
Abstract
Three monoclonal antibodies—natalizumab (NTZ), ocrelizumab (OCR), and alemtuzumab (ALM)—are the mainstays for the treatment of both relapsing and progressive forms of multiple sclerosis (MS). Here, their safety in patients with MS is analyzed and compared for rational use, especially during the COVID-19 pandemic. All clinical studies published between 2016 and 2020 with the primary outcome of the occurrence of adverse events (AEs) with the use of NTZ, OCR, and ALM in the treatment of MS were systematically searched in the PubMed database. In this review, the percentage of patients reporting AEs was calculated and compared. The most common AEs associated with the use of NTZ, OCR, and ALM were infection and infestation. The percentage of patients reporting urinary tract infection, upper respiratory tract infection, and herpes was 16% using natalizumab, 7% using natalizumab and ocrelizumab, and 2% with ocrelizumab, respectively. The most common AEs, such as rashes, pyrexia, and influenza, were reported with ocrelizumab and alemtuzumab. Additionally, alemtuzumab was associated with immune thrombocytopenia (2%), respiratory infections (7%), and thyroid dysfunction (43%). All these data outcomes show that of the three monoclonal antibodies, natalizumab and ocrelizumab were associated with a reduced incidence of adverse events, making them a safer choice for MS.
Introduction
Multiple sclerosis (MS) is a chronic demyelinating disease affecting both brain and spinal cord. It is mainly an inflammatory autoimmune disorder mediated by stimulation and activation of circulating T-cell lymphocytes in the peripheral blood. 1 It affects more than 2.5 million people worldwide. 2 In India, its approximate rate of prevalence stands at 0.17 to 1.33 per 100,000 population.3, 4 Based on evidence-based treatment algorithms and the management guidelines from American Academy of Neurology (AAN) and The European Committee for Treatment and Research in Multiple Sclerosis/ European Academy of Neurology (ECRTRlMS/EAN), the pharmacotherapy of MS includes corticosteroids (methylprednisolone) and other disease-modifying treatments, such as interferons, glatiramer acetate, fingolimod, teriflunomide, dimethyl fumarate, and mitoxantrone. 5 However, these treatment selections have limited efficacy against relapsing remitting multiple sclerosis (RRMS) or primary progressive multiple sclerosis (PPMS) and lack target specificity. Their safety profile has severe shortcomings as they can induce the formation of neutralizing antibodies, neuroinflammation, myelotoxicity, gastrointestinal AE, and even sustained lymphopenia. 6 In recent developments, monoclonal antibodies, such as natalizumab (NTZ, 2004), alemtuzumab (ALM, 2014), ocrelizumab (OCR, 2017), have been approved by the US-FDA for RRMS and PPMS as they are highly specific and reduce the chances of drug interactions. 7
Natalizumab, approved for RRMS, is a fully humanized IgG1 that inhibits the transport of lymphocytes across the blood–brain barrier. The recommended dose is 300 mg, iv, every four weeks. Alemtuzumab, another humanized IgG, provokes cell-mediated lysis and rapid depletion of cluster of differentiation 4 (CD4), cluster of differentiation 8 (CD8) B, and natural killer (NK) cells. It is indicated for the treatment of RRMS and PPMS. The treatment is initiated with 12 mg/day × 5 days, followed by 12 mg/day × 3 days, after an interval of 12 months, and finally, 12 mg/day × 3 days. Ocrelizumab is a CD20-directed cytolytic antibody, which causes immunosuppression. It is approved for RRMS and PPMS. The treatment includes 300 mg, iv, followed by 300 mg, iv, after two weeks, and single dose of 600 mg, iv, every six months, thereafter.
The present pandemic due to the SARS-CoV-2 virus has globally caused an additional challenge in the management of autoimmune diseases including MS. These patients are prone to changes in the immune system, which may make them more vulnerable to viral infections and need to be closely monitored for treatment outcomes and safety. 8
TNF-α, interleukin (IL)-2R, and IL-6 are all elevated in COVID-19 patients, but lymphocyte subsets, including B cells, T cells, and natural killer cells, are low. The severity of the disease is worsened by an increase in inflammatory cytokines and a reduction in cell numbers. As a result, it is critical to examine the risk-to-benefit ratio of the monoclonal antibodies in order to rationally design a therapeutic regimen in the light of COVID-19.
Against this backdrop, the use of monoclonal antibodies has emerged as a novel strategy in the management of MS. However, they can be judiciously employed as an evidence-based clinical choice in light of the accurate assessment of their safety, tolerability, and efficacy. In the present study, the available data have been systematically reviewed and analyzed to assess their safety in the treatment of MS.
Methodology
Literature Search
A systematic study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement. The PubMed database was searched on January 29, 2021, with limits applied for Title/Abstract fields and period (2016–2020). The search terms included “Pharmacovigilance” OR “safety” AND “multiple sclerosis“ AND “Natalizumab” OR “Ocrelizumab” OR “Alemtuzumab.”
Data Extraction
Demography of Clinical Studies Belonging to Natalizumab, Ocrelizumab, and Alemtuzumab

Abbreviations: MAb, monoclonal antibody; AZA, azathioprine; FNG, fingolimod; GA, glatiramer acetate; IFN-β, interferon beta; DMF, dimethyl fumarate; MS, multiple sclerosis; PPMS, primary progressive multiple sclerosis; SPMS, secondary progressive multiple sclerosis; NR, not reported.
(N)* = Patients randomized in the recommended dose of monoclonal antibodies (MAbs).
Statistical Analysis
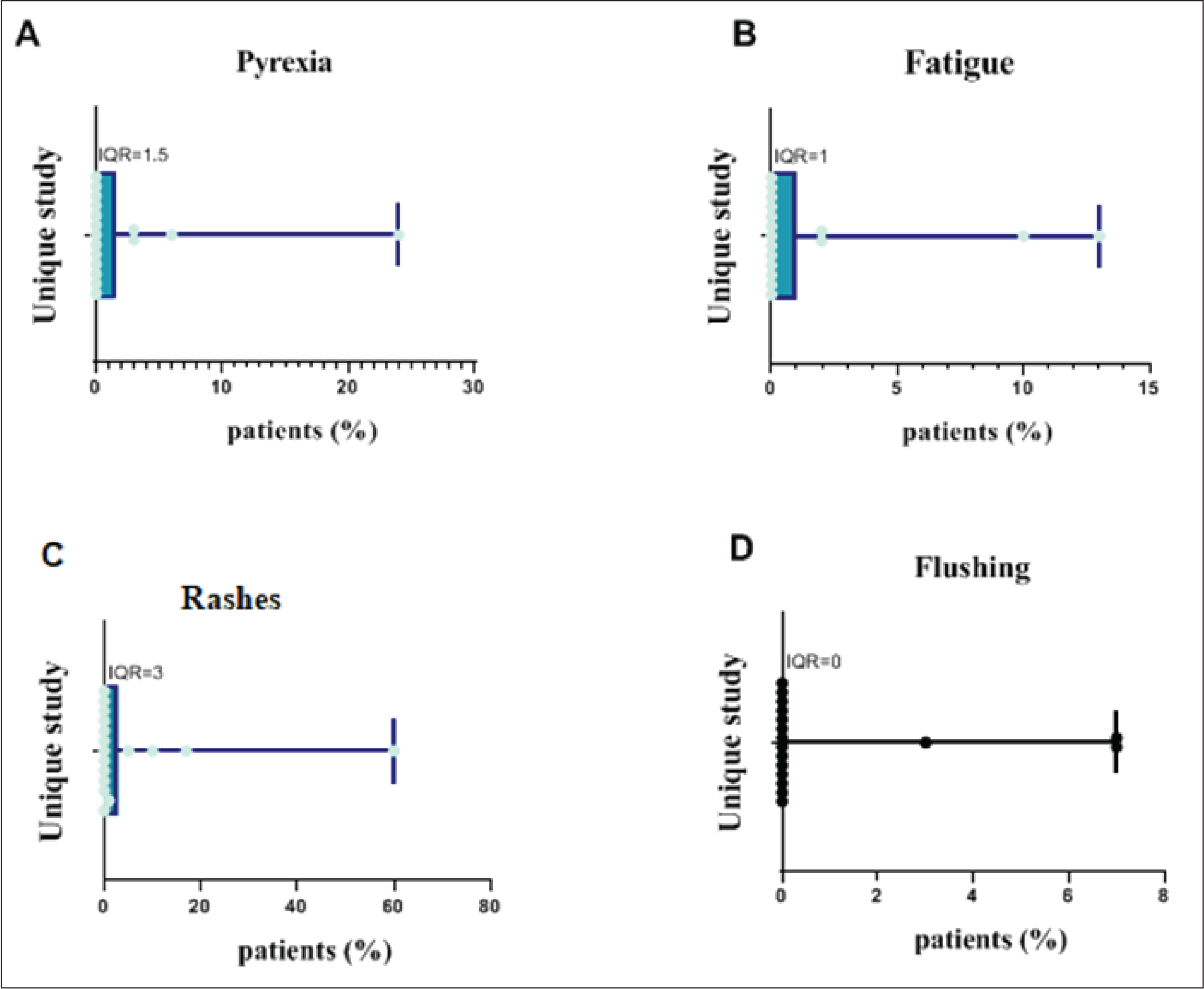
The association of reported AEs with the use of monoclonal antibodies was identified in each study and was statistically analyzed using Graph-pad Prism 9 software (Graph-StatsTechnology Ltd., Bangalore, India). The quartile (lower Q1 and upper Q3), median (Q2), and their interquartile range (IQR) were calculated and represented as box and whisker plots.
Results and Discussion
With no filters, the electronic search of the PubMed database identified 38 records, of which 21 were manually excluded based on the mentioned inclusion and exclusion criteria. The remaining 17 studies were included in this meta-analysis (Figure 1), which comprises data from a total of 7979 patients with MS. The total number of patients using NTZ, OCR, and ALM was 655, 3334, and 3990, respectively (Table 2). In this review analysis, 13 studies belonged to the patients with RRMS, followed by PPMS and secondary progressive multiple sclerosis. The patients were of either gender. The mean age ranged between 30 and 47 years, whereas the mean range of duration of MS was 2.9 to 16.9 years. Prior to starting the monoclonal antibody treatment, the previous treatment was ceased.
PRISMA Flowchart.

Comparison of Reported AEs Among Natalizumab, Ocrelizumab, Alemtuzumab
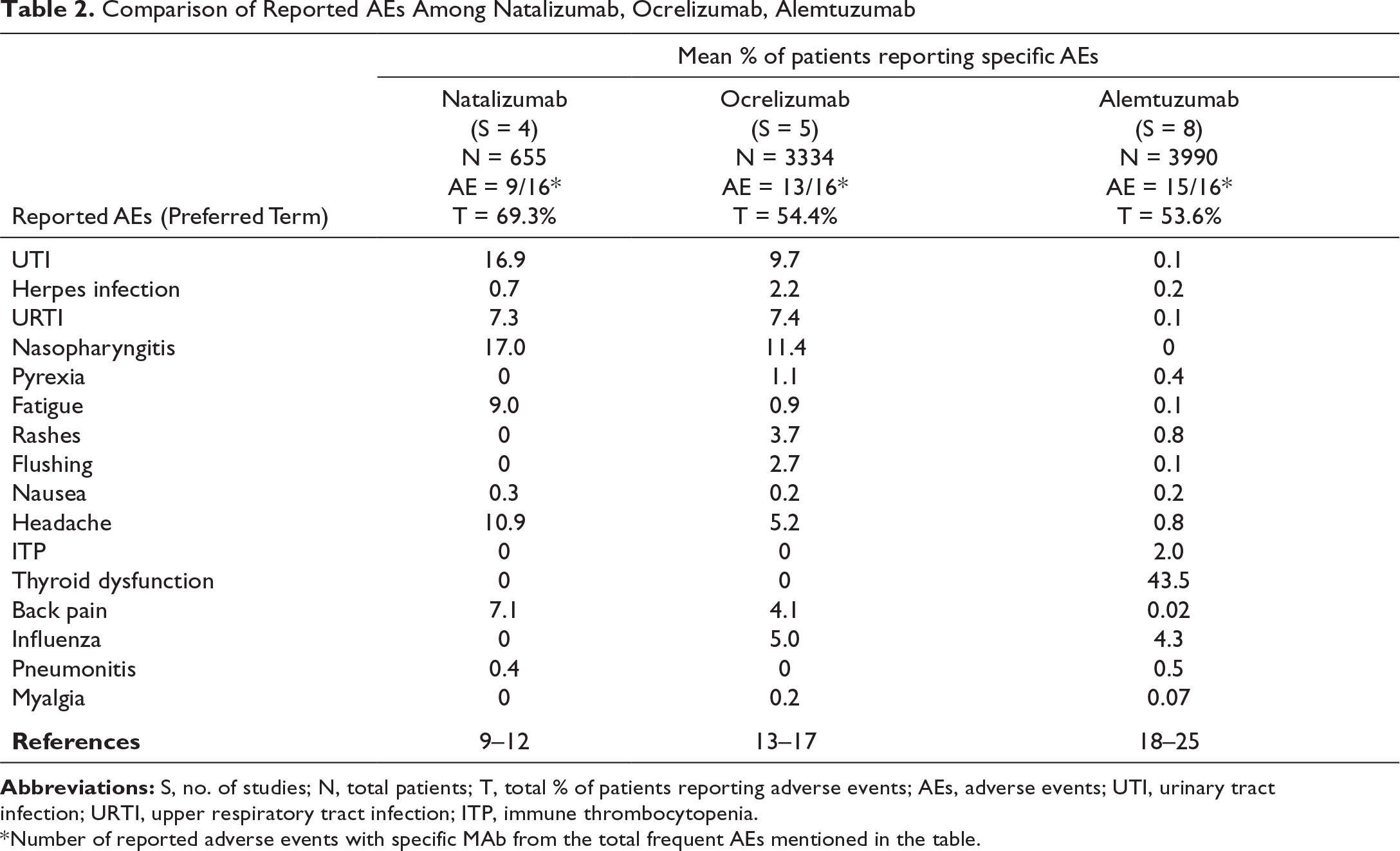
Abbreviations: S, no. of studies; N, total patients; T, total % of patients reporting adverse events; AEs, adverse events; UTI, urinary tract infection; URTI, upper respiratory tract infection; ITP, immune thrombocytopenia.
*Number of reported adverse events with specific MAb from the total frequent AEs mentioned in the table.
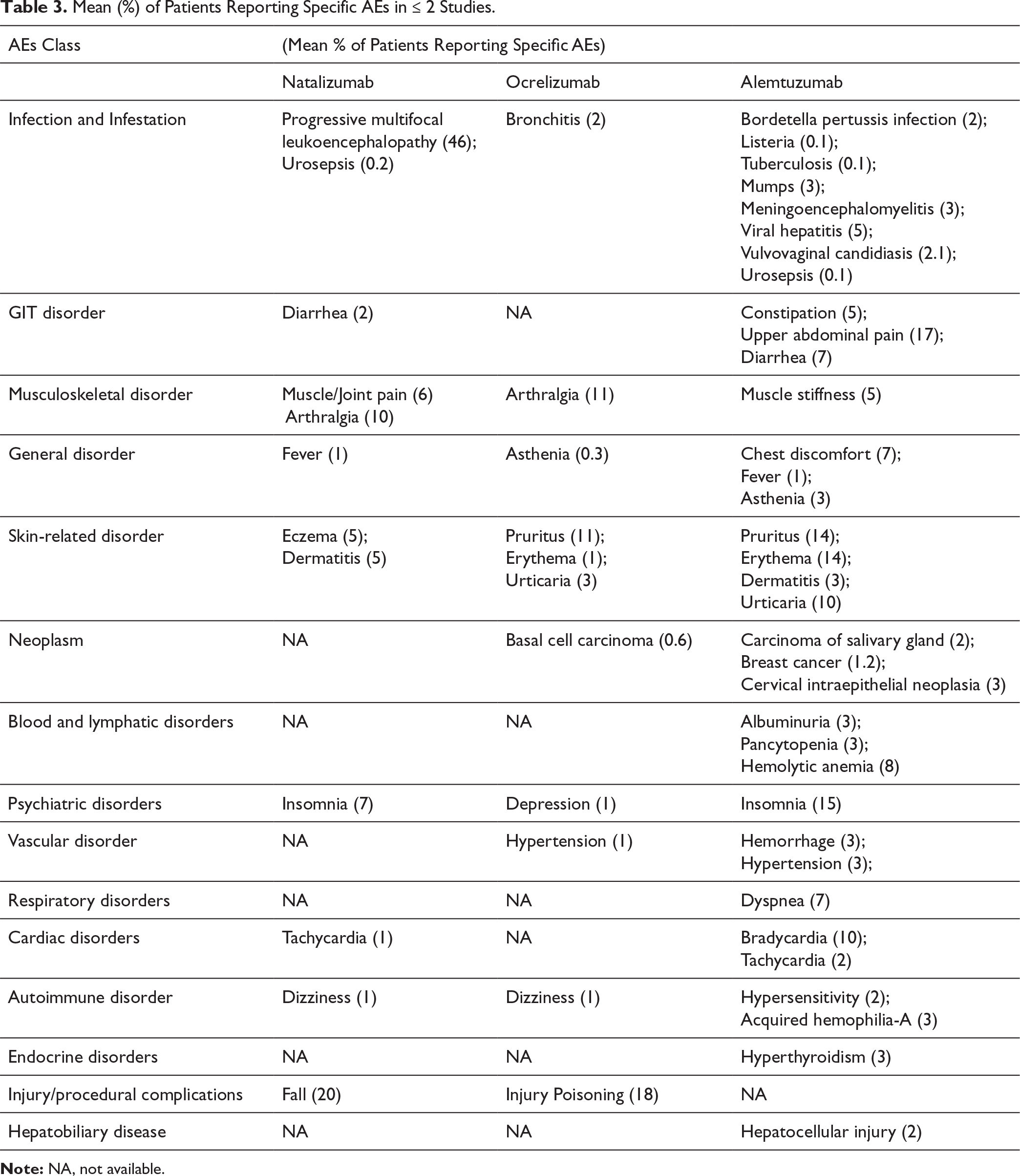
Mean (%) of Patients Reporting Specific AEs in ≤ 2 Studies.
The AEs related to infection and infestations were reported in 94% of studies. These AEs were mostly reported with NTZ and OCR; however, their severity was not as high. Urinary tract infection was reported in 16.9%, 9.7%, and 0.1% of patients using NTZ, OCR, and ALM, respectively (Table 2). Herpes infection was reported in 0.7%, 2.2%, and 0.2% of patients using NTZ, OCR, and ALM, respectively (Table 2). Upper respiratory tract infection was reported in 7.3%, 7.4%, and 0.1% of patients using NTZ, OCR, and ALM, respectively (Table 2). Nasopharyngitis was reported in 17%, 11.4%, and 0% of patients using NTZ, OCR, and ALM, respectively. The IQR of urinary tract infection, herpes infection, upper respiratory tract infection, and nasopharyngitis was calculated as 9.5, 3, 9.5, and 17.5%, respectively (Figure 2a–d).

In the general disorders, fatigue was reported in 9.0%, 0.9%, and 0.1% of patients using NTZ, OCR, and ALM, respectively (Table 2). The AE of rashes was reported in 0%, 3.7%, and 0.8% patients using NTZ, OCR, and ALM, respectively. Similarly, flushing was reported by 0%, 2.7%, and 0.1% of patients using NTZ, OCR, and ALM, respectively (Table 2). Pyrexia was reported in 23% of studies, with an IQR of 1.5% (Figure 3a). The IQR of fatigue, rashes, and flushing was 1.0%, 3%, and 0%, respectively (Figure 3b–d).
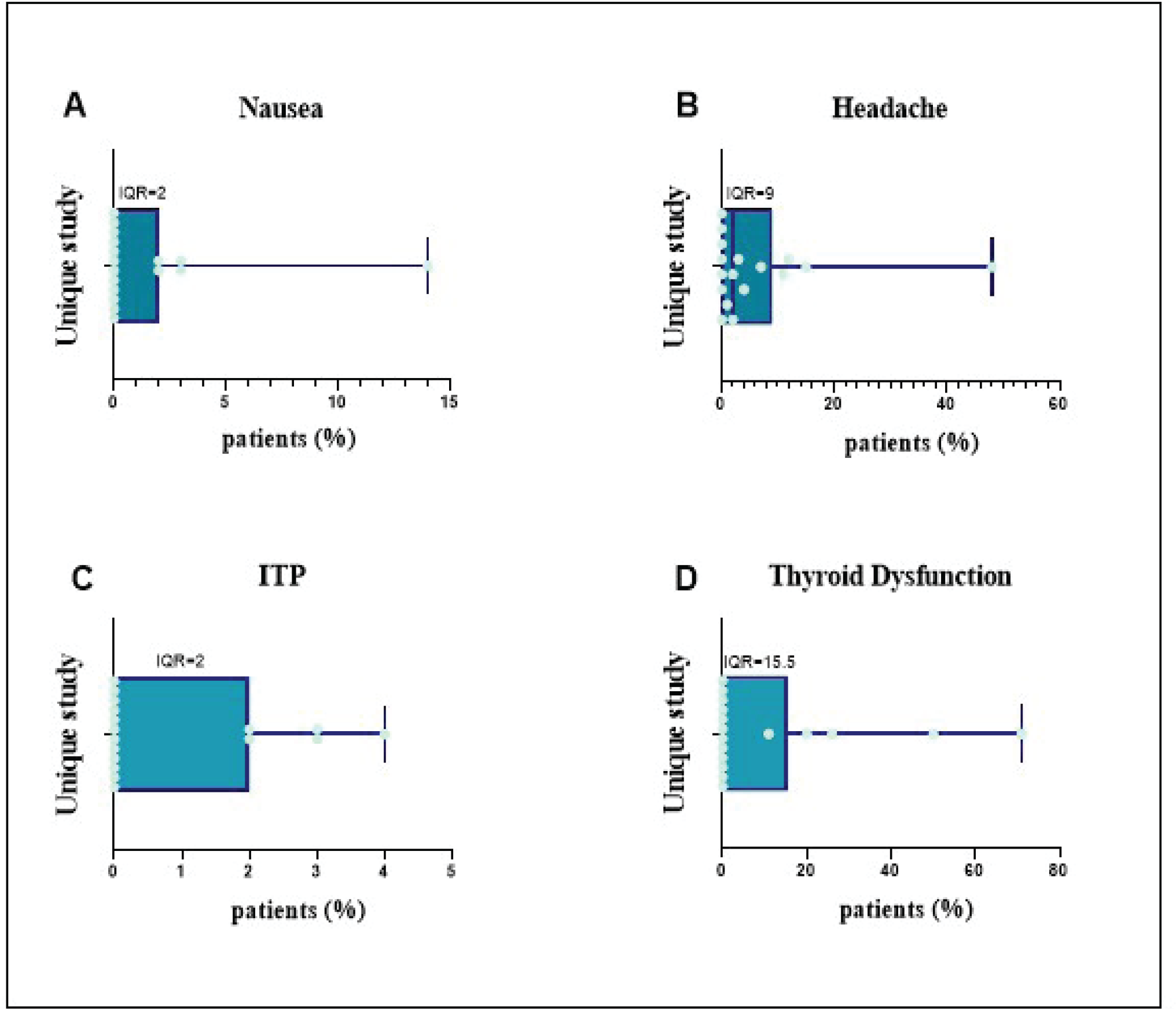
Nausea was the prominent GIT disorder reported in 0.3%, 0.2%, and 0.2% of patients using NTZ, OCR, and ALM, respectively, with an overall IQR of 2% (Table 2, Figure 4a). Headache was reported in 10.9%, 5.2%, and 0.8% of patients using NTZ, OCR, and ALM, respectively (Table 2). Of the three monoclonal antibodies, ALM was majorly associated with severe AEs, such as immune thrombocytopenia (ITP 2%) and thyroid dysfunction (43%). On the other hand, OCR and NTZ, unlike ALM, had no severe adverse events recorded (Table 2). The IQR for headache, ITP, and thyroid dysfunction was calculated as 9.0%, 2%, and 15.5% (Figure 4b–d).
Other adverse events, such as back pain, were reported by 7.1%, 4.1%, and 0.02% of patients using NTZ, OCR, and ALM, respectively (Table 2). Influenza was reported by 0%, 5%, and 4.3% of patients using NTZ, OCR, and ALM, respectively (Table 2). Pneumonitis was reported in 0.4%, 0%, and 0.5% of patients using NTZ, OCR, and ALM, respectively (Table 2). Myalgia was reported in 0%, 0.2%, and 0.07% of patients using NTZ, OCR, and ALM, respectively (Table 2). The calculated IQR for back pain, influenza, pneumonitis, and myalgia was 1.0%, 6.0%, 0%, and 0%, respectively (Figure 5a–d).

The AEs related to cardiac, hepatobiliary, psychiatric, and respiratory disorders were the least common. Of the three monoclonal antibodies, ALM was also frequently associated with the less common AEs that were related to infections and neoplasms, such as carcinoma of the salivary gland (2%) and breast cancer (1.2%), whereas NTZ and OCR appear to be safe.
The incidence of AEs related to NTZ may be because of the production of antibodies against NTZ, which in turn suppresses the immunity. 26 The OCR is a CD20 antibody that may cause reductions of immunoglobulins, primarily IgG, and cause antibody-dependent cell-mediated cytotoxic effects, which may contribute to the risk of infections. 27 The ALM is associated with an increased risk of ITP and thyroid dysfunction because of immediate cytokines release syndrome following intravenous administration, which causes significant elevation of IL-6, TNF-α, and interferon-gamma (IFN-γ) that forms a cytokine storm and potentially increases the risk of these side effects. 28
Previously, meta-analysis has been conducted to determine the safety of various monoclonal antibodies for MS. In contrast to our study, Xu et al. 29 compared monoclonal antibodies with placebo in RRMS and found that they had less significant AEs. In a similar study, McCool et al. 30 investigated OCR and found that it had a better or equivalent safety profile when compared with other disease-modifying medicines for RRMS across all endpoints. In a similar study, Lucchetta et al. 31 found that NTZ, OCR, and ALM showed higher efficacy than other disease-modifying medicines, but more meta-analysis is needed to understand the prevalence of AEs in order to assess their safety profile.
Rapidly increasing cases of MS worldwide has created an ongoing research interest for developing new therapies for MS. Different biological treatments have been studied and tested, and among them, monoclonal antibodies are working as a pillar for MS treatment. Moreover, new advancements in the production of monoclonal antibodies are being incorporated to optimize their safety and tolerability profiles, which is a promising factor.
This review provides a comprehensive overview of the safety profile of approved monoclonal antibodies for MS. This information can potentially assist the clinicians in the selection of the most appropriate therapeutic intervention considering the COVID-19 pandemic. Natalizumab and ocrelizumab, according to our analysis, are the preferable therapeutic options than other licensed monoclonal antibodies for MS treatment, especially during COVID-19, because they were found to be associated with a lower incidence of infections, particularly respiratory infections.
Footnotes
Acknowledgment
The authors thank Arshvir Kaur, Department of Pharmacology, DIPSAR, DPSRU for helping in manuscript formatting and proofreading.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.