in prescribing pattern as well, especially in the case of systemic corticosteroids, which showed a subtle surge during the COVID period and post-COVID period. Several studies by FakhriRavari et al. identified the effectiveness of systemic corticosteroids for treating respiratory infections, 17 suspected COVID-19 cases, and post-COVID respiratory syndromes. We could not observe any solid change in the application of oxygen therapy and inhalation therapies except for corticosteroids. A great decline in the prescription of chest X-rays was observed after the pandemic; the change in this prescribing pattern made it shrink by half during the post-COVID period. The sputum culture test did not show any significant change. Pediatric ICU admissions were observed, which shows a significant elevation of ICU admission incidents during the COVID-19 period but which returned to normal after the COVID period.
The strengths of our study are that we could collect a vast number of cases over 5 years within our limited time, which enabled us to analyze trends and seasonal patterns of the different respiratory infections in our target population. We could include a variety of clinical demographics, lab values, and related data that helped to provide additional information about the treatment patterns during the periods. As the data acquisition was optimized using a computerized query tool, we could limit the acquisition errors to a greater limit. In our study setting, a tertiary care hospital had a similar procedure for handling admissions and criteria for discharge; these standard procedures also helped us avoid site-to-site variability. The study primarily employed Chi-square tests to assess statistical differences across periods due to the categorical nature of the data. We acknowledge that regression analysis controlling for confounders would provide more depth, which could be explored in future studies with larger datasets. Our study has several limitations. First, our retrospective prospective approach allowed us to identify and organize relevant data to support our hypothesis; however, there are opportunities for further improvement. The study was conducted in a tertiary care hospital setting. Nevertheless, conducting a multicentered study could have enhanced its broader relevance and applicability to the general population while also enabling us to gather a larger dataset of cases. Additionally, our reliance solely on medical records within the hospital database restricted our dataset to medical information, excluding important factors like socio-economic data. While our study observed trends in respiratory infections, it is important to note that confounding variables such as seasonal variations and concurrent health interventions may have influenced the results. Respiratory infections are typically more common during the winter months, which may have contributed to the observed trends in infection rates. Consequently, we were unable to establish causal relationships. While we relied on clinical diagnoses, future studies should include microbiological analysis and vaccination data to further clarify these pathogen-specific trends. Another concern is the potential for sampling bias since only moderate and severe childhood infections often require hospital diagnosis. Furthermore, we also identified inevitable confounding factors, such as changes in health-seeking behavior due to COVID-19 fears, which may have affected the findings.
Conclusion
Our study shows that there is an impact of the relaxation of NPIs associated with COVID-19 on the pattern of incidence of other infections, especially RTIs, in the pediatric population. NPIs for the prevention of the spread of COVID-19 could potentially prevent the transmission of different respiratory viruses, which also created a herd of susceptible individuals, which might have resulted in larger outbreaks once the transmission routes were reopened. The reason behind this resurgence was concluded to be a relatively feeble immune system and the increased social activities of the pediatric population that have not been exposed to natural RSV or other respiratory pathogens but became exposed upon the lifting of restrictions, even though the real reason behind this phenomenon is still unclear. Our data suggest that current NPIs adopted by schools cannot effectively prevent the transmission of respiratory pathogens, and results indicate that healthcare systems must be prepared for more future breakouts of common respiratory viruses, as COVID restrictions are relaxed. Thus, we expect to potentially contribute to the development and implementation of rapid interventions to diminish the burden of diseases on healthcare systems. Results from our study could be useful in the post-COVID-19 era, which may provide guidance when planning resources, implementing new guidelines, and rearranging healthcare systems to face potential future pandemics. Moreover, continuous and convenient healthcare surveillance and surveys of serologies are needed to understand furthermore about the long-term impact of the COVID-19 pandemic on the incidence pattern of commonly occurring respiratory viruses.
Summary
This study evaluates the impact of COVID-19 non-NPIs on pediatric respiratory infections across pre-COVID, during COVID, and post-COVID periods using data from 1,536 cases in a tertiary care hospital.
Post-COVID, ARIs increased, while pneumonia cases declined. These shifts may stem from reduced pathogen exposure during NPIs, termed “immunity debt,” alongside vaccination campaigns, healthcare-seeking behavior changes, and relaxed restrictions. Seasonal variations and concurrent health interventions were considered potential confounders.
The study highlights changes in prescribing patterns and emphasizes the need for healthcare preparedness, continuous surveillance, and pathogen-specific analyses to address future respiratory infection trends effectively.
Footnotes
Abbreviations
ARI: Acute respiratory infection; COVID-19: Coronavirus disease-19; FUO: Fever of unknown origin; ICU: Intensive care unit; LRTI: Lower respiratory tract infection; LTRA: Leukotriene receptor antagonist; MRD: Medical records department; NPI: Non-pharmaceutical intervention; PUO: Pyrexia of unknown origin; RTI: Respiratory tract infection; RSV: Respiratory syncytial virus; SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2; URTI: Upper respiratory tract infection; WALRI: Wheeze-associated lower respiratory tract infection.
Acknowledgments
The authors express their sincere gratitude to all those who supported and guided them throughout their project. Special thanks to the faculty, staff, and management for their valuable resources, time, and expertise.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.