
Abstract
Objectives
To compare the attenuation of pressor responses by intravenous clonidine and preservative-free lignocaine to laryngoscopy and endotracheal intubation.
Materials and Methods
A randomized, prospective, comparative, double-blinded study was conducted in 80 adult patients who were randomized into two groups of 40 each, group clonidine (Group C) and group lignocaine (Group L). Group C patients were given 2 µg/kg clonidine in 20 ml of normal saline as a slow infusion over 10 min prior to intubation. Group L patients were given 1.5 mg/kg of preservative-free 2% lignocaine in 20 ml of normal saline as a single-dose infusion over 3 min prior to intubation. Baseline vital and hemodynamic parameters were monitored during the perioperative period at 1-, 5-, and 10-min post-intubation.
Results
The attenuation of heart rate (HR) after intubation was much better with clonidine than lignocaine as there is statistically significant difference in the mean HR between the two groups at 1, 5, and 10 min after intubation with the HR significantly lesser in the Group C than the Group L at all times after intubation. Both clonidine and lignocaine were effective in attenuating systolic blood pressure response after intubation, but clonidine was more effective than lignocaine as systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial pressure (MAP) in the Group C remained much lower than the Group L and the difference between the two groups was statistically significant at all times after intubation.
Conclusion
Premedicating with a single slow infusion of 2 µg/kg i.v. clonidine has been proven to be effective in maintaining perioperative hemodynamic stability at 1, 5, and 10 min post-intubation than lignocaine.
Introduction
Hemodynamic pressure responses to laryngoscopy and endotracheal intubation were first elucidated by Reid and Brace in 1940. 1 Laryngoscopy and endotracheal intubation are considered as one of the most painful procedures carried out on the human body.2–5 The pressor responses that may occur during direct laryngoscopy and tracheal intubation are customarily transient and variable6–9 and these responses occur approximately 30 s after the initiation of laryngoscopy and intubation and lasts for almost 10 min post-intubation. 10
Over the years, various pharmacological and non-pharmacological methods have been followed for minimizing the hemodynamic responses to laryngoscopy and endotracheal intubation. 11
Clonidine is an alpha-2 adrenergic receptor agonist and is an imidazole derivative. Preservative-free intravenous local anesthetics such as lignocaine can also be used as an agent to suppress the stress response to laryngoscopy and intubation 12 and is one of the cheapest drugs available for this purpose. Several authors13, 14 concluded that lignocaine in a dose of 1.5 mg/kg suppresses the stress response to intubation when given 3 min before intubation.
Keeping in view this background of both the drugs, a randomized, prospective double-blinded study was carried out to compare the effect of clonidine 2 µg/kg and preservative-free lignocaine 1.5 mg/kg in attenuating the pressor response during laryngoscopy and endotracheal intubation.
Methodology
A randomized, prospective, comparative, double-blinded study was conducted after approval of the institutional ethics committee. The study was conducted for 6 months in the Department of Anesthesiology and Critical Care of Dr. D.Y. Patil Medical College, Hospital and Research Centre, Pimpri, Pune, India. We calculated the sample size using the fluctuations in the hemodynamic parameters as 106.00 ± 20.62 (group 1: 1.5 mg/kg of lignocaine) and 94.25 ± 14.72 (group 2: 2 µg/kg of clonidine) at T3 after intubation. The calculated sample size was 80 and was divided into two groups equally, with an acceptable difference of 10% and a 95% confidence level.
Eighty patients of the age of more than 18 years belonging to American Society of Anesthesiologist (ASA) grade I and grade II, hemodynamically stable and posted for elective surgeries under general anesthesia requiring intubation were included in the study (Figure 1). A written informed consent was taken from all study subjects. We excluded patients with any pre-existing cardiovascular disease, with a history of allergy to test drugs, patients posted for emergency surgeries and with difficult airways. We also excluded patients with neurological disorders and muscle diseases.
Consort Flow Diagram Depiction of the Study.
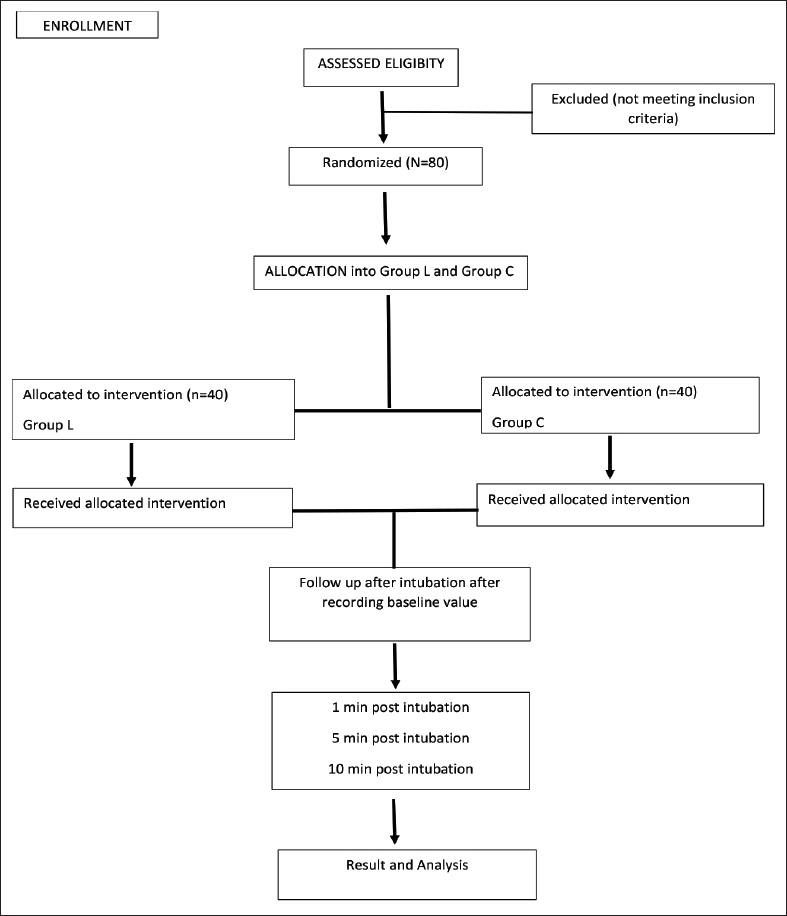
Allocation sequence is generated by a computer-generated random number table, where a total of 70 patients are divided into five blocks, containing 14 patients in each block. The random allocation sequence generation and group allocation were done by an anesthesiologist who was unaware of the study protocol and did not participate in the study. Participants were enrolled for the study by the investigator. The patient and investigator were not aware the of drugs given. The drugs were prepared and administered by the theatre anesthesiologist, who was not part of data collection or analysis. All patients were premedicated with alprazolam 0.5 mg per oral (p.o.) and ranitidine 150 mg p.o. on the previous night 10 p.m. and patients were kept nil by mouth (NBM) after 10 p.m. Patients were prepared by securing a 20-gauge intravenous (IV) cannula, applying basic monitoring like pulse oximeter, standard five-lead electrocardiography (ECG) and non-invasive blood pressure.
Eighty patients were divided into two groups:
Group C (n = 40): received i.v. 2 µg/kg clonidine. Group L (n = 40): received i.v. 1.5 mg/kg preservative-free 2% lignocaine.
After premedication with injection ondansetron 4 mg i.v., injection glycopyrrolate 0.004 mg/kg i.v., injection midazolam 0.02 mg/kg i.v., and injection fentanyl 2 µ/kg i.v. in both the groups, Group C, and Group L received the above-mentioned drugs in the mentioned doses and particular time. The patient was induced on propofol 2 mg/kg i.v. and along with succinylcholine 2 mg/kg i.v. as short acting muscle relaxant. Laryngoscopy and intubation was done using appropriate size blades and cuffed endotracheal tube respectively. The patient was maintained on oxygen and nitrous oxide along with sevoflurane. The patient was given injection vecuronium 0.1 mg/kg i.v. as long-acting non-depolarizing muscle relaxant.
At the end of the surgery, neuromuscular block was reversed by giving neostigmine (0.05 mg/kg) i.v. and glycopyrrolate (0.008 mg/kg) i.v. and following which the patient was extubated after acquirement adequate muscular tone. Any side effects like hypotension, nausea, vomiting, bradycardia, hypertension, arrhythmias, hypoxia, bronchospasm, and blurred vision are watched out for and treated accordingly.
The data recorded were analyzed using the Statistical Package for Social Sciences (SPSS) 21.0 version. The associations were evaluated with the use of Student’s t-test for quantitative variables and χ 2 tests for categorical variables. A p value of less than 0.05 was considered significant.
Results
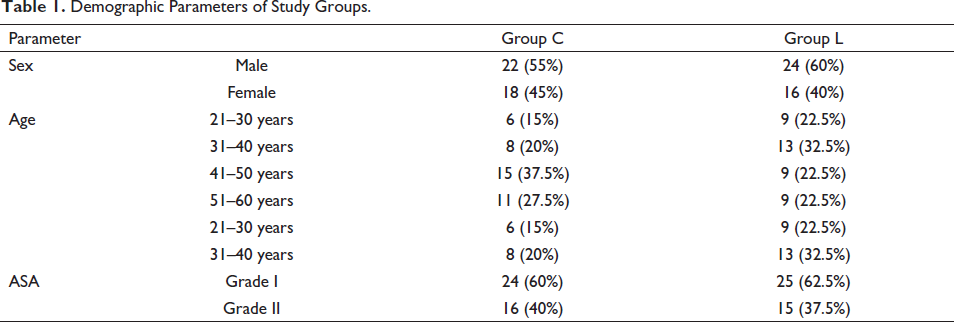
Both groups were comparable with respect to age, gender, ASA distribution (Table 1). Furthermore, there was no significant difference between the two groups with respect to baseline systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial pressure (MAP). As seen in Table 2, in both Group C and Group L, mean HR started to decrease below the baseline after intubation and remained lower than baseline throughout, with the maximal drop in HR in Group C (8.13%) compared to Group L (7.99%) at 10 min after intubation. When the two groups are compared, there is a statistically significant difference in the mean HR between the two groups at 1, 5, and 10 min after intubation with the HR significantly lesser in Group C than Group L at all times after intubation and thus proving that the attenuation of HR post-intubation was much better pronounced with clonidine (Group C) than with lignocaine (Group L).
Demographic Parameters of Study Groups.
Vital Parameters Distribution in Two Groups.
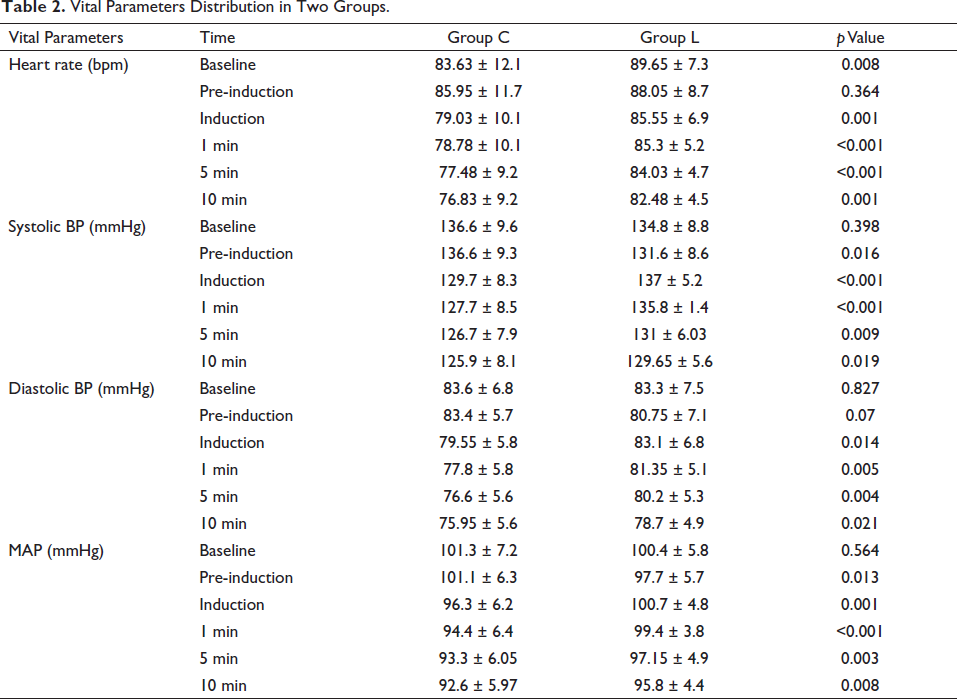
In Group L, SBP, DBP, and MAP started to increase from the baseline at 1 min after intubation, and although it slightly reduced thereafter, SBP in Group C remained much lower than that in Group L. The difference between the two groups was statistically significant at all times after intubation. This clearly indicates that both clonidine and lignocaine are effective in attenuating SBP response after intubation, but clonidine is more effective than lignocaine (Table 2).
Discussion
Laryngoscopy and endotracheal intubation produce hemodynamic stress responses characterized by hypertension and tachycardia. 1 These neuroendocrine responses can cause a variety of complications in patients with cardiac disease due to an imbalance of myocardial oxygen supply and demand like ischemic changes, ventricular arrythmias, and cardiac failure.1, 2 This is also hazardous in patients with vascular pathologies due to weakening of lining of major arteries in particular cerebral and aortic aneurysms. In patients with hydrocephalus or intracranial mass lesions the increase in CSF pressure may produce transient impairment of cerebral perfusion leading to cerebral ischemia.
Adrenergic neurons, inhibitory in nature, which are present in medullary vasomotor centers, get stimulated by alpha-2 agonists, such as clonidine, and this property has been exploited recently to reduce sympathoadrenal stimulation produced by tracheal intubation.15, 16, 17 Although clonidine is primarily used as an antihypertensive, studies have shown that it can also be used to lessen hemodynamic reactions to laryngoscopy and intubation, especially when given intravenously rather than orally and at a dose of 2 µg/kg. 18
Oral clonidine (5 µg/kg) attenuated circulatory reactions to laryngoscopy and intubation, according to Batra et al., 19 oral clonidine does circumvent the response. The findings of this study are backed by earlier research by Ghignone et al. 20 and Pouttu et al. 21 When Zalunardo and Zollinger 22 compared intravenous clonidine (3 µg/kg i.v.) to intravenous esmolol (2 mg/kg i.v.) in attenuating intubation responses, they discovered that intravenous clonidine (3 µg/kg i.v.) was statistically significant (p = .05) in attenuating intubation reactions.
Various studies have reported that lignocaine is effective in blunting these responses. 23 Recent studies, however, have questioned lignocaine’s efficacy. Singh et al., 24 Van den Berg et al., 25 and Kindler et al. 26 found that lignocaine 1.5 mg/kg i.v. was ineffective in controlling the acute hemodynamic response following laryngoscopy and intubation. In our study, a comparison of clonidine (2 µg/kg i.v.) and lignocaine (1.5 mg/kg i.v.) was done in attenuating circulatory responses to endotracheal intubation.
The mean HR in Group C is significantly lower than Group L at all periods following intubation in this study, and this difference is statistically significant (p = 0.05). This is consistent with findings from previous studies by Vyankatesh et al., 27 Marulasiddappa and Nethra, 28 and Chatterjee et al. 29 by comparing lignocaine and clonidine for attenuation of hemodynamic response to laryngoscopy and intubation.
In this study, SBP at increased at pre-induction and decreased at induction, 1, 5, and 10 min after endotracheal intubation in clonidine group compared to lignocaine group. The diastolic blood pressure at induction, 1, 5, and 10 min after endotracheal intubation is statistically lower in clonidine group compared to lignocaine group. The mean arterial blood pressure increased at pre-induction and decreased at induction, 1, 5, and 10 min after endotracheal intubation in clonidine group compared to lignocaine group. The findings of our study are comparable to past researches such as those by Allam et al., 30 Chatterjee et al., 29 and Mohamed et al. 31 which denoted that clonidine was more potent in reducing SBP and DBP than lignocaine.
Limitations
The primary drawback of this study was that the test for stress mediators was not taken into consideration. Catecholamine levels in response to laryngoscopy and endotracheal intubation are said to be higher in central venous ample than that of peripheral or arterial samples. Central venous catheterization being an invasive procedure is unethical to be fixed in patients fit under ASA 1/II for surgery and hence not done.
Perioperative analgesia requirement and perioperative sedation scores were not included in our study. Effects of these drugs on elderly patients and patients with compromised cardiac function were not evaluated. So, it is strongly suggested that further studies required to overcome the above-said limitations to recommend its use in such high-risk patients.
Conclusion
Laryngoscopy and subsequent tracheal intubation induce a fugitive raise in the heart rate and blood pressure due to sympathoadrenal stimulation. Many modalities have been proposed and practiced for attenuating these deleterious pressor responses to laryngoscopy and intubation. It includes both pharmacological and non-pharmacological methods. In this study, we conclude that the attenuating effect of clonidine on the pressor response is far superior to lignocaine, both in controlling the heart rate as well as blood pressure.
Footnotes
Abbreviations
HR, Heart Rate; BP, Blood Pressure;
SBP, Systolic Blood Pressure;
DBP, Diastolic Blood Pressure;
MAP, Mean Arterial Pressure;
NBM, Nil by Mouth;
IV, Intravenous;
ECG, Electrocardiography;
CSF, Cerebrospinal Fluid;
ASA, American Society of Anesthesiologist.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Ethical committee approval was acquired (Research Protocol No. IESC/PGS/2020/143).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable