
Abstract
Background
Insomnia is a significant public health problem that can affect up to 50% of older adults. Pharmacological treatments are commonly used such as benzodiazepines (BZD) and related Z-drug zopiclone.
Objectives
The objective of this study was to investigate the use of zopiclone under real-life clinical conditions.
Materials and Methods
A retrospective review of older patients was conducted in a French geriatric hospital. The eligible participants included patients aged 65 years and older who had received zopiclone as a hypnotic. The presence of indication, the dosage and duration of zopiclone, the reevaluation of the treatment, the reason for discontinuation, and the combination with BZD were assessed.
Results
The study included 30 subjects (mean age 84.6 ± 9.3 years), 90% of whom received zopiclone 3.5 mg and 10% zopiclone 7.5 mg. In 60% of cases, no indication of insomnia was found. At discharge, more patients received a combination of zopiclone and BZD. The drug reassessment was initiated in only nine patients.
Conclusion
The treatment of insomnia with zopiclone is usually prescribed for long-term periods in older adults with less need for reevaluation. More long-term data on side effects and therapeutic efficacy are needed in routine clinical practice.
Introduction
The Diagnostic and Statistical Manual of Mental Disorders (DSM) of the American Psychiatric Association defines insomnia disorder as a predominant complaint of dissatisfaction with the quantity or quality of sleep. 1 The main manifestations of insomnia include difficulty falling asleep at bedtime, recurrent or persistent difficulty maintaining sleep, or early-morning awakening with the inability to return to sleep. Chronic insomnia arises at least three times a week and persists for more than three months, with daytime consequences despite adequate opportunity for sleep. This sleep disorder is a significant public health problem whose prevalence could be estimated at between 5% and 10% in the general US population. 2 However, the prevalence of insomnia varies largely between European countries, ranging from 5.7% in Germany to 19% in France. 3 In older adults, typically defined as aged 65 years and over, sleep disorders can affect up to 50% of them including the risk of falling.4, 5 Without treatment, they are associated with significant morbidity with the risk of development of mental disorders such as depression and anxiety in a bidirectional manner.6, 7 Moreover, daytime cognitive impairment has been reported in patients including tasks assessing attention, working memory, and executive functions.8, 9 For the clinical management of chronic insomnia, cognitive-behavioral therapy is recommended as first-line treatment in adults comprising psychoeducation, relaxation therapy, sleep-restriction therapy, stimulus control therapy, and severe cognitive therapeutic strategies.3, 10 However, in older adults, pharmacological treatments are commonly used to treat sleep disorders, such as benzodiazepines (BZD) and related Z-drugs (zolpidem, zopiclone). 11 If published consistent recommendations limit the duration of treatment to a maximum of 4 weeks, long-term use of these drugs still remains common in the elderly population, regardless of restrictions related to potentially severe adverse events, tolerance, dependence, and withdrawal symptoms.11–13 Z-drugs such as zopiclone are preferred for the treatment of insomnia because of their safety and tolerability profile compared with BZDs.14, 15 In the short term, zopiclone is relatively well tolerated, with no significant impact on psychomotor or cognitive performance, and appears to reduce sleep latency and nocturnal awakenings. 14 Zopiclone use in older adults can result in adverse events such as fatigue, headache, nightmares, nausea, and gastrointestinal issues. 16 However, the adverse events are usually mild and short-term and infrequently result in withdrawal. 14 Withdrawal effects with 7.5 mg zopiclone have been reported in a few studies, including delirium, forgetfulness, and excessive sleepiness.17, 18 In practice, pharmacological agents are used for the long-term treatment of persistent insomnia, although regulatory agencies give indications only for acute treatment. Considering the significance of zopiclone use for the treatment of insomnia in our French geriatric hospital, the aim of the current study was to evaluate its use under real-life conditions.
Objectives
To investigate the use of zopiclone in real-life clinical practice in older adults hospitalized in a French geriatric hospital.
Materials and Methods
An institutional board-approved retrospective review of older patients admitted in our French geriatric hospital was performed for 2022. The patients were selected using a patient cohort visualization tool (Cohort360, health database of Assistance Publique des Hôpitaux de Paris registered with the French national data protection authority CNIL, authorization no. 1980120), which enables queries to be made directly in electronic medical records. The eligible participants were patients aged 65 years and over who had received zopiclone as a hypnotic for insomnia. The presence of an indication, the dosage and duration of zopiclone, the reevaluation of the treatment, the reason for discontinuation, and the combination with BZD were assessed. The demographic data (age and sex), the number of medications, the reason for admission, the history of cognitive impairment, and the length of stay were performed during the study period. Quantitative variables were reported as mean and standard deviation (SD), and qualitative variables as absolute proportion and percentage. Statistical analysis was performed using Microsoft Excel 2016 (Microsoft Corporation, Santa Rosa, CA).
Results
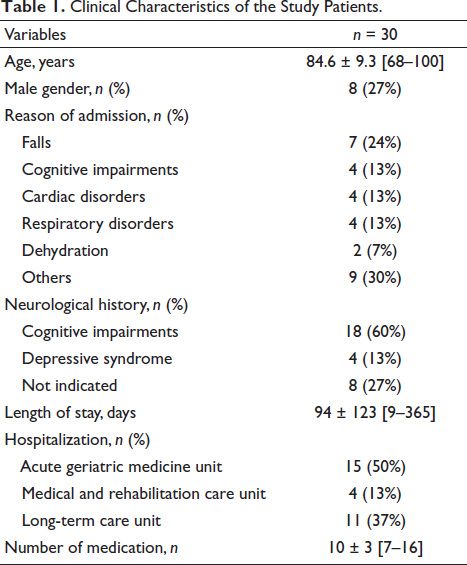
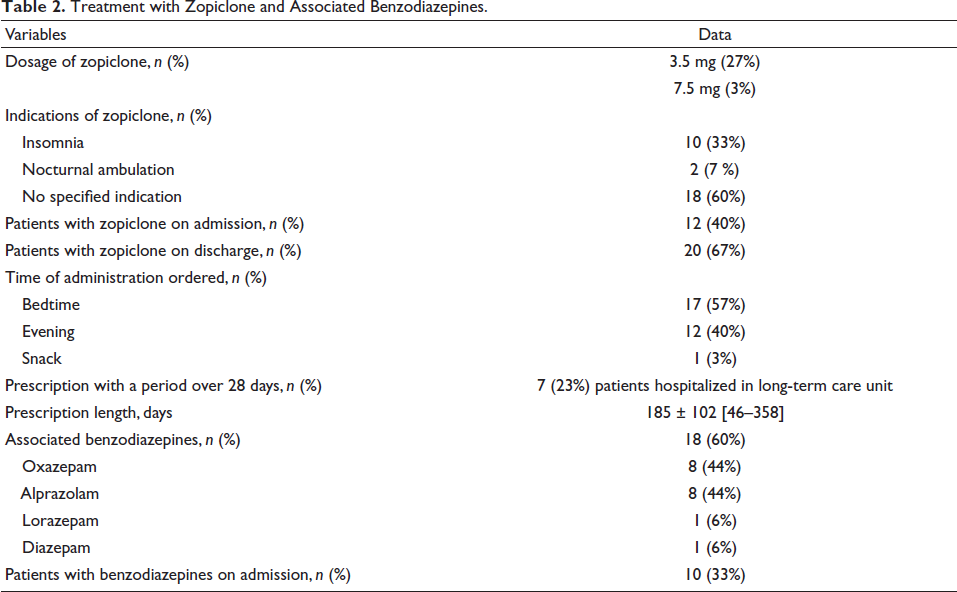
The study group consisted of 30 patients with a mean age of 84.6 ± 9.3 years [range 68–100 years], including 8 men (27%). The patient’s characteristics are detailed in Table 1. Most patients experienced neurological disorders such as cognitive impairments and depression syndrome. The length of stay was fairly long, with a mean of 94 days. Among the 30 patients, 27 (90%) were treated with zopiclone 3.5 mg and 3 (10%) with zopiclone 7.5 mg (Table 2). In most cases (60%), no indication was found for zopiclone treatment. Zopiclone was introduced in 18 patients during their hospital stay, and 12 were admitted with their medication in place (Table 2). At discharge, more patients received zopiclone. The timing of administration was respected in 17 (57%) patients, with zopiclone ordered just before bedtime (Table 2). Although 33% of patients had already taken a BZD on admission, a further 60% received a BZD during hospitalization. The short half-life anxiolytic BZD was largely dispensed, especially oxazepam and alprazolam. A reassessment of the drug use was initiated in nine patients, with withdrawal in five and discontinuation in four. Sedating anti-depressants were also prescribed, such as mianserin and mirtazapine in six patients (20%).
Clinical Characteristics of the Study Patients.
Treatment with Zopiclone and Associated Benzodiazepines.
Discussion
The use of hypnotic drugs has increased over the past decades, with a marketed escalation for drugs over BZD. 19 Zopiclone is a non-BZD hypnotic commonly prescribed for the short-term treatment of insomnia in adults.3, 14 Long-term continuous use is not recommended, and the course of treatment should employ the lowest effective dose specifically for older adults. Few data are available on the practical use of zopiclone in hospitalized elderly patients. 12 Our study showed good compliance for the lowest possible prescribed dosage in the older patients, but often with an inappropriate time of administration in the evening rather than at bedtime. For patients hospitalized in the long-term care unit, the course of treatment by zopiclone was maintained during the study period for up to 1 year. Long-term use of zopiclone beyond 4 weeks is not recommended due to the limited scientific data on tolerability and safety in the elderly.3, 14 Thus, reassessment of zopiclone or related drug treatment after 4 weeks should be carried out consistently to anticipate drug discontinuation. In our study, worsening of treatment was observed with the combination of a BZD in 60% of patients. Despite long-term treatment with Z-drugs being an off-label use, meta-analyses have suggested favorable benefits of eszopiclone for up to 6 months of application in some cases, although this should be decided on an individual basis after carefully weighing the advantages and disadvantages of Z-drugs.20, 21 A systematic review suggested better tolerability and safety of the drug compared with withdrawal symptoms, craving, and severe rebound insomnia associated with high-dose use of zopiclone. 21 An option of drug administration for at least 3 months should be proposed for the use of daridorexant or extended-release melatonin regardless of long-term data requirements. 10 Daridorexant, a dual orexin receptor antagonist, should provide a safe and effective therapeutic alternative for patients with insomnia whose response to current therapies is incomplete or inadequate. 22 Melatonin, freely available in most European countries, has been approved for the treatment of insomnia in older patients with mild to moderate effects on sleep-related parameters.23, 24 However, the long-term efficacy of melatonin needs to be evaluated. 24 Further treatment options for insomnia and comorbid medical disorders would be welcome, such as cannabinoids, or brain stimulation techniques.25, 26
Conclusion
This study demonstrated the widespread use of zopiclone treatment for insomnia in older adults in daily clinical practice. The limited number of patients involved in taking the data must be treated with caution. First-line treatment of insomnia with melatonin may offer an alternative to systematic initiation with zopiclone. More long-term data in routine clinical practice concerning treatment acceptance, side effects, and therapeutic efficacy are needed.
Impact Statements
Zopiclone is commonly used to treat sleep disorders in older populations regardless of the recommended duration limit.
If zopiclone is prescribed for a long-term period and associated with BZD, patients should be cautioned about the occurrence of various adverse events.
The investigation of zopiclone use in real-life clinical practice should help to adjust its prescription.
Authors’ Contributions
Helena Lebreton, Nadia Ladjouzi, and Joël Schlatter participated in the planning, literature search, and writing and critical revision of the article.
Data Availability Statement
Data are available from the authors upon reasonable request and with permission of the Paul Doumer Hospital. Further enquiries can be directed to the corresponding author.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The requirement for informed consent was waived by the Ethics Committee of the Paul Doumer Hospital because of the retrospective nature of the study. The patients were selected using a patient cohort visualization tool (Cohort360, health database of Assistance Publique des Hôpitaux de Paris declared with the French national data protection authority CNIL, authorization no. 1980120).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patients gave their oral consent to the use of their anonymized data.