
Abstract
Objectives:
To shed some light on the understudied complication of chronic prolonged exposure to antipsychotics (AP) in children with consideration to with autism spectrum disorder (ASD).
Methods:
We electronically searched PubMed, Google Scholar, clinical trial.gov, and Medline Database of clinical studies up to June 2021. We used the following keywords: “bone mineral density, osteoporosis, osteopenia, bone loss, bone changes” AND “antipsychotics, SGAs, atypical antipsychotics” AND “pediatric, adolescent, young, youth, children.” We used [Mesh] Term for “antipsychotics agent” and “bone mineral density” and “autism spectrum disorder” and “child.” We retrieved relevant observational studies, reviews, case series, and randomized clinical trials.
Results:
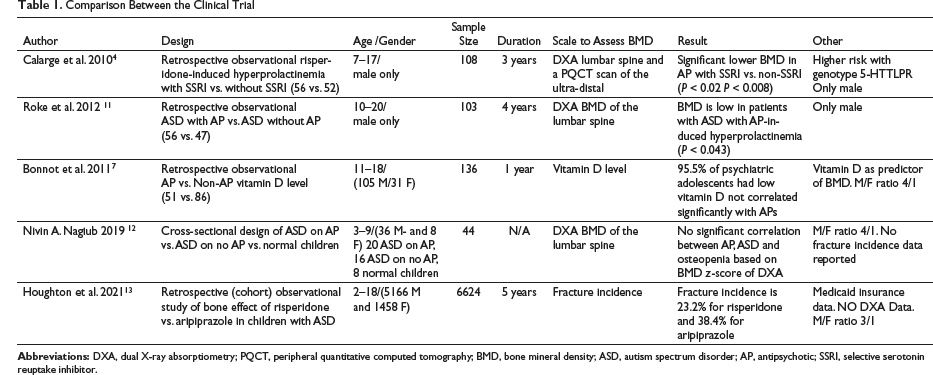
Yvette Roke et al., in 2012, reported in a retrospective observational study that lumbar spine bone mineral density (BMD) and the biochemical bone marker were lower in the AP-treated boy with hyperprolactinemia in comparison to the non-AP-treated group, while a retrospective observational study of institutional adolescents with a psychiatric condition, carried out by Bonnot et al. in 2011, found significant vitamin D deficiency in psychiatric inpatient adolescents that is unrelated to the specific APs. Third, Calarge et al. in a 2010 retrospective observational study have reported a significant reduction in BMD in adolescents with risperidone-induced hyperprolactinemia and selective serotonin reuptake inhibitor (SSRI) compared to another group with risperidone-induced hyperprolactinemia without SSRI. On the other hand, Nivin A. Nagiub et al. (2019) in the cross-sectional study found no correlation between BMD and AP use in children with ASD. Houghton et al., in 2021, found a high fracture prevalence of 38% with aripiprazole compared to risperidone in children with ASD.
Conclusion:
Clinicians should be aware of the potential negative effects of APs on BMD, considerably in children with ASD that has additional risk factors for osteoporosis and bone disease. A provider needs to utilize more sensitive screening and diagnostic tools; the pediatric physician should evaluate other risk factors to prevent early osteopenia and bone fracture in children with ASD who are on chronic psychotropic medication, before adjusting to the AP medication.
Introduction
Up to 20% of children and adolescents have been diagnosed with a mental condition, 1 and there is an increasing trend of prescribed Food and Drug Administration (FDA)-approved (based on safety and efficacy of FDA approved clinical trial) and off-label second-generation antipsychotics (APs) among children and adolescent. 1 Furthermore, a two- to fivefold increase in the prescription of APs in children younger than six years has been recorded recently, despite the limited information on their long-term effects on early child development. 1 As well as, up to 80% of younger children are on multiple psychotropic medications at the same time. 1 The increasing use of atypical APs to treat pediatric psychiatric conditions has led to concerns over the long-term safety of these medications. While most of the attention was focused on cardio-metabolic side effects of these drugs, many clinical studies show evidence that APs can also negatively impact bone metabolism in long term. 2 Especially when these medications were started in the childhood period, when maximum bone growth happens, these lead to subsequent later life bone diseases such as osteoporosis with high comorbidity and mortality. 2 This risk is augmented when the AP is commonly coprescribed with other psychotropics such as psychostimulants and selective serotonin reuptake inhibitors (SSRIs), which have also been associated with detrimental metabolic bone changes. 2 Alongside, peak bone growth achieved early in life will determine later bone mineral density (BMD).1, 2 Eighty-five percent of critical bone growth happens before the age of 18; a loss of 5% to 10% of the peak BMD can significantly increase the chance of fractures. 2 Pubertal bone growth and bone mineralization are two different independent processes that are disproportionally related, where normally the mineralization lags behind bone growth by about eight months. 3 However, this process is disturbed by endocrine disorders such as hyperprolactinemia which is induced by APs. 3 Patients with schizophrenia have a 54% increased risk of mortality after a major fracture than the control group. 4 A recent meta-analysis on decreased BMD in schizophrenia patients revealed that the overall pooled prevalence of osteoporosis (standard deviations 2.5 times below the healthy population T-score) was 13.2% and that of osteopenia (BMD value more than 1 SD but less than 2.5 SD) was 40.0%. 4 APs can negatively affect the bone in multiple ways, such as by blocking dopamine-2 receptors and subsequent hyperprolactinemia with potential hypogonadotropic hypogonadism with significant detrimental effects on bone growth. 2 Conversely, hyperprolactinemia has a direct negative effect on bone growth, through prolactin receptors on the osteoblast, regardless of the gonadotrophic hormonal level. 2 In addition, the possibility that high prolactin can lower calcium absorption and activate parathyroid hormone-related peptides adds another burden on bone growth. 2 Switching the APs to aripiprazole has been associated with a drop in the prolactin level with the reduction in serum bone-specific alkaline phosphates (a biomarker of bone formation) and urinary N-telopeptide cross-links (NTx) which are bone resorption marker. 5 Another route APs might delay the bone metabolism is through modulating several serotoninergic and adrenergic receptors on the osteoblast and osteoclast cellular level regulation. 2 Finally, it is possible that APs impair bone metabolism by either directly or indirectly decreasing the muscular activities, which is the major promoting factor of the bone modeling and remodeling activity. 2 Adolescents with severe chronic mental health conditions are at higher risk of low vitamin D levels, because of poor diet, limited physical activities, low sun exposure, and high substances comorbidity, and this increases their bone metabolism vulnerability and exaggerates the detrimental effects of APs on the bone mineralization.6, 7 One observational study in schizophrenia points out the correlation of accelerated bone resorption in schizophrenia adult patients on chronic APs to the metabolic changes, where they found elevated serum osteocalcin and β-Cross Laps levels that positively correlated with high insulin, low estradiol level, which might point out to a possible abnormality in glucose and lipid metabolism, and insulin resistance. 7
Children and adolescents with autism spectrum disorder (ASD) may carry a higher risk for skeletal changes for several reasons than other children. They may be chronically on high-dose AP medications, such as risperidone, that negatively interfere with bone metabolism. 8 Besides, they often have sensory oversensitivities and aversion to diet items restricting their intake of nutritious foods, or they may be on restrictive diets regime (e.g., gluten-free casein-free diets) because of perceived therapeutic benefits, likewise, they are isolated with limited cognitive, expressive language skills, social, and/or communication abilities. 8 And limited engagement in physical activity puts them at an extra higher risk of poor BMD. 8 One of the meta-analysis reports that median prevalence of AP use in ASD children and adolescent is about 17%, with risperidone being the most commonly prescribed AP (55%), followed by aripiprazole (35%), and up to 22% are on poly-pharmacological psychotropic combination.8, 9, 10 Although hyperprolactinemia is more frequently seen with first-generation APs, this review will be focused mainly on the second (atypical)-generation APs because they are prescribed and utilized more frequently in clinical practice. There is a narrow perception of the long-term bone effect of APs in children and this review might shed some light on this camouflaged complication of APs.
Methods
We (WA, AM) independently electronically searched PubMed, Google Scholar, clinical trial.gov, and Medline database of clinical studies up to June 2021. We used the following keywords: “bone mineral density, osteoporosis, osteopenia, bone loss, bone changes” AND “antipsychotics, SGAs, atypical antipsychotics” AND “pediatric, adolescent, young, youth, children.” We also searched for studies of individual AP medication by name. We used [Mesh] Term for “antipsychotics agent” and “bone mineral density” and “autism spectrum disorder” and “child.” We retrieved relevant observational studies, reviews, case series, and randomized clinical trials. We excluded animal studies, case reports, non-peer-reviewed publications or publication written in a language other than English.
Results
Calarge et al., in 2010, have reported a significant reduction in BMD in adolescents with risperidone-induced hyperprolactinemia with SSRI compared to another group with risperidone-induced hyperprolactinemia without SSRI. 4 In a three year long retrospective and cross sectional observational study of 108 boys (mean age = 11.7 years) aged 7 to 17 years, were enrolled with DSM-IV clinical diagnoses, that are on risperidone with hyperprolactinemia and the correlation with BMD, 50% of the patient had significant hyperprolactinemia. 4 Of these, 52% (n = 56) had been taking an SSRI for a median duration of 2.8 years, while 48% had no SSRI exposure. After assessing child development, anthropometric measures, physical activity, calcium and prolactin levels, dual X-ray absorptiometry (DXA) of the lumbar spine, and measuring the volumetric BMD by peripheral quantitative computed tomography (PQCT) scan of the nondominant ultra-distal radius at end of this period, it was observed that there was a significant correlation between serotonin-transporter-linked promoter region (5-HTTLPR) genotype and SSRI treatment effect on total lumbar spine BMD z-score (P < 0.05) in white non-Hispanic children. The BMD at the ultradistal radius was not statistically significant among LS genotype carriers’ children, patients on SSRIs and AP had lower lumbar BMD z-score (P < 0.02) and trabecular BMD at the radius compared to the untreated patients (P < 0.01).2, 4
Roke et al., in 2012, reported lumbar spine BMD and the biochemical bone marker was lower in the AP-treated group with hyperprolactinemia than in the non-AP-treated group. 11 A retrospective observational study (mean duration 52 months) was done on physically healthy 10- to 20-year-old boys with ASD and/or disruptive behavior disorder (DBD) on chronic AP (n = 56) vs non-AP (n = 47) treatment. Prolactin levels, vitamin D, and biochemical bone markers were followed, the lumbar spine and total body BMD were measured by DXA, and volumetric BMD of the lumbar spine was calculated. 11 The study was done in Netherland between 2006 and 2009. Hyperprolactinemia was observed in 49% of the boys treated with an AP during the treatment. The mean volumetric lumbar spine BMD z-score was lower in the AP-treated patients with hyperprolactinemia than in the AP-treated patients without hyperprolactinemia (P = 0.043) and the same pattern were observed with bone marker carboxyterminal cross-linking telopeptide collagen. Low BMD is reported in 7% to 11% of the hyperprolactinemic boys. The mean lumbar spine and total body BMD z-scores and body composition were similar in the boys who were or were not treated with an AP. Biochemical bone parameters were within normal limits. 11
Bonnot et al. reported, in 2011, no significant differences in the vitamin D levels among patients treated with APs and patients who were not treated with AP. 7 A retrospective observational study of 136 adolescents, admitted to the child and adolescent psychiatric university hospital, was done in Paris. Children were observed for 12 months during 2009. Of these, 105 were males and 31 females aged 13.8 years on average. Fifty-one patients were treated with AP. 7 Other psychotropic medications than AP were not included; patients with other causes of vitamin D deficiency were excluded; participants were subdivided according to their illness into three categories: (a) psychotic spectrum disorders, (b) developmental disorder, and (c) other illnesses, including borderline personality disorder, conduct disorder, adaptation disorder, and mood disorder with no psychotic features. After considering age and BMI, univariate analyses compared 25(OH) vitamin D levels in the adolescent inpatient sample within sex, ethnic origin, disease type, and APs (treated vs. untreated). Overall, 25(OH) vitamin D levels were remarkably low (mean±SD, 15.9± 8.4 ng/mL), for both males and females. Moreover, only 6 patients (4.5%) had a vitamin D levels > 30 ng/mL, whereas 97 patients (72.4%) had levels < 20 ng/mL; no significant correlations between sex, age, BMI, and 25(OH) vitamin D levels were found. A significant difference between ethnicity (blacks/North Africans vs. Caucasians) and 25(OH) vitamin D blood levels was seen. After linear regression on a logarithm-transformed dependent variable to normalize residuals, we found no differences between patients treated with APs and patients who were not treated with Aps, and no differences were observed for 25(OH) vitamin D levels between patients taking risperidone and patients taking other APs. Also, no significant correlation was seen between AP treatment duration and 25(OH) vitamin D levels. 7
Nagiub et al., in 2019, found no correlation between the use of AP and BMD in children with ASD. 12 A cross-sectional design study that included 44 children aged 3 to 9 years, divided children into 3 groups: 20 children with ASD on APs vs. 16 with ASD on no medication vs. eight normal children. 12 DXA of the lumbar spine failed to show significant differences in BMD reflected on z-score. 12
Houghton et al. found, in 2021, aripiprazole has a higher fracture prevalence in ASD children compared to risperidone. 13 A retrospective observational study between 2013 and 2018 includes 6624 children, aged 2 to 18 years, with ASD and on AP either risperidone or aripiprazole. 13 Fracture incidence was 23.2% with risperidone compared to 38.4% with aripiprazole. 13
Discussion
This review showed that AP-induced hyperprolactinemia is a significant cause of bone disease in children, and that risk is accentuated with chronicity of the treatment and with SSRI polypharmacy. Adolescents with ASD especially with low vitamin D is considered a high-risk group. Early bone changes were observed in the trabecular bone region. Risperidone is the most commonly used AP that is associated with hyperprolactinemia-induced osteomalacia while, Abilify is most commonly associated with a bone fracture. This review includes five studies addressing the effect of APs on bone metabolism in children with or without ASD. One study showed a significant reduction in BMD in an adolescent group with risperidone-induced hyperprolactinemia with SSRI in comparison to another group with risperidone-induced hyperprolactinemia without SSRI. Those treated with SSRIs and APs had lower lumbar BMD and trabecular BMD z-score at the radius compared to the other group.2, 4 Although the finding was most prominent at the lumbar spine, a similar change was seen in the trabecular bone at the ultra-distal radius bone. 4 While in the other study no significant differences have been recorded in the lumbar spine and total body BMD in children with ASD regardless of APs treatment and it is not considerably distinctive from the general population. 11 But in the same study done by Roke et al., diminished volumetric BMD was recorded in 7% (volumetric lumbar spine BMD) and 11% (areal lumbar spine BMD) of the AP-induced hyperprolactinemic boys. 11 Furthermore, Bonnot and colleagues found 95.5% of inpatient psychiatric children had low vitamin D levels < 30 ng/mL, while 72.4% had a level below 20 ng/mL. The normal reference vitamin D level for good bone health is 30 ng/mL. 7 No significant change in the vitamin D level was observed among AP-treated children compared to the children on no medication. 7 In our review, the cross-sectional design study done by Naguib et al. to study the long term effect of AP on BMD in ASD, no positive correlation between BMD and use of APs in children with ASD compared to APs naïve ASD or normal children have been reported. 12 While Houghton et al. (2021) found that the bone fracture prevalence with risperidone is 40% less than aripiprazole in children with ASD. 13 The incidence was 23.2% for risperidone vs. 38.4% for aripiprazole. 13
The AP has multiple mechanisms of affecting bone metabolism and mineral density. Hyperprolactinemia, that could happen in up to 50% of the pediatric patient on AP, is one of the main causes, regardless of the underlying psychiatric condition.2, 4, 9 Dopamine-blocking properties of AP have direct negative effects on the bone metabolism and indirect negative effect through raising the prolactin level.2, 14 In addition, modulating the serotonergic and adrenergic system by APs plays a role in aggravating bone changes. The effects are observed clearly with the co-administration of SSRI with AP, specifically in genetically vulnerable children who carry the allele 5-HTTLPR variants. 4 5-HTTLPR variants children have a higher risk for reduced BMD.2, 4 Furthermore, co-prescription of SSRI might negatively slow the metabolism of the AP cytochrome system, such as risperidone, through inhibition of cytochrome-P enzyme and subsequent increase in the AP blood level and the risk of hyperprolactinemia.2, 4
Comparison Between the Clinical Trial
A small portion of AP-induced hyperprolactinemia may present with hypogonadism, making the recognition of this condition clinically challenging and hypogonadism is unreliable predictors of underlying bone condition. The study recognized this clinical association in one patient only. 11 AP-induced hyperprolactinemia has obvious negative effects on bone metabolism, seen obviously with first-generation APs. The levels of bone resorption marker, carboxyterminal cross-linking telopeptide of bone collagen (CTX), were significantly low and levels of bone formation marker type 1 amino-terminal propeptide of procollagen (P1NP) tended to be lower in AP-treated boys with hyperprolactinemia than in AP-treated boys without hyperprolactinemia. 11 This reflects the negative metabolic effect of hyperprolactinemia on bone turnover. 11
Fracture prevalence in ASD patients is controversial; two retrospective observational studies that evaluated the prevalence of fracture in ASD patients found this to be lower in ASD patients than non-ASD patients, 12% vs. 25% for the comparison group (observed for 30 years, n = 118 children).9, 11 Fracture prevalence correlates positively with the use of AP in ASD patients as reflected in the study done by Houghton and his colleagues with prevalence reaching 38.4% with aripiprazole. 13 While, the other study evaluates bone cortical thickness in children with ASD (mean age 7 years, n = 75) measured on a hand and wrist compared to the normal group; the boys with ASD had reduced bone cortical thickness.9, 11 Despite low BMD in ASD patients, the fracture prevalence rate is less, but a fracture in psychiatric patients carries high morbidity and mortality. 4 The patients of this study had a normal calcium metabolism and a 20% fracture prevalence rate (21% for the ASD without hyperprolactinemia vs. 19% for the ASD with hyperprolactinemia) which was also considered low compared with the normal population fracture rate of 37%. These findings could be explained based on the fact that the boys with ASD have limited outdoor groups or physical activities, which would prevent them from getting bone fractures. 11 Significant low levels of vitamin D were observed in ASD boys with AP-induced hyperprolactinemia group compared to ASD without AP (34% vs. 18%, respectively). 11 These observations are inconsistent with the finding of Bonnot et al. 7 Low vitamin D could be caused by APs, dietary restriction, limited sun exposure, or predominant nonphysical indoor activities of the children. 11
Assessing BMD in children utilizing plain skeletal radiography which detects BMD when the loss exceeds 40% is too insensitive in clinical practice. 3 Currently available modalities used to assess BMD include metacarpal morphometry, quantitative bone ultrasound, quantitative computed tomography (QCT), dual-energy X-ray absorptiometry (DXA), and magnetic resonance imaging (MRI) bone density. QCT measures the bone volume and thus accurately assess volumetric BMD and can differentiate between cortical and trabecular bone but it has high radiation risk. 3 Peripheral QCT (PQCT) is an alternative technique with less radiation risk and it is more convenient to be used with children. 3 DXA is still the mean tool for assessing bone density., It has low radiation exposure, precise results, and lower cost than QCT, but it does not directly measure true volume or assess volumetric BMD. 3 The decision of starting the children on AP for a psychiatric condition is to maintain their safety, and usually, the children must be taking them for a prolonged period to prevent recurrent of their symptoms. This puts them at higher risk of side effects with long-term sequelae. 2 Bone changes and hyperprolactinemia are some of the commonly unnoticed adverse effects with serious future potential complication. 2 Current practice guidelines do not recommend universal testing for prolactin level or bone assessment during AP treatment. 2 This is understandable as there is no clear correlation between the use of AP, prolactin level concentration, and skeletal complication in children and adolescent psychiatric patients. 2 There is no clear correlation between the patient’s age, duration of treatment, and the patient’s sex with BMD in the psychiatric population in comparison to the general population, which has a negative association between mean age and BMD. 11 Another controversial point that needs further study is whether the changes in BMD are caused by AP or triggered by an underlying psychiatric condition such as schizophrenia.13, 14
Limitation
A few studies address the long-term effect of APs on bone metabolism in children. From the available data from observational studies, it is hard to isolate the potential effect of APs, SSRIs, or other confounders on BMD from that of the underlying psychiatric condition. Many psychiatric conditions might be associated with bone loss as a primary process such as depression or schizophrenia.2, 4 There is inconsistency regarding the tool used to assess the BMD, such as DXA lumbar spine or PQCT ultra-distal bone, and the selected site such as lumbar spine or peripheral bone or nontrabecular bone region; therefore, the result of the review would be complicated by many confounding factors. 12 Another limitation is the analyses were done predominately for males, who were mostly non-Hispanic white patients, which limits the generalization and diversity of the result.2, 3, 4
Conclusion
Clinicians should be aware of the potential negative effects of long-term use of APs on BMD, considerably ASD pediatric patients with additional risk factors for osteopenia and osteoporosis. A provider needs to more frequently utilize a sensitive tool, such as quantitative bone ultrasound, PQCT, or MRI bone density, to better assess the BMD in children. Volumetric BMD is a more sensitive indicator of mineral density and provides better clew and early diagnosis of the underlying bone condition especially for growing children with attention to their height and pubertal stage. Screening needs to be considered more regularly in the clinical practice especially with an underserved category such as children with ASD. The pediatric physician should evaluate other subsidizing factors such as calcium intake, sun exposure, vitamin D level, and physical activity in ASD children with AP-induced hyperprolactinemia, the AP could be modified if this is clinically doable. Abnormal prolactin levels should be addressed urgently. If this is not effective, a switch to an AP without prolactin-elevating property may be a helpful next step. Because we have controversial data on the AP-induced bone changes, more future studies on the effect of AP on bone mineralization and bone fracture in children with ASD are needed. The study should be designed to include a larger sample, equal gender proportion, larger representation of diverse ethnic and racial participants, with diverse psychiatric comorbidities and a wide range of AP medication. The study needs to include lifestyle modification habits, nutritional assessment, exercise, alcohol, and smoking habit to have a better understanding of this serious hidden complication of AP in vulnerable children population.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.