
Abstract
The difficult airway is already a challenging situation for anesthesiologists, in that scenario Succinylcholine (SCh) use, because of its rapid onset and short duration of action makes it a neuromuscular blockage drug of choice. Development of masseter muscular rigidity is thought to be an early indicator of the occurrence of the dreaded consequence, malignant hyperthermia. Consequently, it is essential to understand the potential side effects of this widely used drug in order to successfully treat the airway. Resulting is the use of videolaryngoscopic intubation along with propofol use and the procedure was completed successfully with no intraoperative or postoperative problems. Here, we described a case report of a 33-year-old male patient with a difficult airway posted for open reduction internal fixation of bilateral Lefort’s III fracture, developed masseter muscle rigidity (MMR) following administration of a standard dose of SCh.
Introduction
Succinylcholine (Sch), is a successful induction agent in facilitating challenging intubations. In rare cases, Sch may also cause major adverse effects such as masseter muscle rigidity (MMR), rhabdomyolysis, increased creatinine phosphokinase (CPK), and malignant hyperthermia (MH).
It makes muscles tenser at rest, with the masseter muscle being particularly more affected. Usually, it is observed as a common pharmacologic response. Masseter muscular rigidity caused by Sch is often momentary and resolves on its own, but it can occasionally last longer, as a noticeable stiffness of the jaw that scarcely permits any mouth opening.1–3
It increases the risk of MH resulting in significant morbidity and mortality among patients. Due to the hypermetabolism of skeletal muscle, Sch or volatile inhalational anesthetics can cause MH. 4 Malignant hyperthermia susceptibility (MHS) is inherited as an autosomal dominant factor. It is impossible to identify susceptibility without either exposure to triggering factors or by particular diagnostic tests because the majority of people with MHS appear normal and lack any clinical indicators. 5 Following case reflects how all necessary measures were taken to secure an adequate already difficult airway along with the perioperative strategy followed for maintaining the patient’s hemodynamic parameters.
Case Presentation
A 33-year-old male patient, 85 kg, was admitted with an alleged history of bilateral nasal bone and bilateral orbit bone trauma posted for open reduction and internal fixation of bilateral Lefort’s III fracture. He was Mallampatti grade IV, restricted mouth opening (4 cm), had a short neck, a thyromental distance of 6.5 cm, with normal temporomandibular joint mobility and dentition. Ophthalmology finding; diplopia was found on left lateral gaze, no history of head injury was present, and clinically, patient was hemodynamically stable with normal routine investigations. He had no medical illness, no past surgical history, or any muscular disorder family history.
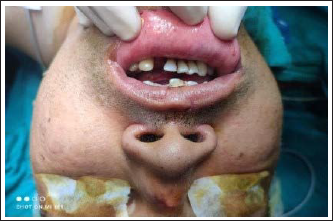
Difficult intubation trolleys and emergency drugs were made available in the operation theatre along with the video laryngoscope if required. After securing an 18 G IV wide bore cannula, the patient was premedicated using injection (IV) glycopyrrolate 0.2 mg, 1 mg midazolam (IV), and butorphanol 1 mg (IV). 120 mg IV propofol was used for induction after pre-oxygenating the patient with 100% oxygen for 4 min. After adequate bag-mask ventilation, muscle relaxant Sch 100 mg (IV) was given. After the disappearance of fasciculations, during the laryngoscopy procedure, it was observed that the mouth became impossible to open fully, insertion of laryngoscopy was found to be very difficult, and clenching of teeth occurred. After a few minutes, laryngoscopy was again tried, but it failed. The patient continued to be mask ventilated with 100% oxygen. The development of masseter muscle spasm was thought to be the reason, and hence the use of any other anesthetic agent was avoided (Figure 1). No increase in EtCO2 or body temperature was found throughout this time. After 5 min of mask ventilation and maintenance of oxygen saturation at 100%, the patient’s respiration pattern improved, and he began to breathe spontaneously. He was then administered inj. Propofol 40 mg (IV) bolus along with inj. Atracurium 15 mg IV. The jaw was seen relatively relaxed now, but due to difficult laryngoscopy, as the patient has already restricted mouth opening pre-operatively, a videolaryngoscopic approach (king vision) was used for intubation. An endotracheal cuffed tube (No. 8) was used for intubating the patient. Then the patient was catheterized to monitor urine color and output, in view of the possibility of the development of overt MH and further myoglobinuria-like complications.
Inhalational anesthetic agents were avoided; the patient was maintained throughout surgery on propofol infusion at the rate of 100 µg/kg/min and on muscle relaxant atracurium along with nitrous oxide and oxygen. As a resuscitation measure, one more 18G wide bore cannula was secured, adequate amount of IV fluids and ringer lactate was given intraoperatively. Meanwhile, the temperature was frequently checked intra-operatively, and careful monitoring of vitals was carried out to prevent a sudden increase in heart rate, blood pressure, and abnormal ECG changes. The patient was afebrile throughout the surgery. The urine was clear, and the output was also adequate. The patient’s vitals were stable during the entire surgery. At the end of the surgery neostigmine 2.5 mg was used as a reversing agent. The patient’s respiratory efforts were adequate to maintain a good tidal volume and adequate muscle power. He was kept under observation for one more hour after extubation to assess his mouth opening, jaw movement, and muscle tone. It was found that the jaw became completely relaxed as it was in the pre-operative period. SCh-induced MMR diagnosis was confirmed. The patient was shifted to the intensive care unit post-operatively to observe any further risk of developing MH. Post-operatively ABG was found to be within the normal range (pH 7.4), mildly raised K+ 5.8 meq/l, and other routine laboratory investigations were repeated and found to be in the normal range. The post-operative period was found to be uneventful, and on the third day, the patient was discharged.
Discussion
The MMR, often referred to as the “steel-jaw”, becomes so rigid that mouth opening becomes restricted due to an increase in muscular tone.6,7 A prolonged increase in muscle tone, particularly in the jaw muscles, may occur in some genetically susceptible patients, making it difficult to open the mouth for laryngoscopy and endotracheal intubation. 8
An important contributor to anesthesia-related morbidity and mortality is intubation failure. Therefore, a quick solution for this clinical conundrum is required. Even though Sch-induced masseter muscle stiffness occasionally lasts longer, it often subsides quickly, as seen in this case. 9 Although intubation was difficult, bag-mask ventilation was continued to be done to prevent desaturation. The need for pre-oxygenation during rapid sequence intubation and the requirement for a backup strategy in the event of an airway failure is highlighted by this case report. Depending on the patient’s state and the availability of videolaryngoscopes (king vision, c-mac), various airway-sealing procedures, including Laryngeal mask airways, nasal intubation, or retrograde mode of endotracheal intubation may be performed if endotracheal intubation is unsuccessful. Surgeries like tracheostomy with cricothyroidotomy may be utilized as an end option. 10
In our case, when SCh effects had worn off, a second bolus dose of propofol was administered, and then the jaw was given a certain time to relax. Propofol is allegedly more successful at reducing tension in the masseter muscle when used as an induction agent. 11 It is the favored anesthetic due to its various benefits in these situations. It can be used to maintain anesthesia, it relaxes the muscles of the jaw, and it works as an MH trigger-avoiding medication. As a result, employing propofol as an induction agent along with videolaryngoscope use, intubation was possible in the patient with an already difficult airway.
Intubation issues frequently arise, particularly when the airway is constrained. New laryngoscopes come with digital technology that improves visibility, decreases the requirement for tissue manipulation, and makes it simpler to examine the anterior airways in case of airway difficulties12,13
High fentanyl doses are regularly known to cause rigidity in non-paralyzed individuals. In order to reduce the risk of muscle rigidity or stiffness, butorphanol was employed in our case as an analgesic instead of fentanyl. 14 MMR has reportedly been linked to MH, aside from interfering with oral intubation. According to the literature, the overall incidence of MH is 1:15,000 in children and 1:40,000 to 1:50,000 in adults. 15 A mutation in the sarcoplasmic reticulum (SR), a calcium release channel is the most common cause of MH (ryanodine receptor). The SR calcium channels frequently open during an MH episode, enabling calcium to enter the body. Resulting in hyperthermia, prolonged muscle contraction, and an elevated metabolism, all of which have a significant risk of death. 16 The decision to proceed with the surgery or not will depend on its urgency and the level of muscular rigidity. 17
Therefore, it is crucial to take the risk of MH into account in patients who experience significant masseter spasm after receiving Sch.
Atypical calcium homeostasis in skeletal muscle in response to trigger compounds is the main part of the pathophysiology of MH. Increased aerobic and glycolytic metabolism brought on by persistently elevated Ca++ levels in the SR causes acidosis, stiffness, rhabdomyolysis, myoglobinuria, hyperkalemia, hyperthermia, and hemody-namic instability. The initial indication of MH when the patient is under general anesthesia is an increase in EtCO2, which is out of proportion to the clinical context. 18
In our situation, since the patient was afebrile, EtCO2 remained normal, the patient’s vital signs were stable, the urine was clear throughout, and the K+ level was only slightly increased. No indications of MH were found during the clinical assessment. In this circumstance, it was fortunate that ventilation was maintained using a bag-valve mask and that a definite airway could then be created orally with the use of a videolaryngoscope. For the treatment of masseter muscular rigidity, atracurium, a non-depolarizing muscle relaxant, and propofol were administered.
MMR typically occurs 20 to 30 min before the onset of MH symptoms. 19 As a result, some authors had advised refraining from surgical procedures following an MMR and instead looking for signs of MH in the patient.
Berry and Lunch, 20 suggested performing the procedure while closely monitoring for MH symptoms. If the EtCO2, ABGs, BP, HR, temperature, serum CPK, urine color, and muscle tone are all within normal ranges, the anesthesia can be maintained by avoiding inhalation agents to lower the risk of acquiring MH. There were no initial signs of MH, so we decided to continue the surgery while carefully scanning for any signs of MH. We maintain the anesthesia with propofol infusion. This might be the reason why the MMR was unable to reach the MH stage. The patient’s EtCO2, ABGs, temperature, and urinalysis were unremarkable, and the slightly elevated serum potassium levels supported the isolated MMR diagnosis. Patients who have a prior history of MMR episodes should be advised to stay more careful regarding the development of complications associated with it.
Conclusion
This case report highlights that a single MMR instance could lead to the possibility of failed laryngoscopy and failed intubation event. Any feasible technique that can open the airway must be quickly considered, and vital signs should be closely watched both before and after the operation while keeping the possibility of MH. The preservation of anesthesia should also include avoiding MH stimuli. Additionally, appropriate instruction and counselling regarding the dangers of future trigger-producing substances should be given to the patients.
Footnotes
Acknowledgment
Constant support provided by Dr. Aruna Chandak for preparing the manuscript is gratefully acknowledged. Dr.Priyanka Dev and Dr. Aditi Prafulshatalwar are acknowledged for their valuable suggestions and ideas.
Abbreviations
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained prior to performing the procedure, including permission for publication of photographs.