
Abstract
Objective:
To compare the effects of dexamethasone and fentanyl when added to a mixture of bupivacaine and lignocaine in supraclavicular blocks in patients undergoing forearm surgeries.
Methods:
Sixty-six patients aged between 20 to 60 years old belonging to ASA one or two were recruited prospectively, double-blinded, and randomized way. Supraclavicular block under sonographic guidance was performed in the three groups by using injection bupivacaine (0.5%) 20 cc + injection lignocaine (2%) 10 cc + injection 0.9% normal saline; 2ml (Group S), injection bupivacaine (0.5%) 20 cc + injection lignocaine (2%) 10 cc + injection dexamethasone 8 mg (Group D), and injection bupivacaine (0.5%) 20 cc + injection lignocaine (2%) 10 cc + injection fentanyl 50 µgm (Group F). The onset time of sensory and motor block, duration of sensory and motor block, and hemodynamic variables were recorded.
Results:
Group D showed a significantly greater sensory and motor block duration than other groups (P = 0.001). Comparison of hemodynamic variables failed to reveal any statistically significant differences between all the groups.
Conclusion:
Both dexamethasone and fentanyl are good adjuvants in the supraclavicular block, but dexamethasone is better, given faster onset and duration of analgesia.
Introduction
Regional anesthesia is the preferred choice of anesthesia for forearm surgeries. 1 Brachial plexus block is a popular and widely employed regional nerve block technique for perioperative anesthesia and analgesia. The supraclavicular approach to the brachial plexus results in faster onset and complete block, as it can be given at distal trunks where it is most compact throughout the plexus.2, 3 Introduction of ultrasound guidance (USG) has led to enhanced visualization of brachial plexus anatomy, needle placement, and perineural dispersion of local anesthetic, lessening the requirement of local anesthetic and thus decreasing the risk of complications associated with local anesthetic systemic toxicity. 4
Lignocaine has a quick onset of action but only up to 1 h to 1.5 h. The onset of action of bupivacaine is slow, but its action lasts longer. Combining both the drugs, i.e., lignocaine with bupivacaine, is better than individual drugs alone as the mixture provides prolonged action of bupivacaine and rapid onset of lignocaine. Observation from previous studies reveals safety and no increased toxicity with mixtures of bupivacaine and lignocaine. 5
An additive to bupivacaine is aimed for the quick onset and prolonged duration of blockade. 6 Various adjuvants, including fentanyl, midazolam, magnesium sulfate, dexamethasone, and neostigmine, have been added to local anesthetics to prolong the block duration and postoperative analgesia. 7
Fentanyl, a mu receptor agonist which mainly acts by interacting with mu opioid receptor can also activate other receptors like delta and kappa inducing analgesia. The chemical formula is C22H28N2O. The targets of fentanyl molecules are a subclass of the opioid receptor system within the body, mainly localized in the brain within specialized neuroanatomical structures.
Dexamethasone sodium phosphate, a synthetic adrenocortical steroid, is a white or yellow crystalline powder that is exceedingly hygroscopic and freely soluble in water. Its molecular weight is 516.41 and the chemical formula is C22H29FO5. Dexamethasone, a potent glucocorticoid, has anti-inflammatory as well as analgesic properties. When used as an adjuvant with local anaesthetics, it influences the duration of sensory and motor block and the duration of analgesia. The probable reason how corticosteroids produce analgesia may be their anti-inflammatory effect. Specifically, it inhibits ectopic neuronal discharge by blocking nociceptive C-fibers. 8 Dexamethasone as an adjuvant to local anesthetic has been studied in previous investigations. However, there are only a few studies in which the analgesic effect of fentanyl is compared to dexamethasone. Hence, the present study aimed to compare the efficacy of dexamethasone and fentanyl as additives to bupivacaine and lignocaine in the supraclavicular block with the duration of postoperative analgesia as a primary objective and the onset of sensory and motor blockade, duration of sensory, and motor blockade as a secondary objective.
Materials and Methods
Following the approval of the Ethical Committee, this randomized, prospective, double-blinded, single hospital study was conducted under the Department of Anaesthesia, Dr D.Y. Patil Medical College and Research Centre, from July 2021 to November 2021. This study has been registered in the National Clinical Trial Registry of India (
The following inclusion criteria were considered: (a) ASA Grade I or II of either sex, (b) ages between 18 and 60 years of either sex, (c) patients undergoing elective forearm surgeries, (d) hemodynamically stable patients with all routine investigation within normal limits, and (e) availability of informed consent. Also, the exclusion criteria employed were (a) patient refusal, (b) patients with ASA physical status III or more, (c) noncooperative patient, (d) patients with nerve injury, (e) patients who have known allergies to any of the test drugs, (f) patients with coagulation disorders or on anticoagulant drugs, (g) patients with cardiac disease, and (h) patients with respiratory diseases.
Statistical Analysis
The sample size was calculated using WinPEPI® software (WinPEPI software, Brixton Health, London, United Kingdom) concerning an article by Mohsen Sayed, with the level of significance at 5%, power at 90%, and an allocation ratio of 1:1. The minimum sample size was 44, i.e., 22 in each group. As the third group was the control group, we used the same sample size in that group as well (the total sample size was 66, i.e., 22 in each group). 9 The data were entered in MS Excel 2016, and the statistical software IBM SPSS statistics for windows version 16 (IBM Corp; Armonk; NY; USA) had been used for the analysis. An alpha level of 5% had been taken, i.e., if any P-value was less than 0.05, it was considered significant.
Adjuvant added along with local anesthetics determined the group of study. Three equal groups of 22 patients were randomized as per the computer-generated random numbers as follows:
Group D: Injection bupivacaine (0.5%) 20 cc + injection lignocaine (2%) 10 cc + injection dexamethasone 8 mg Group F: Injection bupivacaine (0.5%) 20 cc + injection lignocaine (2%) 10 cc + injection fentanyl 50 µgm Group S: Injection bupivacaine (0.5%) 20 cc + injection lignocaine (2%) 10 cc + injection 0.9% normal saline (NS; 2 mL)
An anesthesiologist who was not involved in drug administration, patient care, or data collection prepared the drug. Nil by mouth (NBM) status and consent were checked in the preoperative room. Basic monitoring equipment (pulse oximeter, non invasive blood pressure (NIBP), and electrocardiogram (ECG) monitor) was connected inside the operating room. Baseline vital parameters were recorded. An intravenous line was secured using a 20G intravenous (IV) cannula in the non operating arm. The supraclavicular block was performed by USG technique using Hitachi Arietta S70—portable USG machine with linear probe attachment 6 MHz to 12 MHz. The patient was supine with his/her head turned 45 degrees to the opposite side, and the probe was placed in a supraclavicular fossa in the coronal plane to inspect the first rib and subclavian artery visually. The brachial plexus and its surrounding structures were viewed. A 50 mm insulated needle with a diameter of 20 gauge was introduced lateral to the probe and parallel to its long axis after the skin was sterilized and local anesthetic administered. By in-plane technique, once the needle pierced the brachial plexus cluster, the anesthetic mixture was administered, i.e., injection bupivacaine (0.5%) 20 cc along with injection lignocaine (2%) 10 cc with the adjuvants was added according to the randomization, i.e., injection dexamethasone 8mg or injection fentanyl 50 µgm or 0.9% NS 2 mL. The drug was injected incrementally after verifying that no air or blood was aspirated just next to artery. The needle was then repositioned to inject near the upper pole of the artery. Local anesthetic dispersion while injecting was confirmed by USG.
Complete sensory and motor blockade in all radial, median, and ulnar regions indicates a successful block. Sensory and motor blockade evaluations were done every 2 min until complete sensory or motor block, or till 30 min whichever was earlier. We measured the duration of sensory and motor block by the time it took for pain sensation to disappear at the arm to reappear paresthesia or complete motor function recovery. Heart rate, blood pressure, SpO2, respiratory rate, and ECG were monitored throughout the intraoperative and immediate postoperative period. Also, notable side effects were looked for and intraoperative sedation was provided whenever needed.
The onset of sensory block was evaluated by pinprick sensation. Dull sensation on pin Prick, which was compared with the other arm, was taken as the time of onset of sensory blockade.
Duration of Sensory Block
Evaluated as the period between the sensory blockade and reappearance of the pinprick response.
Assessment of Motor Block
Assessed with the help of modified Bromage scale.
The Onset of Motor Block
Considered from the injection of the drug up to the time of complete paralysis.
Duration of Motor Block
Interval between the successful block completion and the full recovery of motor function in the upper limb.
Duration of First Rescue Analgesia
Time taken from the drug administration to giving first rescue analgesia. Injection diclofenac 75 mg IM was given when the patient complained of the visual analogue score (VAS) >4.
Depiction of VAS was explained to patients preoperatively. The patient ranked the degree of pain on return of sensations by marking the linear scale. The score was measured by taking the distance from 0.
In order to display analytically, the following statistical methods were adopted: Continuous variables like age, weight is expressed as mean ± standard deviation and compared across the three groups using analysis of variance test. Categorical variables are defined in numbers, proportions, and percentages, and reached across the three groups using Pearson's chi-square test for independence of attributes. The data was entered in MS Excel 2016, and the statistical software IBM SPSS statistics for windows version 16 (IBM Corp; Armonk; NY; USA) has been used for the analysis. An alpha level of 5% has been taken, i.e., A P-value less than 0.05 was considered significant.
Results
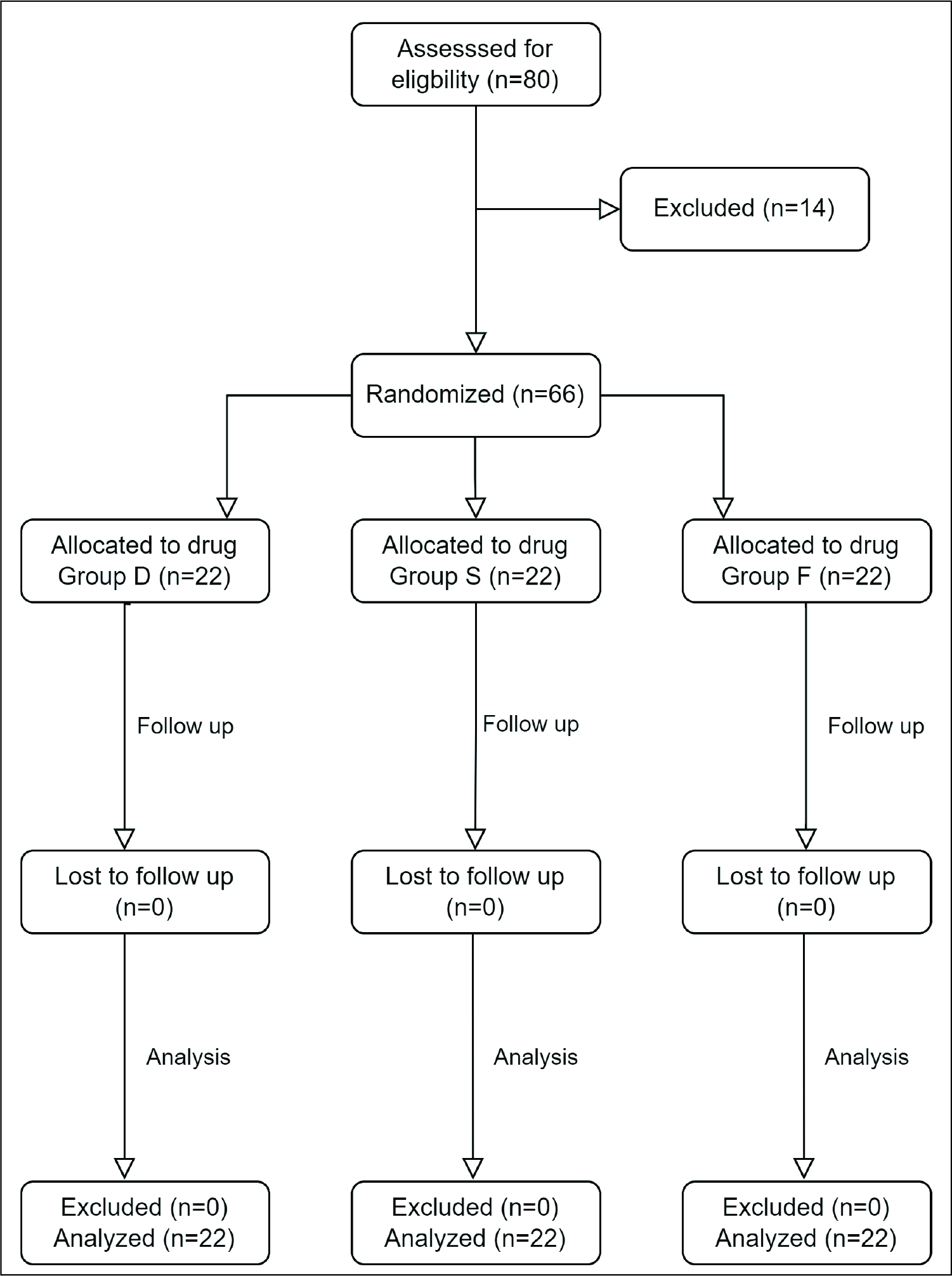
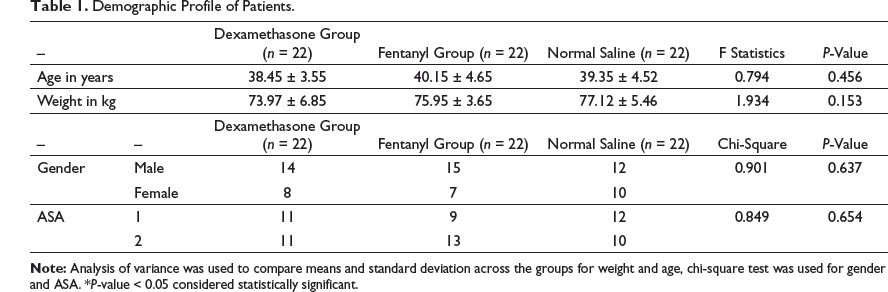
This study was done at Dr D.Y. Patil Medical College and Research Centre, Pimpri. Among 80 patients initially enrolled in the study, 14 patients had to be excluded because of the applied stringent exclusion criteria (Figure 1), sixty-six patients were divided equally into three groups receiving dexamethasone, fentanyl, and normal saline, respectively, to a mixture of bupivacaine and lignocaine in the supraclavicular block as per randomization. Regarding demographic data and ASA classification, there was no statistically significant difference between the groups (Table 1).
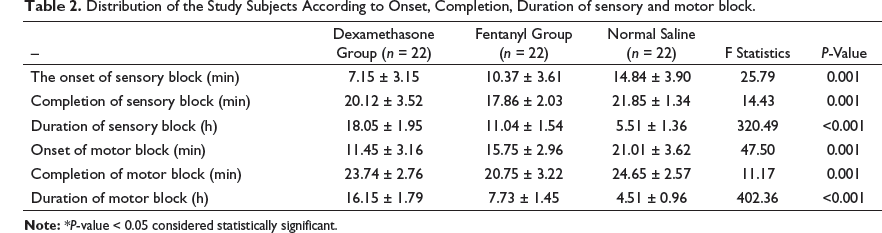
Table 2 shows the mean onset of sensory blockade. In Group S, it was 14.84±3.90 min, in Group F, it was 10.37 ± 3.61 min, and whereas in Group D, it was 7.15 ± 3.15 min. Using Pearson's chi-square test for analysis it was observed that these results were significant (P-value = 0.001). The mean onset of the motor blockade in Group S was 21.01 ± 3.62 min, Group F was 15.75 ± 2.96 min, and Group D 11.45 ± 3.16 min. As per Pearson's chi-square test for analysis, it was found that these results were significant (P-value = 0.001). The mean duration of sensory blockade in Group S was 5.51 ± 1.36 h, in Group F 11.04 ± 1.54 h, whereas in Group D, it was 18.05 ± 1.95 h. Using Pearson's chi-square test for analysis, it was found that these results were significant (P-value <0.001). The mean duration of the motor blockade in Group S was 4.51 ± 0.96 h, Group F was 7.73 ± 1.45 h, and Group D was 16.15 ± 1.79 h. As per Pearson’s chi-square test for analysis, it was found that these results were significant (P-value < 0.001).
CONSORT diagram showing enrolment, allocation, and analysis at every stage of randomized control trial. n = number of patients
Demographic Profile of Patients.
Distribution of the Study Subjects According to Onset, Completion, Duration of sensory and motor block.
Distribution of the Study Subjects According to use of First Analgesia Rescue, Postoperative Pain.

Discussion
In forearm surgeries, the supraclavicular block is preferably used compared to general anesthesia to avoid unwanted effects like hypertension, arrhythmias, tachycardia, and increased intraocular and intracranial pressure.10, 11 USG provides an effective reliable block that has increased safety because of better visualization of anatomy and needle placement. The regional technique is better for associated conditions like uncontrolled diabetes, hypertension, cardiovascular, or respiratory diseases. The cost-benefit is also more with a regional block. It is useful in early ambulation of the patient and day care surgeries. Many adjuvants such as adrenaline, clonidine, steroids, neostigmine, midazolam, magnesium sulphate, dexmedetomidine, and opioids like tramadol, fentanyl, and morphine have been tried in peripheral nerve blocks to improve the quality, duration, and avoid using toxic doses of local anesthetics.
The mean onset of sensory block was rapid in Group D (7.15 ± 3.15 min) as compared to the Group F (10.37 ± 3.61 min) compared to Group S (14.84 ± 3.90 min). The onset time of motor block was also rapid in Group D (11.45 ± 3.16 min) than in Group F (15.75 ± 2.96 min) compared to Group S (21.01 ± 3.62 min) which was clinically and statistically significant (P < 0.005).
Nagabhushanam et al. in their study found that the addition of dexamethasone to the mixture of local anaesthetics produced rapid onset of sensory (8.43 ± 1.89 min) and motor block (12.93 ± 1.48 min) compared to fentanyl (sensory being 10.1 ± 1.3 min, motor being 14.4 ± 1.73 min) added as an additive supraclavicular block. 12 Biradar et al., El-Baradey et al., Vieira et al., and Shrestha et al. stated that in ultrasound-guided supraclavicular brachial plexus block, when dexamethasone is used as an additive to local anesthetics, produced a relatively rapid onset of motor and sensory block.13–16 The results of these studies are in concurrence with our study.
Sayed et al. found that onset of sensory and motor block was shorter in the fentanyl group than dexamethasone group. This result met with with Choi et al. but not similar to our present study.9, 17
Chavan et al. observed that the addition of fentanyl 50 µg into local anesthetic solution supraclavicular block prolongs the duration of analgesia but delays the onset time of sensory blockade, similar to our study. Chavan et al. postulated that the changes in the pH of anesthetic solution could be responsible for the possible mechanism of delaying the onset of sensory and motor blockade by fentanyl. 18
The mean duration of sensory block in our study was prolonged in Group D (18.05 ± 1.95 h) as compared to Group F (11.04 ± 1.54 h) and Group S (5.51 ± 1.36 h). The duration of motor block in the present study was also found to be prolonged in Group D (16.15 ± 1.79 h) than Group F (7.73 ± 1.45), and the variation between the two groups was found to be statistically and clinically significant (P < 0.005).
A study by Sharma et al., which is similar to our present study, observed that Group D showed prolonged duration of sensory block (17.192 ± 2.897 h) and motor block (15.582 ± 2.815 h) compared with Group F where the duration of sensory block was (6.772 ± 0.335 h) and duration of motor block was (5.654 ±0.437 h). 19
Nagabhushanam et al. and Sayed et al. observed that the sensory blockade lasted longer than motor block, similar to our study.12, 9 Small fibers need less concentration of local anesthetic than large fibers. Large motor fibers require a greater concentration of minimal effective local anesthetic than the small ones (sensory fibers). This is a possible mechanism for prolonged sensory blockade than the motor block. 20
The mean duration of analgesia was prolonged in Group D (19.37 ± 1.88 h) compared to Group F (8.78 ± 1.57 h) and Group S (6.65 ± 1.77 h), which was statistically highly significant. The study done by Sayed et al., which is similar to our study, showed that the duration of analgesia was longer in Group D (19.37 ± 1.92 h) than Group F (12.67 ± 1.67 h). 9
Dexamethasone is a very potent and highly selective and long-acting glucocorticoid. Three mechanisms may explain the action of dexamethasone in peripheral nerve blocks. One, the absorption of local anesthetics is reduced as steroids produce vasoconstriction.21–23 The second mechanism potentiates potassium channels’ inhibitory activity on sensory pain nerves. The third one, because of anti-inflammatory action and inhibition of nociceptive C-fibers. 23
Swaminathan et al. observed that dexamethasone is advantageous for the longer duration of analgesia with all local anesthetics. 24
Peripheral action of fentanyl for analgesia was hypothesized by Nishikawa et al. mainly by three mechanisms. 25 Firstly, fentanyl acts directly on the peripheral nervous system, and opioid binding sites are found on the primary afferent tissues (dorsal roots).10, 26 Fentanyl acts on the dorsal horn because of the presence of bidirectional axonal transport of opioid-binding protein. 27 This accounts for the analgesic action of fentanyl. Secondly, fentanyl may diffuse from the brachial plexus sheath to the subarachnoid and epidural spaces, which then binds with the opioid receptors in the dorsal horn. Thirdly, the local anesthetic action of fentanyl is potentiated by analgesia mediated by an opioid receptor that leads to fentanyl uptake to the systemic circulation.
Rajkhowa et al. mentioned in their study that ropivacaine and fentanyl are believed to prolong sensory and motor blockade. It is probable that opioids bind to opioid-binding sites on the dorsal nerve roots and diffuse into surrounding tissues and the epidural and subarachnoid spaces. Additionally, the central opioid receptors may also be involved after systemic absorption of fentanyl. 28
The novelty of our study established is that dexamethasone is superior to fentanyl in terms of faster onset of sensory and motor blockade, prolonging the duration of the block, quality, and postoperative analgesia. These results are analogous to the study done by Sharma et al. and Yaghoobi et al.19, 23
None of the patients had variations in heart rate, blood pressure, and respiratory rate following the administration of dexamethasone and fentanyl along with local anesthetics. Nagabhushanam et al. found no statistically significant difference in hemodynamic profile between dexamethasone and fentanyl as an additive to local anesthetic, 11 similar to that of our study.
Conclusion
Both dexamethasone 8 mg and fentanyl 50 µg are suitable analgesic adjuvants with local anesthetics. They can be safely used with a stable hemodynamic profile to prolong the duration of analgesia in the supraclavicular block. In supraclavicular block, the duration and postoperative analgesia were superior when dexamethasone was used as an additive to local anesthetics, compared to fentanyl and normal saline.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.