
Abstract
Introduction
Topical corticosteroids are currently the primary drugs to treat several dermatological disorders. But they are misused for various indications such as acne, pigmentation, fungal infection, and pruritus, and many times as a cosmetic or a skin cream for any type of rash. This study is performed to compare the magnitude of adverse events between practitioner-prescribed and self-prescribed groups of patients. In addition, this study also focuses on the demographic and educational status of patients where topical steroids are most widely misused.
Materials and Methods
It is a cross-sectional, hospital-based observational study conducted in the Department of Dermatology in collaboration with the Department of Pharmacology, KIMS, Bhubaneswar. A total of 134 patients were enrolled after getting the informed consent for the study, and assessed based on their topical steroid misuse and their adverse effects.
Results
The present study showed that steroid misuse was most common between 20 and 30 years of age group patients with low educational status. The most commonly applied steroid was clobetasol followed by mometasone and steroid abuse was more common in self-prescribed patients than physician-prescribed patients. The economic burden was more in the case of people using steroid cream only or steroid + anti-fungal creams because they have to be applied over a large body surface area. Incidence of adverse effects was observed more in self-prescribed patients and with low educational status.
Conclusion
This study highlights the fact that self-medication increases the incidence of adverse reactions and economic burden on the patients. Continuous education of patients and strict regulations regarding over-the-counter sales of steroids may help decrease the incidence of steroid misuse.
Introduction
Topical corticosteroids (TCS) have greatly contributed to the dermatologist’s ability to effectively treat several difficult dermatoses. 1 These are available in the form of creams, ointments, gels, solutions, and various other vehicles. 2 The common indications are conditions such as psoriasis, lichen planus, eczema, lichen simplex chronicus, and other steroid-responsive dermatoses. 3 Apart from their anti-inflammatory property, they possess additional clinically valuable properties like antipruritic, immunosuppressive, and melanogenic, etc. 2
Therefore, they are misused for various indications such as acne, pigmentation, fungal infection, pruritus, and many times as a cosmetic or a skin cream for any type of rash. 3 Poor health infrastructure, lack of adequate specialist services, the practice of self-medication, affordability, and easy access over-the-counter (OTC) have resulted in widespread abuse of TC. The problem of adverse effects has, however, become a huge concern due to the rampant misuse of TC, particularly by non-dermatologists. 4 Also, there is a tendency to reuse old prescriptions for a recurrent or new rash. Prescription sharing with relatives and friends on the presumption that similar-looking skin problems can be self-treated by simple prescription copying is rampant. 1
Ironically, the Indian market is flooded with several fixed-dose combinations of corticosteroids with anti-bacterial and fungal agents, which in no way can be considered scientific and rational. 5 Apart from producing undesirable adverse effects, inappropriate TCS use can mask clinical signs of underlying diseases causing diagnostic dilemmas and delays in treatment. 6 TCS abuse becoming a great cause of concern for their dramatic clinical effects, peer pressure to use them for cosmetic purposes, easy availability of products, inadequate information of their adverse effects, and the phenomenon of steroid addiction. 7
Many studies are published in literature focusing on a similar problem but to our knowledge, none of them have compared the adverse events occurring in patients who are using topical steroids on their own or have been prescribed by practitioners which makes our study unique and novel. The present study is designed to compare the magnitude of adverse events between practitioner-prescribed and self-prescribed groups of patients. Furthermore, this study aims to focus on the demographic and educational status of patients where topical steroids are most widely misused.
Study Objectives
Primary Objective
To compare the incidence of adverse events in terms of incidence and severity caused by topical steroid misuse amongst practitioner-prescribed and self-prescribed groups of patients.
Secondary Objectives
To identify different indications for which topical steroids are most commonly prescribed or misused.
To assess the demographic and educational status of patients.
To compare the economic burden in both groups.
Materials and Methods
It is a cross-sectional, hospital-based observational study conducted in the Department of Dermatology, Venereology and Leprosy outpatient department in collaboration with the Department of Pharmacology, Kalinga Institute of Medical Sciences in the period of April 2022 to September 2022. This study was approved by the Institutional Ethics Committee (IEC) No. KIIT/KIMS/IEC/875/2022. A total of 134 consecutive patients were enrolled who had satisfied the inclusion and exclusion criteria after getting the informed consent. They were assessed based on their topical steroid misuse and their adverse effects.
Inclusion Criteria
Patients of the age group between 10 and 65 years.
Patients of both sexes (males and females).
Patients using topical steroids for a minimum of four weeks period, either continuously or intermittently.
Exclusion Criteria
Patients with comorbidities that can cause changes similar to adverse effects of topical steroids, e.g., polycystic ovarian syndrome, Cushing syndrome, chronic alcoholics, and depression.
Patients who have consumed oral steroids in the last one month or continuing.
Clinical performance was given to all the included patients and details regarding their demographic profile, complaints, adverse event description, educational profile, economic burden due to steroid misuse, and other important details were obtained by the patients, and the data collected was further analyzed using required statistical methods. All statistical analysis was performed by using IBM SPSS version 25 software. Categorical variables were described by frequency and percentage, whereas continuous variables were presented by median and interquartile range (IQR). The association among all the categorical variables was accessed by the chi-square test. Statistical significance was defined by p < .05.
Results
A total of 134 patients including 72 females (53.73%) and 62 males (46.27%) were recruited in the study. The patient’s baseline characteristics are summarized in Table 1. The median age was 28 years (IQR: 24–37) and the median average duration of steroid use was four months (IQR: 2–6.25). It was observed that clobetasol was applied by 48 patients (35.82%), mometasone by 34 patients (25.37%), beclomethasone by 19 patients (14.18%), betamethasone by 13 patients (9.7%), fluocinolone by 9 patients (6.72%), halobetasol by 8 patients (5.97%), and desonide by 3 patients (2.24%).
Demographic Characteristics of the Patients Using Steroids.
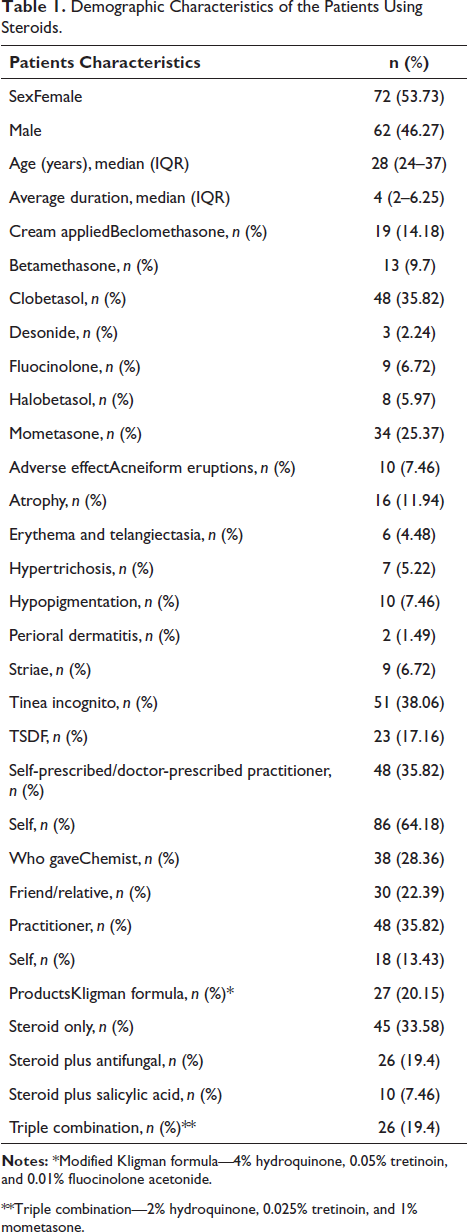
**Triple combination—2% hydroquinone, 0.025% tretinoin, and 1% mometasone.
It was seen that 38% of patients had tinea incognito and 17.16% of patients complained of TSDF (topical steroid damaged/dependent face) as an adverse effect after steroid application. Atrophy was seen in 11.94% of patients while 7.46% of patients had acne from eruptions and hypopigmentation as adverse effects.
A total of 86 patients (64.18%) were taking medicine without any formal prescription while 48 patients (35.82%) were taking medicine on advice of the registered medical practitioner. Out of self-prescribed patients, 38 patients (28.36%) were taking the drug on the local chemist’s advice, 30 patients (22.39%) took the drug on advice from their friends or family and the rest 18 patients (13.43%) had taken the drug on their own.
From all the products, 45 products (33.58%) were steroid, 27 (20.15%) were Kligman formula, 26 of them (19.40%) were steroid plus anti-fungal, 26 of them (19.40%) were a triple combination and 10 of them (7.46%) were steroid plus salicylic acid (Table 1).
Table 2 shows that most of the patients who are taking steroids without the advice of the physician belong to higher educational status and suffer from a greater incidence of adverse drug reactions (ADR) as compared to the physician-prescribed group, which is statistically significant (p < 0.05).
Association of the Adverse Effects and Educational Status Between Practitioner-prescribed and Self-prescribed Groups of Patients.
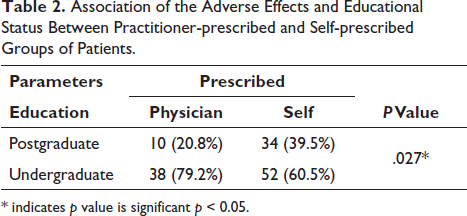
* indicates p value is significant p < 0.05.
Table 3 depicts that out of all the patients, 78 patients were in Grade 2 of severity and 56 patients were in Grade 3 of severity. Overall different types of cream that have been applied by the patients had no significant association between the severity of grades. None of the patients had Grade 1 severity, 35.9% of patients were in Grade 2 who were using only steroids while only 30.4% of patients were in Grade 3 who were using that. Similarly, 30.4% of patients were in Grade 3 and 11.4% of patients were in Grade 2 who were using triple combination which is statistically significant (p = 0.030).
Association Between the Creams Applied and Severity of Grade.
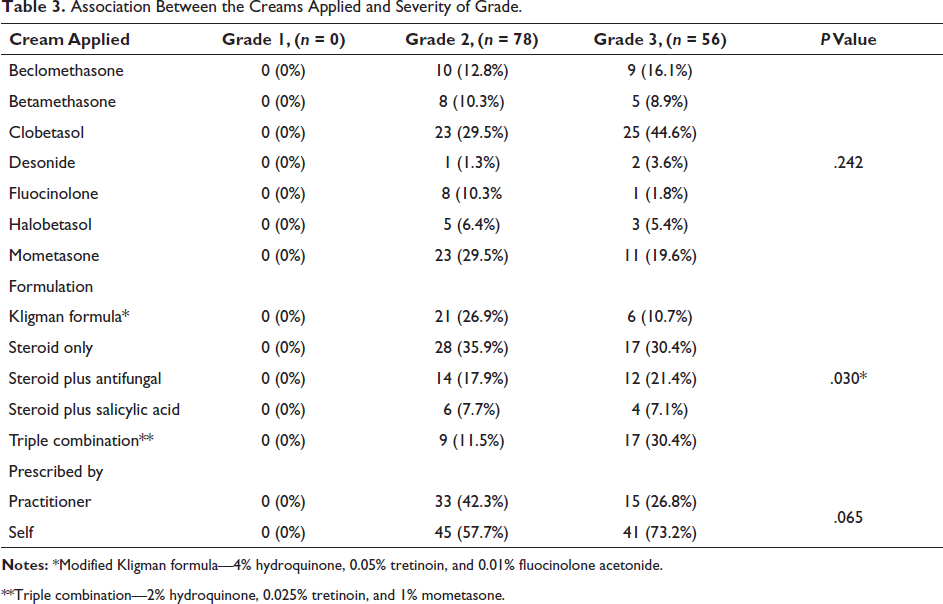
**Triple combination—2% hydroquinone, 0.025% tretinoin, and 1% mometasone.
Table 4 shows that the economic burden was more in patients using steroid only and steroid plus antifungal ointment.
Total Money Spent on Various Steroid Ointments.
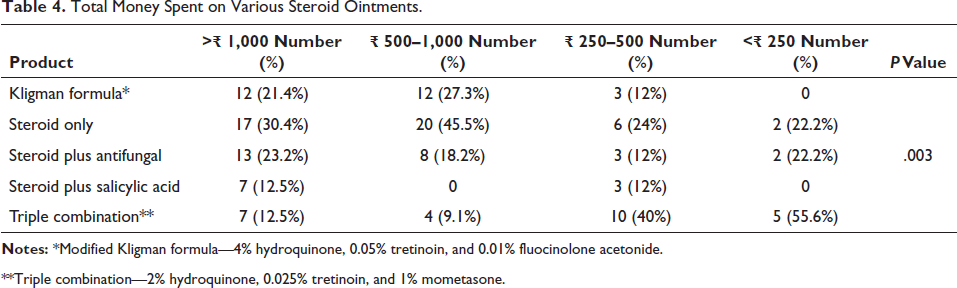
**Triple combination—2% hydroquinone, 0.025% tretinoin, and 1% mometasone.
Discussion
Topical steroids are commonly prescribed drugs for autoimmune and dermatological conditions because they have immunosuppressive, anti-proliferative, and anti-inflammatory actions. Steroids are currently the most preferred drugs in the dermatological clinics. However, reports suggest that these drugs are often misused. 8 Patients have reported various adverse effects including atrophy, striae, telangiectasia, hypertrichosis, and acneiform eruptions. Such adverse effects are commonly seen in off-label use or self-medication of topical steroids. Sometimes, the adverse effects could be more serious and cause systemic effects due to hypothalamo-pituitary axis suppression. 9 Most of the patients get guided by their relatives, pharmacy store sellers, or the advertisements coming on television and start using topical steroids without proper knowledge about the indications and adverse reactions. Studies suggest that steroids are commonly used for the topical treatment of dermatophytosis. Even for bacterial infection, acne, or minor rash, topical steroids are used by the patients. Such drugs are commonly available at the pharmacy store and are dispensed without a prescription. 10 These drugs can be refilled multiple times without a prescription or by using an old prescription. All these factors have contributed to the abuse of topical steroids. Though topical steroids have anti-inflammatory properties but they also possess anti-pruritic, anthropogenic, melanogenic, sex-hormonal, and immunosuppressive effects on the skin, causing various adverse effects. 11
It is always advisable to use topical steroids on the advice of a registered medical practitioner. There are many factors that need to be considered before prescribing these drugs like efficacy and potency of the drug, local site of application, age of the patient, indication, and duration for which the drug is prescribed. 12 Long-term application of these topical steroids in vulnerable age groups has caused serious consequences in the past. There are various studies that have highlighted the adverse effects caused because of the misuse of steroids. This problem is spreading rapidly and is a matter of concern for dermatologists.
The present study was conducted in the Department of Dermatology, Venereology and Leprosy outpatient department and was done in collaboration with the Department of Pharmacology, KIMS, Bhubaneswar. A total of 134 patients were enrolled in the study, out of which 72 were female and 62 were male. The median age was 28 years and the median average duration of steroid use was four months. Most topical steroid abusers in our study were between 20 and 30 years of age which is similar to some studies done in Iraq and Africa.13, 14
It was seen in this study that the most commonly applied steroid was clobetasol (35.82%) followed by mometasone (25.37%), beclomethasone (14.18%), betamethasone (9.7%), fluocinolone (6.72%), halobetasol (5.97%), and desonide (2.24%). Amongst these, 64% of the patients were using these topical medications without any prescription while 36% were using them on advice from a registered medical practitioner. The most common ADR reported was tinea incognito (38%), followed by TSDF (17.16%). Atrophy was seen in 11.94% of patients while acneform eruptions and hypopigmentation were seen as adverse effects in 7.46% of patients. These adverse effects were more common in self-prescribed patients (64%) than physician-prescribed patients (36%). The self-prescribed group patients generally take advice from their relatives, friends, and chemists or get influenced by various advertisements. This indicates the easy availability of these topical steroids in the pharmacy. Lack of knowledge and irresponsible intake of drugs on the advice of pharmacists, relatives, etc. causes disastrous complications in the patient. This problem is gradually increasing in India and becomes more difficult when such topical steroids are used as cosmetic agents to treat acne or as fairness creams. Studies have reported such type of misuse, not on India but also in China, Russia, Iraq, and Nepal.13, 15–17 Also in the present study, clobetasol is the most common steroid that was abused by the patients for various indications which is similar to a study done by Meena et al. 4 Whereas some other studies6, 7 by Khurana et al., and Inakanti et al. revealed that betamethasone is the most common steroid abused in their clinical settings. However, both are highly potent steroids based on their vasoconstrictive activity. Most of the patients in our study got relief of their symptoms just by stopping the respective steroid whereas few patients had to be treated with topical calcineurin inhibitors and oral doxycycline.
One major highlight of our study was the educational status of the patients in which misuse of topical steroids is seen. It was observed that amongst 86 patients in the self-prescribed group, 52 were undergraduate and 34 were graduate or postgraduate while in physician prescribed group, 38 were undergraduate and 10 were graduate or postgraduate. Hence there was a significant difference found in the abuse of topical steroids, based on education status. Patients with poor educational status (less than graduate) had more tendency to steroid abuse causing more incidence of adverse effects in such patients.
In our study, the most common indication of steroid use was tinea corporis followed by fairness and removal of pigmentation which is similar to a study done by Meena et al. 4 whereas some other studies7, 13 (Inakanti et al., Al-Dhalimi et al.) showed fairness achievement was the most common indication for steroid use. In tinea corporis, the steroid is generally combined with the antifungal drug in the ointment and provides immediate relief in the inflammatory symptoms of the disease. Steroids are often combined with bleaching cream for more fairness, which is unethical and causes several adverse effects.
It was also observed in the present study that topical steroids alone were the most common preparation used by patients in our study followed by steroids combined with antifungals and antibiotics. This finding is similar to the study done by Jha et al. 12 where 43.4% of patients used topical steroid preparations alone. Our study also highlights that a greater magnitude of damage is caused by steroids alone preparations where 34.2% of patients fall under the Grade 2 category and 30.4% of patients fall under the Grade 3 category of severity. None of the patients had Grade 1 severity. 18 In the case of patients using triple combination, 30.4% of patients were in Grade 3 and 11.4% of patients were in Grade 2 severity which is statistically significant.
The rampant use of steroid and steroid plus formulations has also increased the economic burden amongst the patients. This financial burden also poses a psychosocial impact on the patients. In our study, it was observed that economic burden was more in the case of people using steroid cream only or steroid + antifungal creams because they have to be applied over a large body surface area, and on the other hand, it reoccurs more frequently than the treatment used for pigmentation. More multicenter studies with greater sample sizes are required to derive correct data regarding the financial impact of the use of these topical steroids. That data will be required to drive policy-level interventions to curb the menace of topical steroid misuse, which is the need of the hour.
This study will enlighten the magnitude of adverse events and economic burden on patients due to self-medication. It will create awareness about the adverse events of topical steroids amongst medical practitioners and the general public. This study may help the regulatory authority to keep a check and prohibit the counter availability of topical steroids.
Conclusion
Topical steroids are commonly prescribed for many conditions and misuse of TCS has a huge impact on the health status of society. The misuse is self-prescribed mostly, increases the financial burden of the patient, and leaves a deep impact on clinical practice. The present study showed that steroid abuse was more common in self-prescribed patients than in physician-prescribed patients. Also, patients with lower educational status had more tendency to steroid abuse causing more incidence of adverse effects. Economic burden was also more in patients using only steroid and steroid antifungal topical preparations. Hence, this study highlights the fact that self-medication increases the incidence of adverse reactions and economic burden on the patients. Continuous education of patients by clinicians and strict regulations regarding the OTC sale of these topical formulations may help decrease the incidence of steroid misuse.
Footnotes
Abbreviations
Acknowledgments
Staff of Department of Dermatology and Pharmacology, KIMS Hospital, Bhubaneswar.
Authors’ Contributions
Dr. Laxman Besra: Concept, design, definition of intellectual content, literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review. Dr. Ratikanta Tripathy: Concept, design, definition of intellectual content, literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review. Dr. Vartika Srivastava: Concept, design, definition of intellectual content, literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review. Dr. Sakshi Gaba: Concept, design, definition of intellectual content, literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review. Mr. Sourabh Padhee: Data analysis, statistical analysis, manuscript preparation, manuscript editing, and manuscript review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical Approval was taken, and the Reference number is KIIT/KIMS/IEC/875/2002.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Patients included in the study have given their consent to participate in the study.