
Abstract
Background
Diabetic ulcers are infections caused by the loss of the deepest skin tissue on the feet of patients with diabetes mellitus. Appropriate treatment, such as antibiotic therapy, is necessary to prevent the spread of infection and antibiotic resistance.
Objectives
This study aims to evaluate the use of antibiotics to treat diabetic foot ulcers (DFU) qualitatively using Gyssens analysis in the intensive care units (ICUs).
Materials and Methods
The study was held retrospectively by analyzing the quality of antibiotics used with Gyssens. Data collection was held at Roemani Muhammadiyah Semarang Hospital, Semarang City. Subjects involved in this study included all ICU patients who were prescribed antibiotics from January 2020 until December 2022.
Results
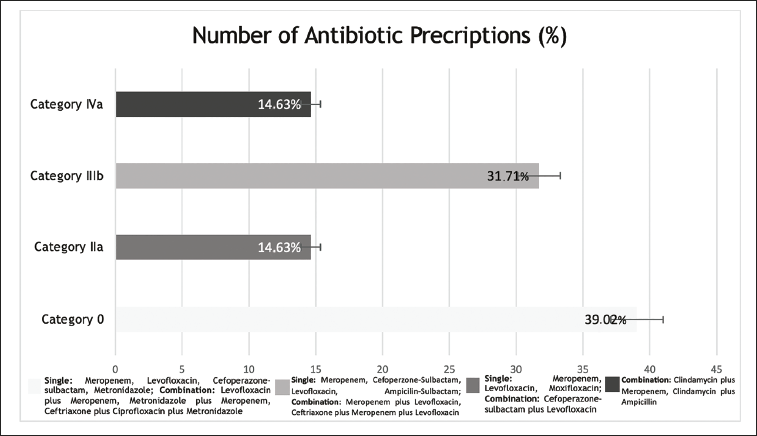
The results showed that the highest of single-use antibiotics was Meropenem (7.14%), the dual antibiotic combination was Clindamycin plus Meropenem (7.14%) and a triple antibiotic combination was Metronidazole plus Ceftriaxone plus Ciprofloxacin (3.57%), Ceftriaxone plus Meropenem plus Levofloxacin (3.57%). The accuracy of antibiotic use based on Gyssens analysis was obtained from 41 prescriptions it was the category appropriate were 16 prescriptions (39.02%), inappropriate doses were six prescriptions (14.63%), too short use was 13 prescriptions (31.71%), and more effective antibiotics needed were six patients (14.63%).
Conclusion
The utilization rate among antibiotics for the treatment of DFU was deemed inappropriate. It was also necessary to perform a bacterial culture before deciding on the mode of administration.
Introduction
Diabetic ulcer is an ulcer infection or loss of the deepest skin tissue on the foot of patients with diabetes mellitus, which is caused due to abnormalities in the peripheral nerves and arteries. Diabetic ulcers are the most common symptoms of diabetes mellitus. 1 Untreated diabetic ulcer infection will quickly spread and damage wider tissue. The risk of amputation can be reduced by 40% with a stable sepsis infection. 2
The most effective treatment for infections caused by diabetes is antibiotic therapy. Antibiotics are the most commonly used treatment for diseases associated with bacteria, despite increasing toxicity due to inappropriate antibiotics selection and their dosing, which can cause side effects such as worsening the condition, being patient-related diseases, and prolonging the duration of illness. Inappropriate antibiotics can also cause infections to become more persistent and last longer due to resistant microorganisms. 3
The most significant negative impact of inappropriate antibiotic use is the emergence and spread of antibiotic resistance, also known as antibiotic resistance. 4 The obstructs effective treatment services can be associated with increased health service costs or worsened morbidity and mortality cases. 5
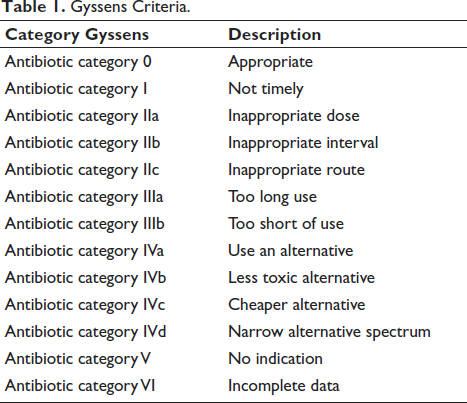
The issue of bacterial resistance has also become a growing problem worldwide. The WHO stated the importance of assessing factors associated with the problem and strategies to control the incidence of resistance. Antibiotic quality evaluation was the most effective method to identify bacterial resistance (Table 1).
Gyssens Criteria.
Materials and Methods
The study protocol was approved by the health research ethics committee at Roemani Muhammadiyah Semarang Hospital (reference number EA-008/KPEK-KSR/VII/2023).
Data were collected retrospectively at Roemani Muhammadiyah Semarang Hospital in Semarang City from May to June 2023 for this descriptive observational study. A total of 434 patients’ medical records were included in the study population. During data collection, 28 patients who met the inclusion criteria were identified after selecting 406 data samples [224 patients did not have antibiotic use documented, and 182 were not intensive care unit (ICU) patients]. These criteria included all ICU patients who were hospitalized and diagnosed with diabetic ulcers. All patients who received prescribed antibiotics in the period from January 2020 until December 2022 and who had complete medical records (patient age, gender, education, profession, diagnostic/International Classification of Diseases, Tenth Revision (ICD 10), drug data, duration of administration, length of stay (LOS) and route of administration, and frequency of administration.
The quality of antibiotic use was assessed according to Gyssens analysis. 6 This study was conducted by documenting all types of antibiotics used in hospitals for diabetic ulcer foot therapy. The antibiotic usage data was then compared with consensus or guidelines with the Ministry of Health Indonesia’s antibiotic usage guidelines (2021), The International Working Group on the Diabetic Foot (IWGDF) (2023), 7 and the American Diabetes Association (2021). 8
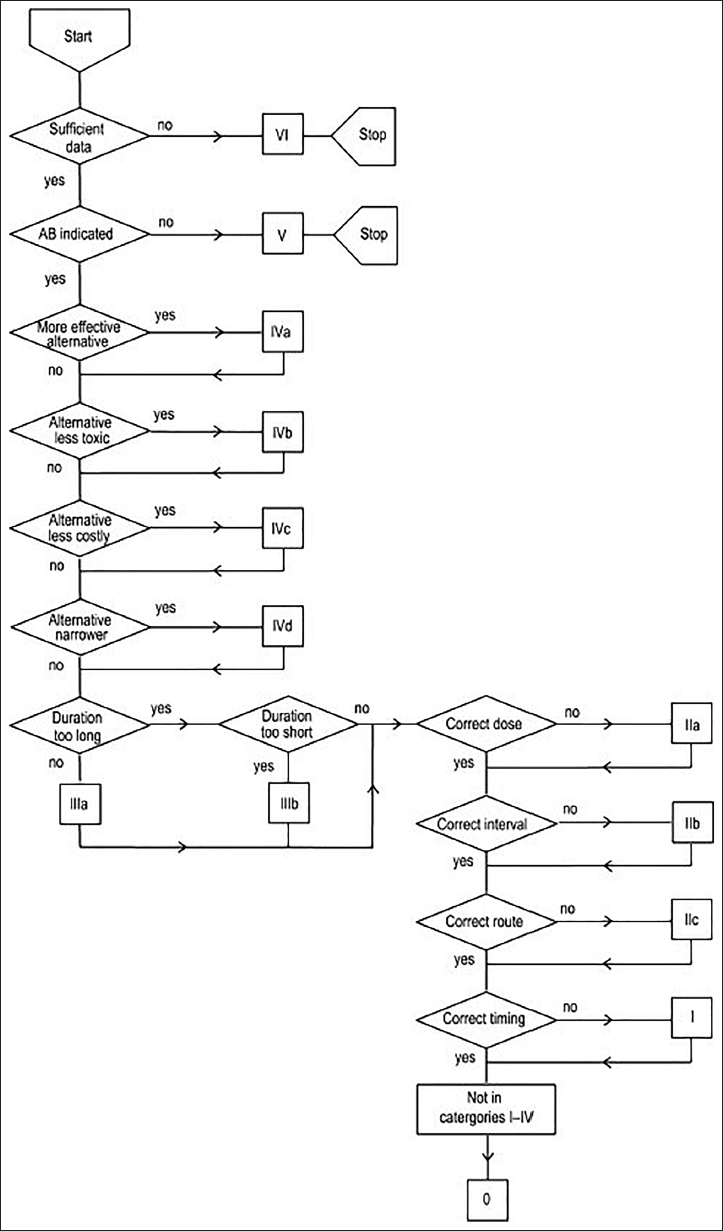
The data was analyzed based on indications, potential, toxicity, cost, and availability of administration duration, dosage, interval, route, and timing. Subsequently, it was categorized into 0–VI according to the Gyssens flow chart (Figure 1).
Antibiotic Usage Flow Chart by Gyssens. 7
Rationality Category of Antibiotic Use Based on Gyssens Method
Microsoft Excel was used for data processing. To characterize data from medical records and perform qualitative analysis, patients’ characteristics were described and calculated by the formula:
Patients’ characteristics:

Antibiotic profile:

Results
Characteristics of Diabetic Ulcer Patients
Based on medical records data taken at Roemani Muhammadiyah Semarang Hospital, the diabetic foot ulcers (DFU) patients were described by patient age, gender, education, profession, and diagnostic/ICD 10. All data samples collected were complete.
Antibiotics Use Profile
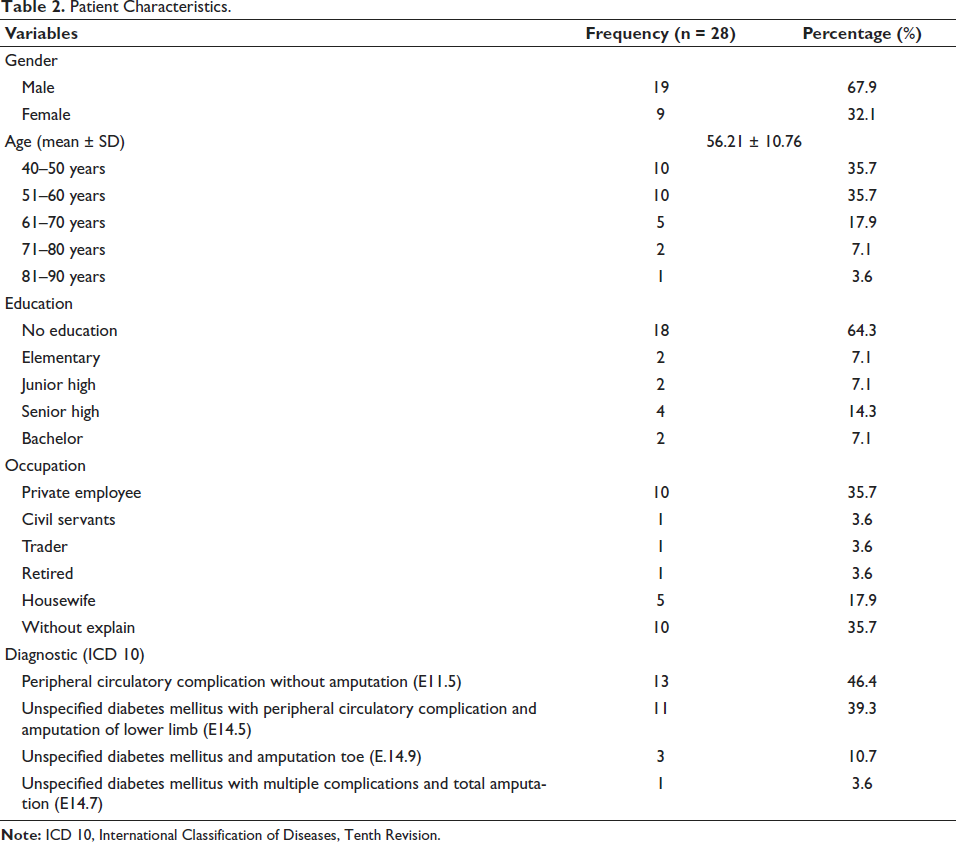
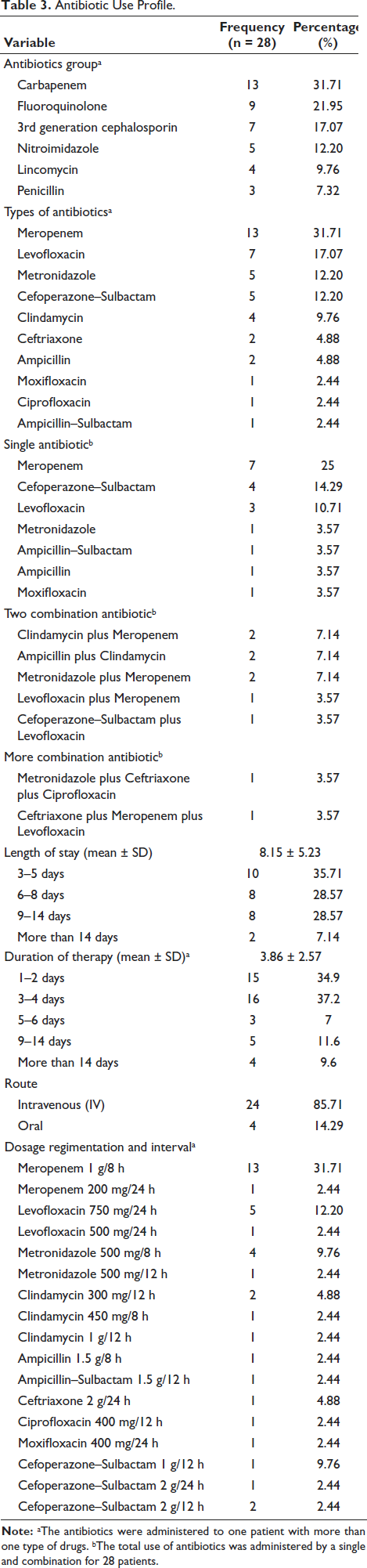
Table 2 shows the most widely used antibiotic meropenem. The carbapenem group was 13 (30.2%) based on the antibiotics use profile. A total of six (21.43%) meropenem antibiotics were commonly used. Clindamycin plus meropenem 2 (7.14%) was the most widely used combination of two antibiotics, and there were also three other types of combinations. The doses listed in the antibiotic use profile were 400 mg–2 g. Most dosage intervals were 8 h, and the chosen route of administration to DFU patients in the ICU room was intravenously (IV) and oral. The average LOS and duration of patients receiving antibiotics were 8.15 ± 5.23 and 3.86 ± 2.57 days.
Patient Characteristics.
Discussion
Characteristics of Diabetic Ulcer Patients
According to this study’s findings, 28 diabetic ulcer patients are displayed by gender. It can be seen that female patients slightly outnumber male patients with a ratio of 67.9% versus 31.1% (Table 2). This observation could be attributed to various factors. Men typically tend to be diagnosed younger than women. Still, women may have higher risk factors like obesity at diagnosis and experience a higher risk of cardiovascular complications from type 2 diabetes. 8 Basically, the risk of developing type 2 diabetes increases with age, obesity, and lack of physical activity. 9 In contrast to the study conducted by Piran et al, 10 the risk factors for the development of DFU were higher proportion in males compared to females due to the higher pressure on men’s lower limbs due to their average weight, as well as differences in lifestyle, and self-care. 10 The higher prevalence of atherosclerosis in males compared to females, may also contribute to the higher rate of DFUs in males. 11 Most commonly, complication and amputation patients outnumber those without complication with a ratio of 53.6% versus 46.4%. DFUs are associated with significant morbidity and a higher risk of lower limb amputation. DFU and amputations have a major impact on the patient’s quality of life. 12
The characteristics of the last education show that patients who have not received any education have a more significant percentage (64.3%) of DFU progressivity. These findings are from a study conducted by Yazdanpanah et al. which shows that patients who have low educational levels tend to experience worsening DFU. 13 As many patients were not educated, and their level of education influenced their awareness, it was seen patients with a longer duration of diabetes without complication have some awareness compared to patients with a shorter duration with DFU complication. 14 Many published studies have noted that low awareness and knowledge were attitudes to low-level education. A recent study by Fatima et al stated that only 7% of the study population (among 358 patients) had good foot care acquaintances and habits, 55.3% had average, and 37.7% had poor foot care acquaintances and habits. 15
The incidence of DFU in educated diabetic patients was less because they were likely to find access to information from many sources. In general, 64.3% of patients who have an occupation suffer from DFU, higher than patients with no occupation. A qualitative study conducted by Palmer et al stated that physically demanding jobs might contribute to the development of DFU in diabetic patients. 16 It relates to the previous study, that the high pressure on the lower limb increases the risk of DFU. Routine monthly foot checks can help reduce the risk of complications.
Antibiotics Use Profile and Gyssens Analysis
The selection of antibiotic treatment for DFU patients should be based on the severity of the infection and the likelihood that resistant organisms will be involved. In most cases, the DFU were polymicrobial. 17 Acute infection in a previously untreated patient was usually caused by aerobic Gram-positive cocci, but deep or chronic wounds often harbor polymicrobial flora, including aerobic Gram-negative and obligate anaerobic bacteria. 18 The systemic antibiotic that was indiscriminately used for skin ulcers without any sign of infection could accelerate the risk of antibiotic resistance. 19 The use of empirical antibiotics must cover Gram-positive cocci. However, the patients under antibiotic treatment must be considered by providing a broad spectrum for coverage of Gram-negative bacteria, too.
Carbapenem class was most widely used as a single antibiotic (47.06%) in DFU patients in the ICUs of Roemani Muhammadiyah Semarang Hospital (Table 3). Meropenem was a broad-spectrum Carbapenem antibiotic with excellent activity against many pathogens associated with severe DFU administered IV at 1 g every 8 h. However, the accuracy of this antibiotic is considered appropriate when used on patients with systemic inflammatory response syndrome (SIRS). 20 According to IWGDF (2023), the Carbapenem class was appropriately used in patients with accompanied risk factors for Gram-negative resistance. The second and third antibiotics most frequently used in this study were 3rd generation cephalosporin and Fluoroquinolone class, namely, Cefoperazone–Sulbactam (14.29%) and Levofloxacin (10.71%). In patients with DFU, Cefoperazone–Sulbactam and levofloxacin were widely used in moderate to severe infection-associated Gram-negative, gram-positive Penicillin-susceptible and Penicillin-resistant, specifically methicillin-resistant Staphylococcus aureus (MRSA). 21 Most commonly Clindamycin plus Meropenem (7.14%), Ampicillin plus Clindamycin (7.14%) and Metronidazole plus Meropenem (7.14%), is this antibiotic administered to DFU patients as a dual combination. For most cases of DFU, Clindamycin was rarely used without combination with other antibiotics due to its ineffective coverage polymicrobial, for which bactericidal antibiotics such as beta-lactam or Metronidazole are preferred. 22 Clindamycin was effective for mild MRSA infection as a choice for patients who have hypersensitivity to beta-lactam antibiotics.
Antibiotic Use Profile.
The combination of Clindamycin and Ampicillin or Meropenem was inappropriate because the mechanism of action was similar to coverage of Gram-positive anaerobe and some Gram-negative species similar to Propionibacterium, Porphyromonas, and included Staphylococcus epidermidis. 23 In our study, some of the used antibiotics were classified as an appropriate/rational category (39.02%) according to the Gyssens analysis that indicated compliance with the antibiotic therapy regimen with treatment guidelines and the accuracy of the diagnosis of DFU by medical personnel in the ICUs of Roemani Muhammadiyah Semarang Hospital. The evaluation findings also showed that treatment needs a narrower alternative spectrum, specifically, six out of the 41 prescriptions (14.63%). These antibiotics can be seen in Figure 2. Only one randomized controlled trial (RCT) by Graham et al recommended a combination of IV Piperacillin 3 g every 6 h plus IV Clindamycin 600 mg every 8 h for DFU treatment. 24 In contrast with Graham et al, most evidence recommended a dual combination with Clindamycin must be coverage for Gram-negative like Fluoroquinolone or 3rd generation Cephalosporin.20, 23, 25
Out of 41 Prescriptions Antibiotics from 28 Patients were Analyzed by Gyssens. Appropriate Category (n = 18 Patients), Inappropriate Dose Category (n = 6 Patients), Too Short of Use (n = 13 Patients), and Use an Alternative Antibiotic Category (n = 4 Patients).
Another finding was that 13 out of 41 antibiotic prescriptions were 31.71% too short a duration of antibiotic administration (less than 3 days). Using antibiotics for a shorter duration than recommended can result in treatment failure and the development of resistant bacteria to these antibiotic drugs, which is even more risky if the drug has adverse side effects. 26 In contrast to the study conducted by Palin et al that compared the short and long duration of antibiotic administration, giving long-duration treatment was no more effective than a shorter course. 27 Sometimes, the longest duration is specified depending on the patient’s clinical condition. 28 The IWGDF/Infectious Diseases Society of America (IDSA) guidelines strongly recommended administering antibiotic therapy to a patient with a skin or soft tissue diabetic foot infection for 1–2 weeks mild and 2–4 weeks for moderate to severe infection. 6 The previous guidelines from the National Health Service (2020) recommended that a minimum duration of administering empirical antibiotics was 2–3 days. Then, microbiological examinations must be evaluated to change a narrow spectrum agent once a definite pathogen has been identified. 29 However, in our hospital, medical personnel occasionally used bacterial culture.
The consideration of using antibiotics also concerns the dosage. In our findings, six out of 41 antibiotic prescriptions were inappropriate dosage (14.63%), which included category IIa. Inappropriate use of neither Levofloxacin 500 mg every 24 h nor Meropenem 200 mg every 24 h was associated with lower plasma concentration. Levofloxacin was a class of antibiotics with a concentration-dependent 0–24 h [area under curve (AUC)0-24]/minimum inhibitory concentration (MIC) pharmacodynamic.30, 31 In other words, the effectiveness of this antibiotic was to maximize the dosage. The route of administration was intravenous 85.71%, which is based on the onset of action and its effectiveness. Intravenous antibiotics were typically administered to patients with moderate to severe infections. 32 In addition, intravenous treatment is necessary in cases where the patient is unresponsive, unable to swallow, dehydrated, or in shock. 33 This allows antibiotics to be delivered to affected tissues directly into the systemic circulation. 34 The total LOS for DFU patients was 320 days, with an average of 8.15 days, indicating that they spent approximately 8–9 days in the hospital. The severity of the disease, concurrent disorders, and Wagner stages of the patients could have influenced LOS, but these factors were not discussed in this study. 35
Limitations
This study was based on an analysis of antibiotic prescriptions, particularly for 1 year and it did not include a quantitative evaluation.
Conclusion
The utilization rate among antibiotics for the treatment of DFU was deemed inappropriate. To guarantee that prescribed antibiotics are highly appropriate for the patient’s condition and illness, it is also necessary to perform a bacterial culture before deciding on the mode of administration. Consequential compliance with the antibiotic therapy regimen with treatment guidelines and the accuracy of the diagnosis of DFU by medical personnel in the Roemani Muhammadiyah Semarang Hospital ICUs. For further research, the data period should be collected from the last 5 years and include a quantitative evaluation of antibiotic use.
Abbreviations
AUC: Area under the curve; DFU: Diabetic foot ulcers; ICD 10: International Classification of Diseases, Tenth Revision; ICU: Intensive care unit; IDSA: Infectious Diseases Society of America; IQED-Foot: Initiative for quality improvement and epidemiology in multidisciplinary diabetic foot clinics; IWGDF: International working group on the diabetic foot; LOS: Length of stay; MIC: Minimum inhibitory concentration; MRSA: Methicillin-resistant Staphylococcus aureus; RCT: Randomized controlled trial; SIRS: Systemic inflammatory response syndrome.
Footnotes
Acknowledgments
The authors would like to thank STIKES Telogorejo Semarang, specifically Lembaga Pendidikan and Penelitian dan Pengabdian Kepada Masyarakat, for their continued support and encouragement of the program.
Author Contributions
G.R. Al Farizi and A.A.P. Paramita conceived and designed the study. F. Gloria and D. Karlina performed data processing and Gyssens analysis. G.R. Al Farizi provided the funding. E.B. Astuti collected data from patients’ medical records. G.R. Al Farizi revised the manuscript. All authors have read and approved the manuscript and have made significant contributions to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was approved by the health research ethics committee at Roemani Muhammadiyah Semarang Hospital (reference number EA-008/KPEK-KSR/VII/2023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.