
Abstract
Xylometazoline, a sympathomimetic available as over the counter drug, acts as a nasal decongestant and has been reported as an independent risk factor for hemorrhagic and ischemic stroke. The chronic use of xylometazoline leads to either increased release of more potent vasoconstrictor norepinephrine in the presynaptic region, or acts directly on central adrenoreceptors which leads to dysfunction resulting in chronic progressive vasculopathy that manifests as an ischemic stroke. Sympathomimetics also activate 12-lipoxygenase pathways which induce proliferation and migration of vascular smooth muscle cells. 12-lipoxgenase also plays a significant role in regulating the degree and stability of platelet activation, as its activation significantly strengthens platelet activation and uncontrolled platelet activation, which may lead to myocardial infraction and stroke. The present case reports a rare case of young adult suffering from isolated left medial cerebellar peduncle infarct related to the chronic use of xylometazoline. Acute cerebellar stroke is rare, especially in young adults and represent only 3% of total ischemic and hemorrhagic strokes. Clinical symptoms, patient age at the onset of stroke, and lesion size had no significant effect on the clinical outcome. Symptoms are frequently underestimated and misdiagnosed which further lead to serious complications and poor functional outcomes.
Introduction
Xylometazoline is a sympathomimetic decongestant, which is a widely used over the counter (OTC) drug in conditions such as common cold, allergic sinusitis, and rhinitis. Being lipophilic in nature, it gets absorbed into the blood vessels and passes easily through the blood–brain barrier into the central nervous system. It acts on adrenergic (α-2) receptors and causes vasospasm, and it also activates the 12-lipoxygenase pathway which induces vascular smooth muscle cell proliferation and migration. Chronic use of xylometazoline can also be an independent risk factor for ischemic and hemorrhagic stroke. 1
Acute cerebellar stroke is a relatively rare subtype of acute stroke, representing 3% of total ischemic and hemorrhagic strokes. Symptoms are frequently underestimated or misdiagnosed. Imaging of cerebellar stroke is also challenging and may be difficult or impossible to discern on computed tomography. Missed diagnosis is not only detrimental but can also lead to serious complications and poor functional outcomes in patients. 2
Here we report a rare case of a young adult diagnosed of isolated left medial cerebellar peduncle infarct related to the chronic use of xylometazoline.
Case Report
A 25-year-old man with no history of systemic illness presented to the outdoor patient department (OPD) of a tertiary care center with complaints of slurred speech, difficulty in swallowing, blurring of vision, confusion, headache, and difficulty in walking since one week. The patient complained of disturbed sleep pattern, emotional instability, mood swings, and continuous fear of death.
On physical examination, the vital signs were normal including blood pressure (114/72 mmHg), pulse rate (90/min), and SPO2 (97%).
On neurological examination, the patient was well oriented (Glasgow coma scale-E5V4M6), with intact memory and cognition. There was no nystagmus, and the cranial nerve examination was normal. There was right side motor weakness with hypotonia in the right arm and leg, and moderate weakness (3/5), but he could stand with little support. The patient had an asymmetrical gait, walked fast taking small steps, and fear of falling. There was knee hyperextension and lack of heel rise. Babinski’s sign was absent. Clinical assessment done by using the Modified International Cooperative Ataxia Rating Scale (MICARS) showed a clinical score of 55 out of 100 and the Modified Rankin Scale showed a clinical score of 3 suggestive of moderate disability.
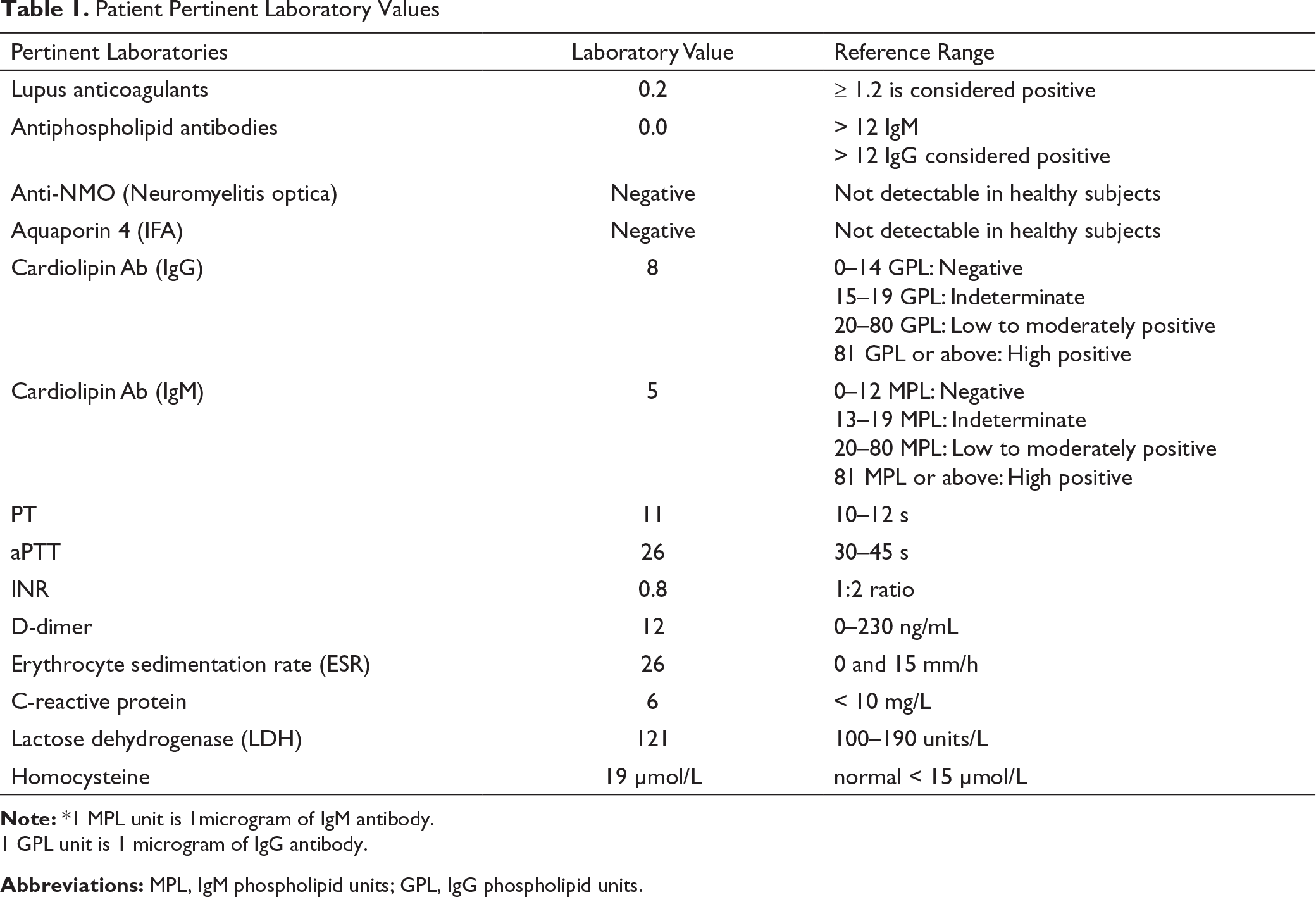
Patient Pertinent Laboratory Values
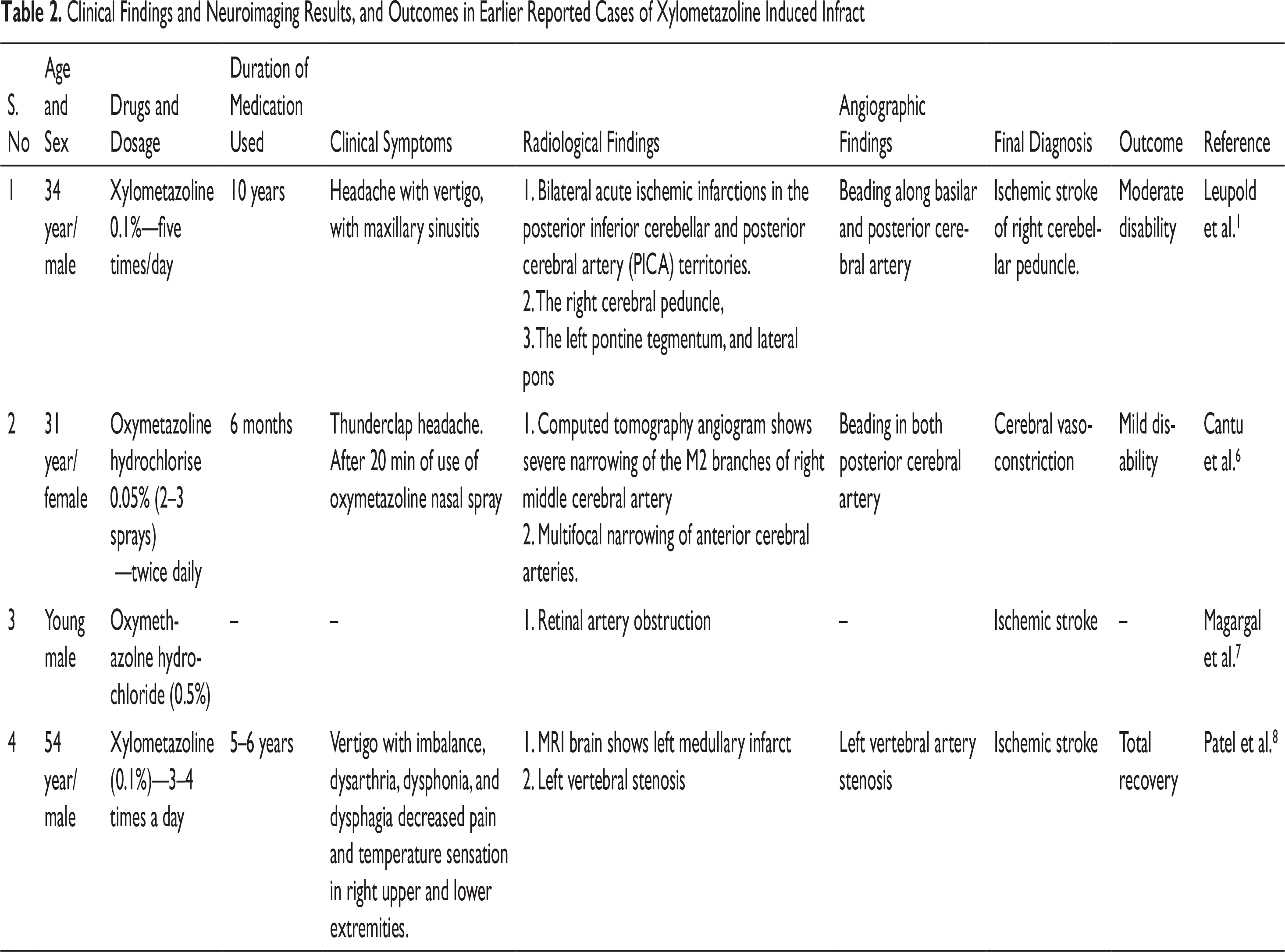
Clinical Findings and Neuroimaging Results, and Outcomes in Earlier Reported Cases of Xylometazoline Induced Infract
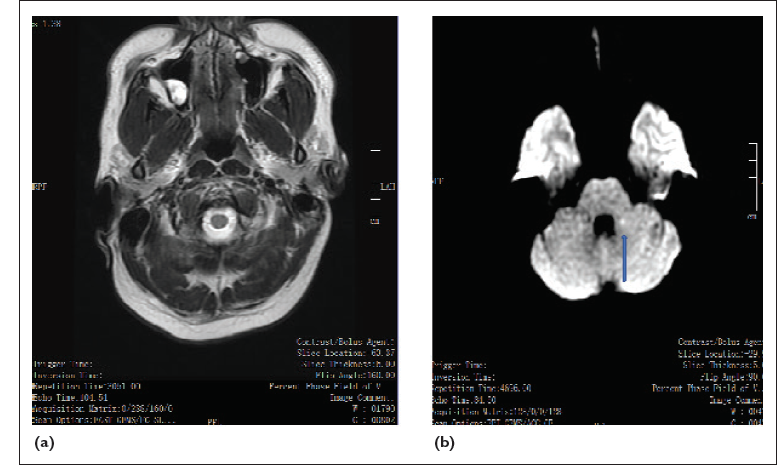
(a) MRI Axial T1-Weighted Image Shows Right Maxillary Sinusitis and Polyp (b) MRI Brain With Diffusion-Weighted Imaging (DWI), Showing Small Focus of Mild Diffusion Restriction With Mildly Reduced Apparent Diffusion Coefficient (ADC) in the medial Aspect of the Left Medial Cerebellar Peduncle.
Electroencephalography of patients showed focal slowing of delta waves in the left temporal region in lead T4, O2, and C4. Nerve conduction velocity study of right upper and lower limbs showed conduction delay (normal 50 to 60 mEV).
A lumbar puncture was done and cerebrospinal fluid (CSF) sent for routine microscopy and antibody screening. CSF studies showed lymphocytic pleocytosis (WBC 110/mm 3 ; normal < 5 µL of CSF), glucose level of 86 mg/dL, and protein level of 57 mg/dL. CSF studies were negative for both bacterial and viral cultures. Antibody screening for N-methyl-D-aspartate receptor (NMDA-R), glutamic acid decarboxylase, contactin-associated protein-like 2 (CASPR2), leucine-rich, glioma inactivated 1 (LGI 1) antibodies, ganglioside antibodies and a panel of anti-neuronal antibodies in serum and CSF were negative. Anti-glycine receptor and anti-dipeptidyl-peptidase-like protein 6 (DPPX) antibodies were negative.
Past history revealed that the patient have been self medicating with Otrivin (xylometazoline 0.1%) nasal spray (2–3 puffs) regularly for rhinitis for the past three years before going to bed. There were no other risk factors like smoking and alcohol intake. On the Naranjo’s causality assessment scale, the adverse event score of 8 indicated a “probable” causality relation to xylometazoline.
Use of the nasal spray was discontinued. Tab ecosprin 150 mg, tab atorvastatin 20 mg, and tab deflazacort 30 mg once daily were started, maintaining an INR between 1.5 and 2.0 (normal 2.0 to 3.0 in a patient on antithrombotic drugs). The patient underwent physical and occupational therapy and achieved significant improvement in his clinical symptoms approximately after 6 weeks of treatment. Functional recovery and residual disability outcomes were rated using MRS = 2 and Glasgow Outcome Scale (GOS). There was no significant problem in daily activities after 10 weeks from the day when treatment started.
Discussion
Ischemic infarct is an example of a medical condition with multiple risk factors, which requires a complete detailed history and exhaustive laboratory tests to find out the cause. In younger adults, these efforts may not be always sufficient as vascular risk factors can be absent many times. The diagnosis is mostly made by the exclusion of risk factors. Vascular malformations and arterial hypertension are the most common causes of cerebral infarct in young adults, while smoking and hypercholesterolemia are the major risk factors. 3 Hemorrhage and infarct because of the use of easily available OTC sympathomimetic drugs as nasal decongestants are silent, hidden health care problems, as they show a rare association.1, 4
Sympathomimetic drugs are further classified as beta-phenylethylamine or imidazole derivatives a class of sympathomimetic drugs such as naphazoline, oxymetazoline, and xylometazoline. They are widely used OTC drugs, for the treatment of common cold, allergic rhinitis and sinusitis. Commonly encountered side effects of these drugs are oral and nasal dryness, burning and stinging sensation in the nose, nasal dripping, and sneezes. Tremors, headache, dizziness, palpitation, and anxiety are less pronounced adverse effects. 4
Several mechanisms by which sympathomimetic drugs cause cerebrovascular complications have been proposed. 1 In this case, the most presumable mechanism is vasoconstriction of cerebral arteries induced by vascular smooth muscle cell proliferation and migration caused because of chronic use of xylometazoline. 5 Xylometazoline causes reduction in edema of the nasal mucosa by directly acting on adrenergic α-1, α-2, and β receptors located diffusely in the cerebral vascular walls. Xylometazoline also releases most potent vasoconstrictor norepinephrine (NE), which potentiates adrenergic tone and results in vasospasm of cerebral arteries. The patient could have had an ischemic stroke because of the reversible cerebral vasoconstriction syndrome (RCVS) secondary to central adrenergic receptor stimulation by xylometazoline. In RCVS, there is reversible vasospasm of intracerebral arteries caused by disturbance in vascular tone.
It is possible that sudden increase in the dose and frequency of sympathomimetic drugs can result in the development of stroke in a shorter time duration (within a week). However, in this case ischemic cerebral stroke has occurred after chronic use of xylometazoline for three years without any modification in dosage. Similar findings have been reported previously where patients developed stroke after chronic use of a sympathomimetic nasal decongestant drug without any change in dosage regimens.1, 6, 7 Hemorrhagic stroke associated with sympathomimetic drugs usually occurs after short term use because of accelerated hypertension or hypertension crisis, thereby leading to intracerebral hemorrhage. The chronic use of xylometazoline leads to either increased release of one of the most potent vasoconstrictor NE in the presynaptic region, or it acts directly on central adrenoreceptors which leads to dysfunction, resulting in chronic progressive vasculopathy which further manifests as an ischemic stroke. A total of four cases have been reported, out of which three had a brain infarction while one experienced retinal artery occlusion (Table 2).1, 6–8 The chronic use of sympathomimetics activates 12-lipoxygenase pathways which induce increased proliferation and migration of vascular smooth muscles.9, 10 12-lipooxgenase also plays a significant role in regulating the degree of stability and uncontrolled platelet activation, as the activation of 12-lipoxygenase significantly strengthen platelet activation which may lead to myocardial infarct. 11
Similar focal vasculopathy of sinus and nasal mucosa causes rebound nasal congestion on stopping the use of nasal decongestants, resulting in chronic and continuous repetitive use of the nasal decongestants by patients. This rebound nasal mucosal congestion and inflammation is described as rhinitis medicamentosa caused mainly by prolonged use (7 to 10 days) of sympathomimetic decongestants. 12 Similar findings are present in this case as the patient has right maxillary sinusitis and polyps extending up to the right nasal cavity.
In this case, MRI diffusion study showed evidence of a small focus of mild diffusion restriction with mildly reduced apparent diffusion coefficient value suggestive of left medial cerebellar peduncle (MCP) which in turn is suggestive of subacute lacunar infarct. MCP is the main afferent pathway composed of white matter fibers originating from the contralateral pontine nuclei. The pontine nuclei are an intermediary gray matter scattered in the basal pons and part of the cortical-ponto-cerebellar pathway (closed loop communication between the cerebellum and precentral/prefrontal cortex which control action of motor tasks, planning, and initiation of movements). 13 The cerebellum has a high ratio of afferent/efferent pathways (40:1), with the small superior cerebellar peduncles. The only efferent fibers connecting the dentato nuclei to the cortex pass through the dentate-rubro-thalamic tracts. In general, the cerebellar pathways decussate twice, once at the level of the pons (crossing pontine fibers) and other at the level of the inferior colliculi in the tegmentum (decussation of the superior cerebellar peduncles). MCP is supplied by the anterior inferior cerebellar artery (AICA) and the superior cerebellar artery. Isolated AICA infraction (thromboembolic or secondary to severe atherosclerotic disease of basilar arteries and branches) is an uncommon event. There is damage to the axons because of the loss of antegrade or retrograde input with subsequent myelin breakdown and end-stage gliosis/volume loss resulting in Wallerian degeneration. In this patient, there is restricted diffusion in the involved left cerebral peduncle, thus the clinical signs are ipsilateral to MCP lesion resulting in right side limb ataxia, and facial weakness.
Clinical symptoms of cerebellar stroke in young patients are subtle and are not often recognized or misdiagnosed. 14 It is possible that isolated cerebellar stroke can present with a low score in the National Institute of Health Stroke Scale (NIHSS). Patient age at the onset of stroke and lesion volume had no significant effect on the clinical outcome and symptoms of the lesion after acute brain ischemia. This may be because of the involvement of particular anatomical structures integrated into complex functional networks. 15 Similarly, in this patient, symptom severity and rate of clinical recovery were significantly influenced by lesion structure and location in the superior cerebellar artery supplying area, and thus, the patient recovered quickly.
Sympathomimetic nasal sprays are easily available as OTC medicines. They can be an independent risk factor for hemorrhagic and ischemic strokes, and thus, should be considered at the time of evaluation of a stroke. OTC drugs can act as a double-edged sword and require due consideration for patient safety. Measures to educate patients regarding adverse effects of such OTC drugs are highly recommended.
Declaration of Patient Consent
The authors certify that they have obtained patient consent. In the form the patient has given his consent for the use of clinical information and images to be reported in the journal. The patient understands that their name and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Key Points
Thunderclap headache warrants immediate clinical evaluation with appropriate laboratory and radiological investigations. Reversible cerebral vasoconstriction, infarct, and hemorrhage are the most common causes.
Acute or chronic use of sympathomimetic vasoactive substances (e.g., adrenergic agonists and serotonergic drugs) are known risk factors for their reversible cerebral vasoconstriction activity.
A brief counseling should be given to all patients prescribed or using nasal decongestants of their own about the risk of rhinitis medicamentosa, hypertension, and reversible cerebral vasoconstriction syndrome.
A strict warning should be given to the patient that regimen should not be used for more than 3 to 5 days without the consent of the treating physician.
Ethical Statement
Written informed consent was obtained from the patient for the publication of this case report.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.