
Abstract
Objective
To assess the patterns and factors affecting medication use during antenatal and perinatal periods and to examine maternal and fetal outcomes among pregnant women admitted to a tertiary care hospital in a developing country.
Methods
A cross-sectional study was conducted in the obstetrics wards from 2017 to 2019. Data on patient demographics, co-existent medical conditions, medications, and patient outcomes were collected. Descriptive statistics were used to analyze baseline data, chi-square test was used for categorical variables, and multivariate logistic regression was used for factors influencing drug prescription.
Results
Out of 442 pregnant women, 56% were primigravida with a mean age of 24.7 ± 3.9 years. Approximately 32% experienced at least one disease condition during pregnancy; hypothyroidism (9.7%) was the commonest. The mean number of medications was 2.7 and 38.9% received drugs for a disease condition. Antimicrobials (24.5%) were the commonest drug class. Maternal age of over 25 [(OR (CI): 1.508 (1.191–2.716) (p = .005)] and maternal illness [OR (CI) 2.934 (1.8–4.7) (p = .00)] were identified as factors affecting drug prescription. Approximately 39.8% of deliveries were cesarean. Of the newborns, 12.6% had low birth weight, 9.2% were admitted to the newborn intensive care unit, and 14.9% were premature.
Conclusions
Most patients were primigravida and under 25 years. Antimicrobials were the most prescribed drug class. Maternal age over 25 years and maternal illness were identified as the factors affecting medication use. The prevalence of cesareans and prematurity was similar to previous studies.
Introduction
Pregnancy is an alteration of the normal physiological process requiring special and organized medical attention. Antenatal care is an organized medical service with the end objective of achieving the delivery of a healthy baby without impairing the health of the mother. The usage of medications during pregnancy is expected to help to achieve this outcome. The proportion of pregnant women receiving drugs excluding iron and folic acid during pregnancy varies from 38.4% to 61.8%.1, 2 This could be due to infections, hemorrhage, anemia, and pre-eclampsia arising as a result of pregnancy or due to an established illness of the mother that requires treatment. 3 Pharmacotherapy of these conditions can reduce perinatal morbidity and mortality.
However, pregnancy management using medications has been challenging for both healthcare providers and pregnant women due to the fear of teratogenic effects. For example, thalidomide which was given as a treatment for hyperemesis gravidarum was later found to cause phocomelia on exposure to the fetus during the first trimester. 4 Similarly, use of non-steroidal anti-inflammatory drugs (NSAIDs) during the first trimester increases risk of miscarriage and malformation (e.g., gastroschisis). 5
Besides teratogenicity, fetal vulnerability to drug pharmacodynamics and resulting toxicity is also a concern. Pharmacokinetics and pharmacodynamics vary during pregnancy. Factors that may alter pharmacokinetics and pharmacodynamics during pregnancy include changes in weight, body composition, pregnancies with multiples (e.g., twins, triplets), increased blood volume, and abrupt changes in behaviors such as alcohol and tobacco use.6–8
In order to optimize medical management during pregnancy and to guide safe drug use, the U.S. Food and Drug Administration (FDA) classified drugs into five major categories A, B, C, D, and X, with categories D and X indicating evidence of risk in pregnancy.9, 10
Extent of drug use during pregnancy is also not very well known. The maternal mortality in India has also remained high at 130/1,00,000 while in Karnataka it is 108/1,00,000 (2014–2016). 11 Studies which report the patterns and extent of medication use in pregnancy, maternal factors that influence medication use, together with the outcomes of pregnancy, are limited, especially from developing countries like India to the best of our knowledge. We searched using the MeSH terms pregnancy, drug utilization, determinants of prescription and outcomes in PubMed from 2000 to 2022.
The primary objective of the study was to study the patterns of medication use during antenatal period and evaluate the factors influencing drug prescription in pregnancy. The secondary objectives of the study were to describe the drugs prescribed during labor and postpartum period and to describe the neonatal and maternal outcomes observed.
Materials and Methods
A prospective, observational study was conducted from March 2017 to September 2019 in the obstetrics ward of an Indian tertiary care hospital after obtaining ethics approval (IEC reference number: 279/2016). All booked adult pregnant women (>18 years of age) coming to St. John’s Medical College Hospital, Bangalore, for labor were included. Pregnant women who did not have well-documented antenatal care were excluded.
Data was collected on the designed case record form (CRF). In addition, the following data were collected:
Outcomes for the baby: Apgar score, respiratory distress, birth weight, gestation status, and congenital anomalies.
In order to minimize selection bias, all consecutively admitted patients were recruited. In order to minimize measurement bias, clearly defined inclusion and exclusion criteria were established.
According to literature, the proportion of pregnant women receiving drugs (excluding iron and folic acid) during pregnancy varies from 38.4% to 61.8%.2, 3 Taking the proportion as 40% which was the median and assuming a precision of 5% and confidence interval (CI) of 95%, the required sample size was estimated to be 369. With dropouts estimated to be 20%, the estimated required total sample size was 442.
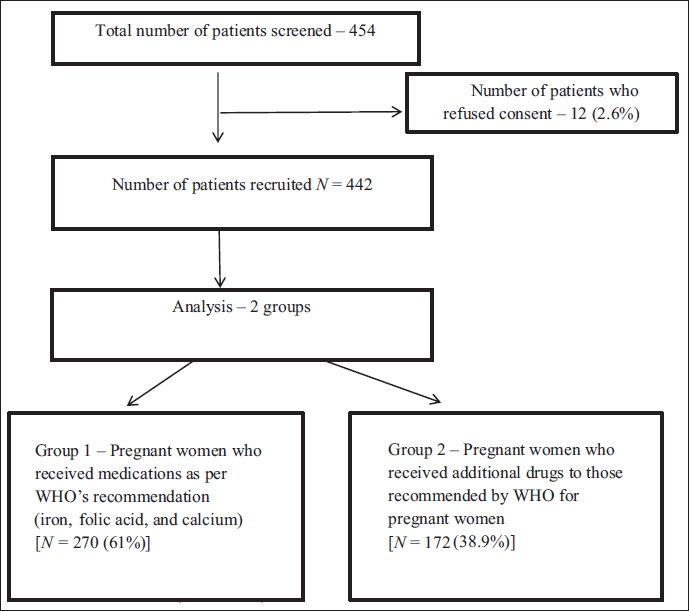
Thus, a total of 442 pregnant women were recruited into the study. Of these, 270 (61.1%) patients received only medications recommended by World Health Organization (WHO) for a normal pregnancy (iron, folic acid, and calcium) and 172 (38.9 %) received additional drugs. Figure 1 presents the flow of the study.
Flow of Study Participants.
Statistical Methods
To understand the factors associated with drug use, we divided the pregnant women into two groups—those who received the expected standard of care according to the guidelines of the WHO and those who received medications in addition to those that would usually be administered in the course of the expected standard of care. Chi-squared test was used to compare the characteristics of pregnant women who did and did not receive additional medications. Characteristics that were significant in univariate regression were further analyzed by multivariate logistic regression. A p-value under .05 was considered significant for all tests. Statistical analysis was performed using the commercially available software SPSS 16.0.
Results
Demographic Characteristics of Baseline Population
The mean age of participants was 24.7 (SD = 3.9) years. Of the total participants, 193 (44%) had a college degree, the majority resided in urban areas (69%), and 142 (32%) had a household income of over INR 45,000. Most of the women were homemakers (81%).
Obstetric Characteristics of Baseline Population
Approximately 56% of participants were primigravida. The majority had at least three or four antenatal visits with 39% having had more than four antenatal visits. Of the total number of participants, 113 (32%) had at least one disease condition during pregnancy, with the most common being hypothyroidism, seen in 42 (9.5%), followed by anemia in 40 (9%) of the participants. Other disease conditions included upper respiratory tract infections (6.7%), urinary tract infections (2.7%) and gestational diabetes mellitus (2.5%), hypertension (1.4%), HELP syndrome (0.2%), and systemic lupus erythematosus (0.2%).
Drug Prescription Patterns During Antenatal Period
The mean number of medications prescribed for each pregnant woman during the antenatal period was 2.68. About 172 pregnant women (38.9 %) received 285 non-standard drugs. Out of 285 drugs prescribed excluding standard-of-care medications, majority of the drugs belonged to FDA drug class B (66.6%), followed by FDA class A (16.8%), FDA class C (15.7%), and FDA class D/X (about 0.7%).10, 11
In the first trimester, 435 (98.4%) pregnant women received folic acid, 12 (12.7%) received thyroxine, 5 (1.1%) received progesterone, and 2 (0.5%) received paracetamol. Azathioprine, prednisolone, and hydroxychloroquine were prescribed to one pregnant woman with systemic lupus erythematosus.
All patients received iron, folic acid, and calcium during the second trimester. All pregnant women also received two doses of tetanus toxoid vaccination. About 30 (6.7%) patients received antimicrobials; the most commonly used antimicrobials were cephalosporins (4%) and nitrofurantoin (2.7%). Paracetamol was prescribed to 21 (4.7%) pregnant women and NSAIDs were prescribed to 7 (1.6%) pregnant women. One of the most common drugs prescribed during the second trimester was thyroxine in 34 (7.9%) patients. Other drugs prescribed during the second trimester were ranitidine (2.4%), pantoprazole (1.4%), nifedipine (1.4%), and cough syrup containing chlorpheniramine (1.1%).
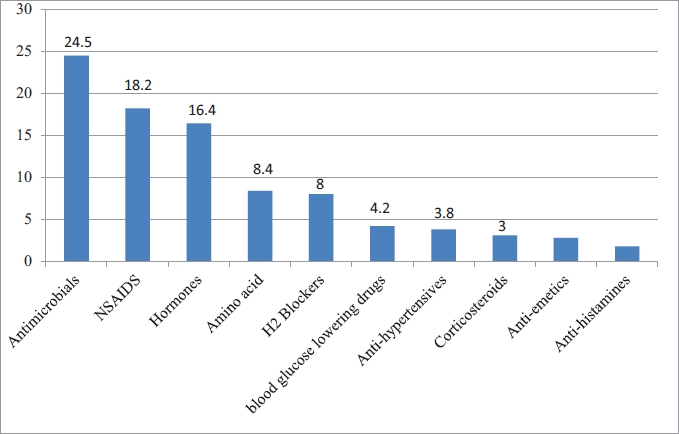
During the third trimester, all pregnant women continued to receive iron, folic acid, and calcium supplements. Other commonly prescribed drugs were antimicrobials (7.3%) consisting of antibiotics like cephalosporins (2.7%) and anti-fungal like clotrimazole (4.5%). About 42 (9.5%) pregnant women received thyroxine for hypothyroidism, 11 (2.4%) and 5 (1%) received ranitidine and pantoprazole, respectively, 9 (2%) received betamethasone, 8 (1.8%) received ondansetron, 40 (9%) received paracetamol, and 8 (1.6%) received NSAIDs. The most common antihypertensive medication used during third trimester was labetalol in 1% of the pregnant women. For gestational diabetes, insulin was prescribed for 1.4% of the pregnant women. Some of the other drugs prescribed during the third trimester were L-Arginine (5.4%), Calamine lotion (0.2%) and SLE drugs like prednisolone (0.2%), azathioprine (0.2%), and hydroxychloroquine (0.2%). The most prevalent drugs for disease conditions prescribed across all three trimesters are presented in Figure 2.
Determinants of Drug Prescription Patterns During Antenatal Care
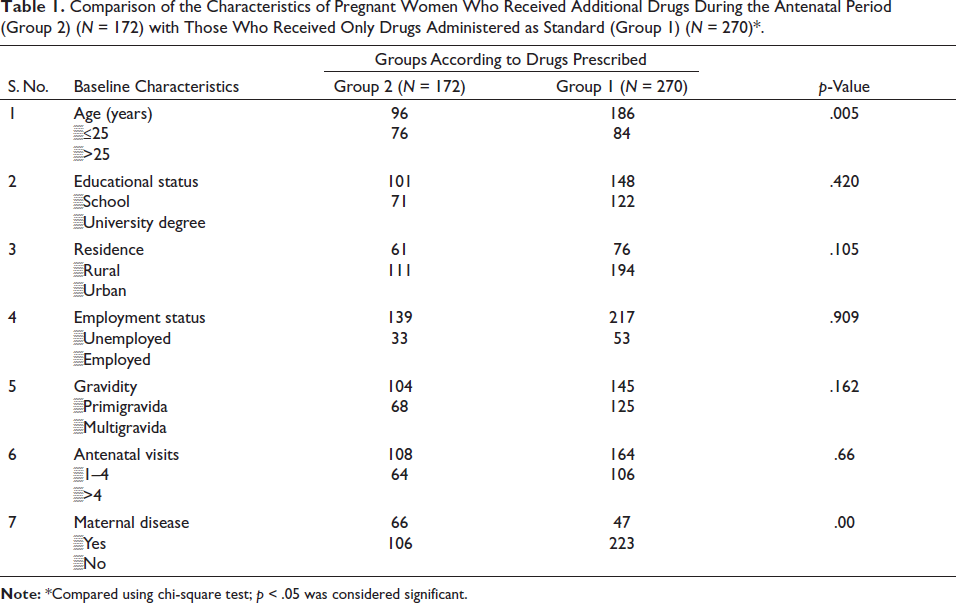
The results of the chi-square tests demonstrated that being over 25 years of age (p = .005) and the presence of a disease condition (p < .001) were the significant factors associated with drug prescription in pregnancy, as presented in Table 1.
Comparison of the Characteristics of Pregnant Women Who Received Additional Drugs During the Antenatal Period (Group 2) (N = 172) with Those Who Received Only Drugs Administered as Standard (Group 1) (N = 270)*.
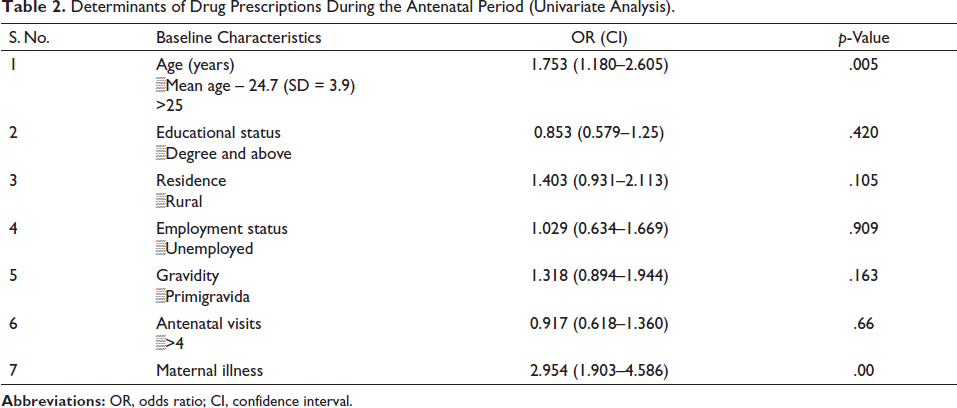
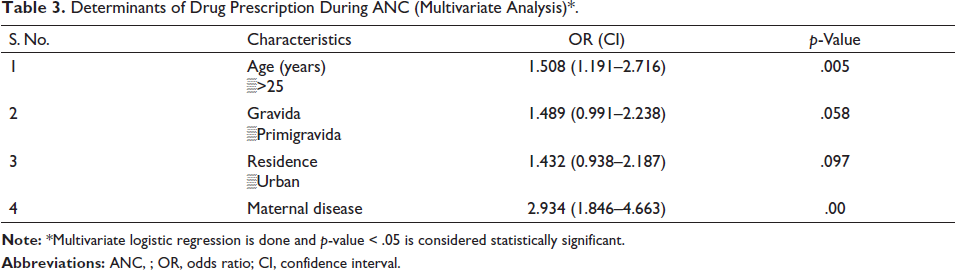
To determine the predictors affecting drug prescription, we performed a univariate regression followed by a multivariate logistic regression. A significant association was found between maternal age over 25 years [OR (CI) 1.508 (1.191–2.716) (p = .005)] and the presence of a maternal disease condition [OR (CI) 2.934 (1.846–4.663) (p = .00)] with the of prescription of drugs during an antenatal period as presented in Tables 2 and 3.
Determinants of Drug Prescriptions During the Antenatal Period (Univariate Analysis).
Determinants of Drug Prescription During ANC (Multivariate Analysis)*.
Labor and Postpartum Outcomes
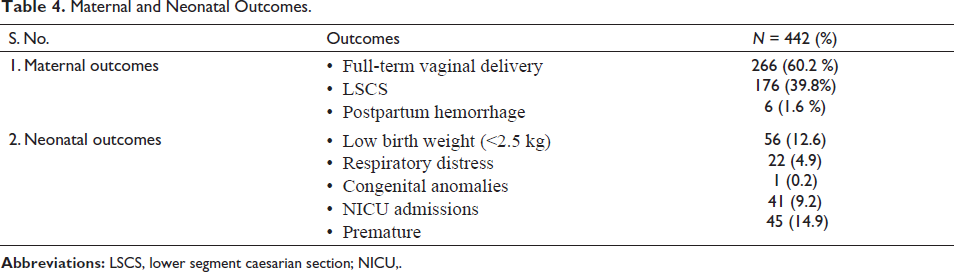
Out of 442 deliveries, 266 (60.2%) were normal vaginal delivery and 176 (39.8%) were cesarean sections. Overall, maternal and neonatal outcomes are presented in Table 4. No difference in outcomes were observed for the two groups identified.
Maternal and Neonatal Outcomes.
Drug Prescription Patterns During Labor
Prostaglandin was used by 51% of pregnant women to induce labor. Oxytocin was used by 82% of pregnant women. The most commonly prescribed non-routine drug were antibacterial agents, primarily the cephalosporins cefazolin (40%) and cefotaxime (22%).
Drug Prescription Patterns During Postpartum Period
The most commonly prescribed drug class was antibiotics, namely cephalexin (48%) and cefazolin (31%). Opioid analgesics (pethidine and tramadol) were prescribed for 47% of patients. Other drugs prescribed postpartum included methergine for 24 patients (5 %) and oxytocin for 107 patients (24%).
Discussion
This study was conducted as a prospective cross-sectional study of 442 pregnant women. Demographic characteristics, drug prescription patterns and factors affecting drug prescription patterns were analyzed.
The mean age among members of the study was 24.7 (SD = 3.9) years. This was comparable to the mean age of the urban antenatal population observed in a study conducted in Mumbai. 11 This is higher than the national average age of pregnant women, 21. 12 In this study, approximately 44% of participants were college graduates and 19% were employed. This was higher than the number of graduates and employed women in the previous study. In this study, approximately 56% of the pregnant women were primigravida, similar to trends from other developing countries. 13
Notably, approximately 60% in both Group 1 and Group 2 had three to four antenatal visits. In previous similar studies, approximately 21% of pregnant women had three to four antenatal visits. 11 This could be attributed to the high urban population in this study (69%). In this study, 143 participants (32%) had at least one disease condition during pregnancy. The most predominant was hypothyroidism (9.7%) followed by anemia (9%). This coincides with previous studies from India, where the prevalence of hypothyroidism ranges from 4.8% to 11%.14–17 The high prevalence of hypothyroidism in the Indian population has previously been attributed to the presence of goitrogens in the Indian diet.18, 19 Gestational diabetes mellitus was present in 1.3% of participants and hypertension in 1.8%, which was similar to a previous study from Telangana, India. 20
The average number of drugs prescribed for each pregnant woman during antenatal care was 2.68, similar to previous literature. 11 One hundred seventy-two (38.9%) pregnant women received additional drugs during antenatal care; the most commonly prescribed drug classes included antimicrobials (24.5%) and NSAIDs (18.2%). Out of the 285 drugs prescribed, excluding standard medications, the majority of the drugs belonged to FDA drug class B (66.6%) followed by FDA class A (16.8%), which was similar to the trend observed in previous literature. 11
Antibiotics were the most common drug class prescribed, primarily cephalosporins like cefazolin (40%) and cefotaxime (22%). This could be possibly due to cephalosporins being considered safe to use during breastfeeding. 21 Prostaglandin was used in 51% of participants and oxytocin in 82%. Opioid analgesics such as pethidine and tramadol were prescribed for 33% and 14% of patients, respectively.
The study population was divided into two groups, as previously mentioned, to analyze prescription patterns. Older maternal age (>25 years) and the presence of maternal disease conditions were significantly associated with the prescription of additional drugs to those administered as standard during and after pregnancy and childbirth. This coincides with the findings of a previous study by Molla et al. 22
To identify the predictors affecting drug prescriptions, a univariate analysis followed by a multivariate analysis was conducted. Maternal age over 25 years and the presence of a maternal illness were factors affecting drug prescription during antenatal care. Thus, the findings of this study indicate that pregnant women over 25 are 1.5 times more likely to be prescribed additional drugs compared to women under 25. The presence of a maternal illness during pregnancy increases this likelihood by 2.9 times.
When neonatal and maternal outcomes were studied, 266 (60.2%) deliveries were normal vaginal deliveries and 176 (39.8%) were cesarean sections. This is similar to the national statistics in India (National Family Health Survey 5, 2018–2019). 23 Low birth weight was seen in 12.6% of newborns, which was lower than reported in the National Family Health Survey. 23 Of the newborns in this study, 9.2% were admitted to NICU, and 14.9 % were premature.
In conclusion, most patients were primigravida and under 25 years. Antimicrobials were the most prescribed drug class. Maternal age over 25 years and maternal illness were identified as the factors affecting medication use. When maternal outcomes were studied, the prevalence of cesareans and prematurity were similar to previous studies. To the best of our knowledge, this is the first comprehensive, prospective study analyzing the predictors of antenatal drug prescription in India. Identification of co-existent medical conditions and maternal age over 25 as factors affecting drug prescription paves the way for future research into this demographic so that appropriate precautions and care can be taken while prescribing medications for this group of patients to avoid teratogenic effects and adverse pharmacodynamic effects while at the same time ensuring optimal control of long-standing and fairly common medical conditions. For this reason, the findings of this study can support better patient management and contribute to further cohort and multicentric research of a critical demographic.
This study had some limitations. Only booked cases were recruited, and over-the-counter drugs or ayurvedic medicines could not be included for logistical reasons such as inconsistent naming of drugs in different states, language variations, and incomplete disclosure by patients, to name a few.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical statement
Ethics approval obtained from Institutional Ethics Committee.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
All data relevant to the study has been submitted.
Informed consent
Informed consent obtained prior to collection of data.