
Abstract
Background:
Myopericytoma is a typically benign, slow-growing soft tissue tumour that originates from pericytes, the contractile cells surrounding blood vessels. While they can appear in both appendicular and axial skeletons, the rarity and indolent nature of the condition can be a clinical challenge.
Objective:
The purpose of this study is to review the radiological findings of myopericytomas in a series of cases at a tertiary referral centre, identify characteristic imaging patterns and aid in the accurate diagnosis of suspected lesions.
Patients and Methods:
A retrospective study was conducted and 62 histopathologically proven cases of myopericytoma were identified at our tertiary orthopaedic oncology institution. Of these, 51 cases were included in the final cohort and analysed. Each case was reviewed for patient demographics, lesion morphology and magnetic resonance imaging (MRI) signal characteristics.
Results:
Of 51 cases, most were located in the subcutaneous soft tissues. All lesions were solitary, with a mean size of 2.06 cm. On imaging, all lesions were isointense to muscle on T1-weighted sequences and hyperintense on fluid-sensitive sequences, exhibiting variable patterns of post-contrast enhancement. No significant signal drop was observed on chemical shift imaging and no diffusion restriction was noted on diffusion-weighted imaging (DWI).
Conclusion:
Myopericytoma is a rare soft tissue tumour with certain distinctive imaging features which can aid in early recognition and accurate diagnosis.
Introduction
Myopericytomas are rare, benign soft tissue tumours originating from pericytes, the contractile cells surrounding blood vessels and lie on the same histological spectrum as myofibroma.[1] Although variable, the histopathology is reasonably well-described, characterised by circumscribed but non-encapsulated concentric perivascular proliferation of spindle-shaped cells containing collagenous or myxoid stroma.[2] Immunohistochemistry often aids delineation with cellular expression of alpha-smooth muscle actin, amongst other markers, favouring the diagnosis.[3]
The tumour is typically seen in adults with a predilection for the subcutaneous tissues of the appendicular skeleton and head and neck.[4] Rare cases of deeper and even visceral myopericytomas have been described in the literature. They typically manifest as a painless, slow-growing mass measuring up to 2 cm in size.[5] Multicentric occurrence and malignant behaviour have been described, but are uncommon.[6]
Although reasonably well-described histopathologically, the literature on the specific imaging features of myopericytoma is relatively scant. Most published articles are case reports or case reviews with small case series, describing the lesions as showing low signal intensity on T1-weighted imaging and high signal intensity on T2-weighted MR imaging, with the lesions seen in specific areas such as Kager’s fat pad, the ear, breast and parotid gland.[7–10] Some studies identify peripheral enhancement on post-contrast study as a characteristic, whereas others describe internal homogenous or heterogeneous enhancement as a characteristic, rendering this an area of uncertainty.[5] Furthermore, opposed-phase imaging and diffusion-weighted imaging (DWI) characteristics have not been assessed in the available literature.
Patients and Methods
Study Design and Patients
This retrospective study was conducted at a tertiary orthopaedic oncology centre and was approved by the local ethics committee. All biopsy-proven myopericytomas over 17 years were identified from the institutional pathology database. Radiology database (Radiology Information System, Picture Archiving and Communication System and Computerised Radiology Information System) were searched for collaborative patients using the keywords ‘myopericytoma’ and ‘tumour’. The data collected were correlated with histopathology and laboratory records. Patient demographics, clinical characteristics, and complementary imaging were recorded for the eventual analysis. These were reviewed by a junior registrar-level radiologist and a consultant musculoskeletal radiologist with over 10 years of experience.
Inclusion and Exclusion Criteria
All biopsy-proven myopericytoma cases with available magnetic resonance imaging studies were included in the study, while cases without imaging were excluded.
Data Collection and Data Analysis
The data recorded included patient demographics (age, gender), site of lesion, morphological features (size, location), MRI signal characteristics of the lesion on T1-weighted, fluid-sensitive sequences (either T2FS or STIR), DWI, chemical shift imaging and post-contrast studies. Data was collected and analysed using a Microsoft Excel spreadsheet.
Statistical Analysis
SPSS version 24 software (International Business Machines, Armonk, NY) was used for statistical analysis. Descriptive statistics was undertaken. Mean and standard deviation or median (range) were used to summarise the data.
Results
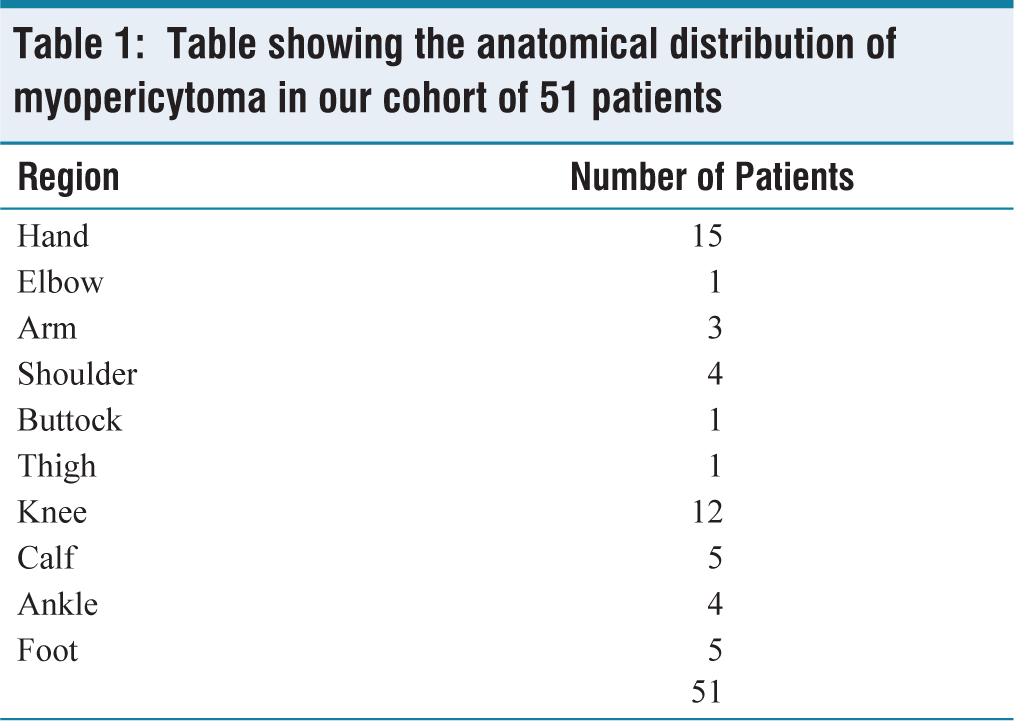
In total, 62 histopathologically proven cases of myopericytomas were identified for the study. Of these, 11 cases were excluded from analysis due to the unavailability of corresponding imaging studies, resulting in a final cohort of 51 cases for detailed radiological evaluation. The final cohort consisted of 35 males and 16 females, with a mean age of 61.7 years (range 13–93 years). All lesions were solitary and located in the appendicular skeleton, with 24 cases in the upper limb and 27 in the lower limb [Table 1]. The mean maximum diameter of the lesions was 2.06 cm (SD = 1.73), with the largest lesions observed in the lower limb (mean maximum diameter of 2.29 cm).
Table showing the anatomical distribution of myopericytoma in our cohort of 51 patients
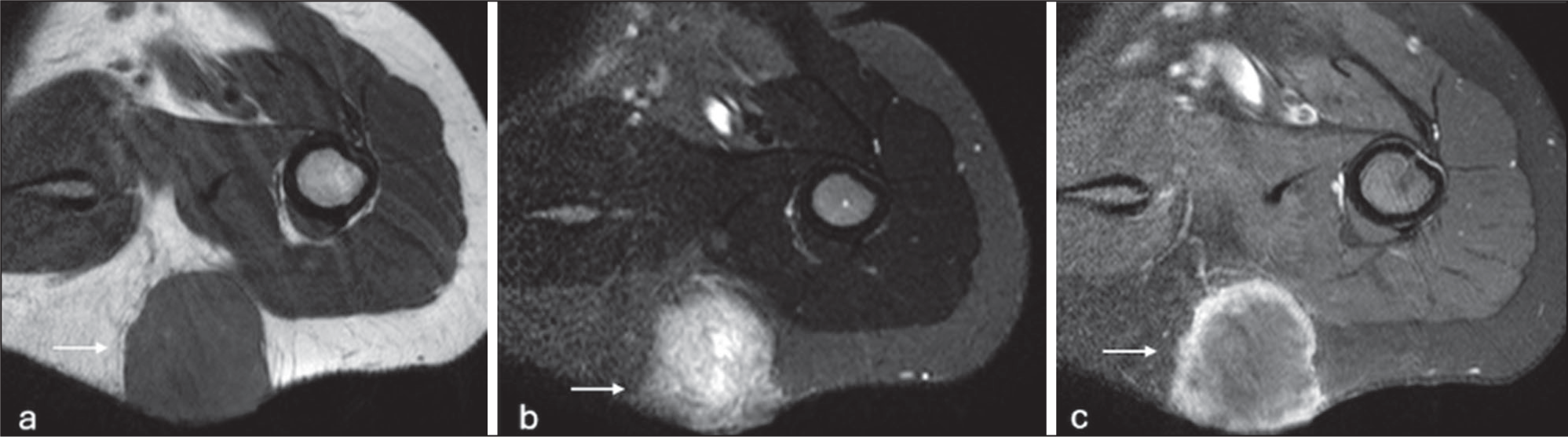
In terms of signal characteristics, all lesions were isointense to muscle on T1-weighted sequences. Fluid-sensitive sequences were performed in 39 cases, with lesions in 29 of these cases showing high homogenous signal intensity relative to the muscle and 10 of them demonstrated heterogeneous signal [Figures 1–5].
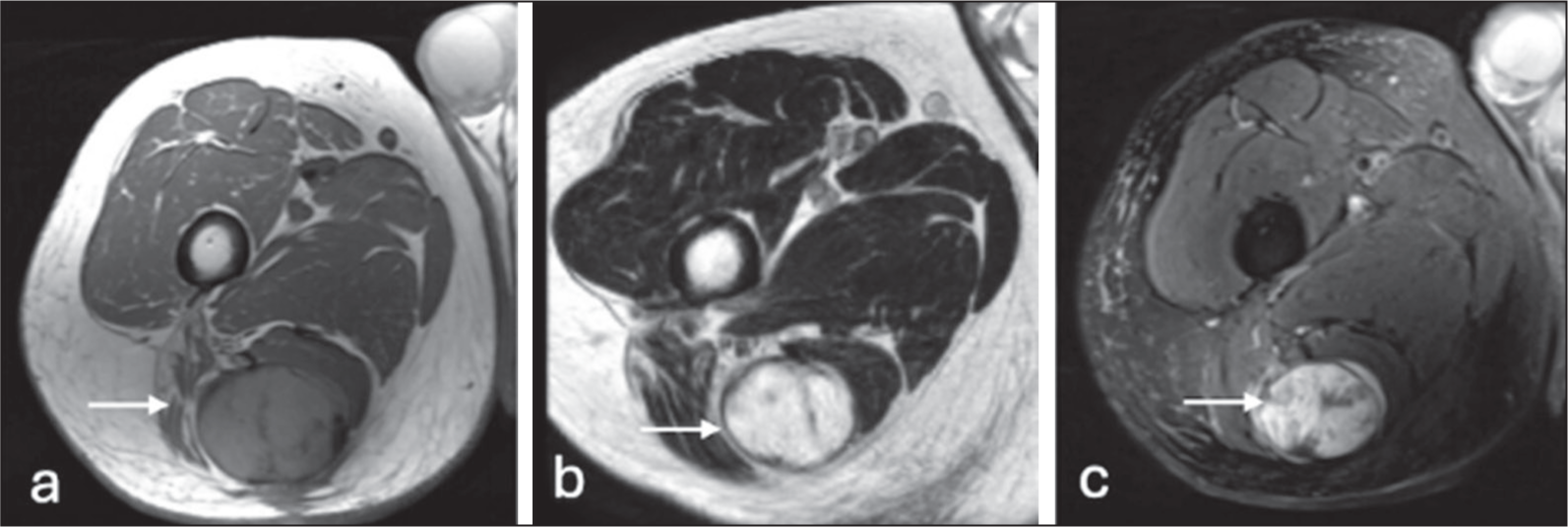
Axial T1-weighted (a), T2-weighted (b) and STIR (c) showing myopericytoma within the hamstring muscles (arrow)
Longitudinal ultrasound (a), power Doppler (b), axial T1-weighted (c) and fat-suppressed T2-weighted (d) images demonstrating a myopericytoma within the subcutaneous planes (arrow)

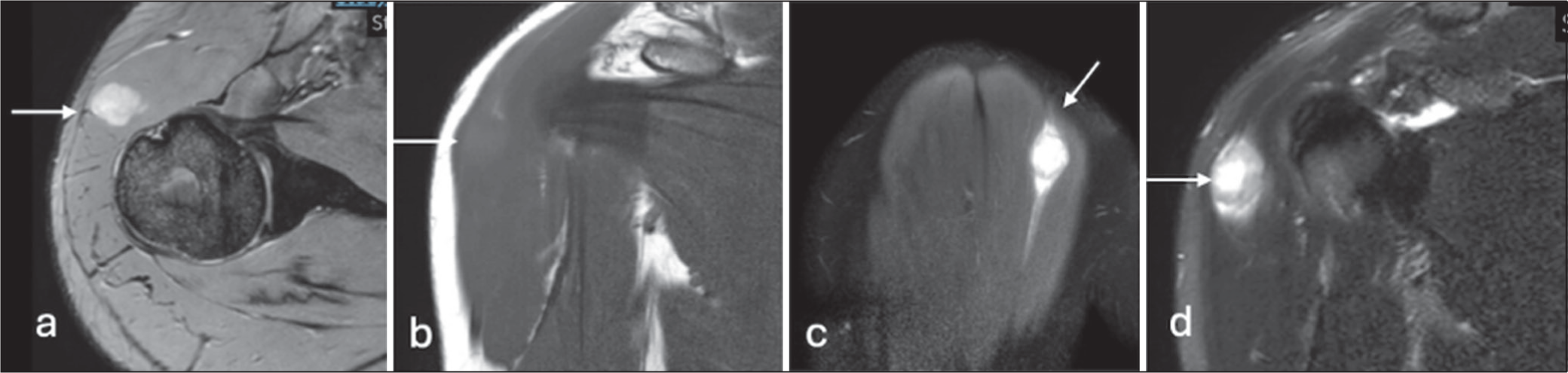
Axial T2-weighted (a), coronal T1-weighted (b), sagittal proton density fat-saturated (c) and coronal proton density fat-saturated (d) images demonstrating a myopericytoma within the deltoid muscle (arrow)
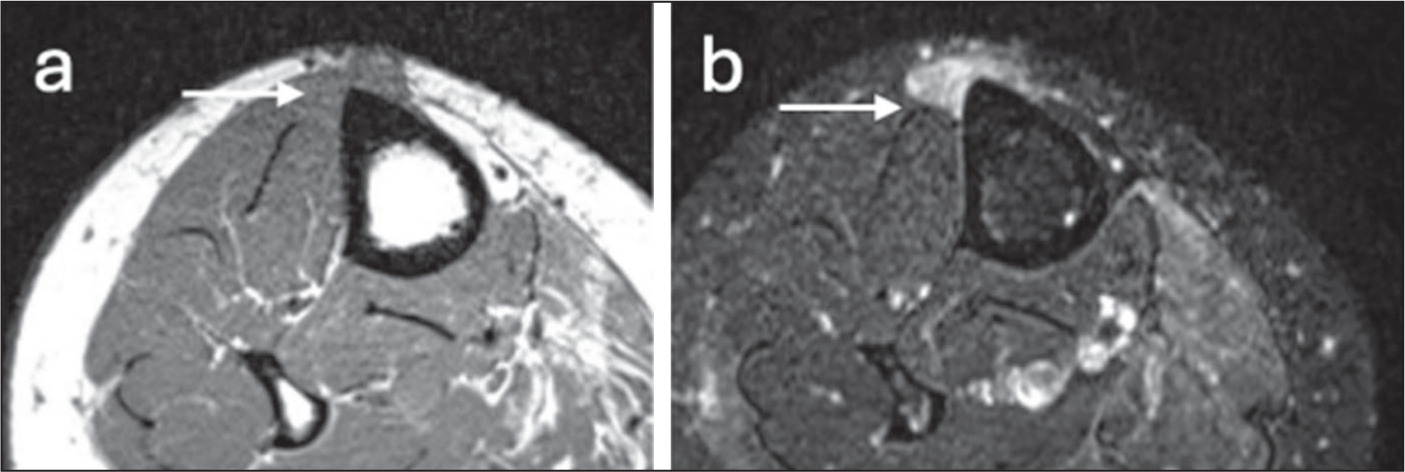
Axial T1-weighted (a) and STIR (b) images demonstrating a myopericytoma closely related to the tibialis anterior muscle (arrow)
Axial T1-weighted (a), STIR (b) and T1 fat-saturated post-contrast (c) images demonstrating a myopericytoma in the subcutaneous tissue, demonstrating peripheral contrast enhancement (arrow)
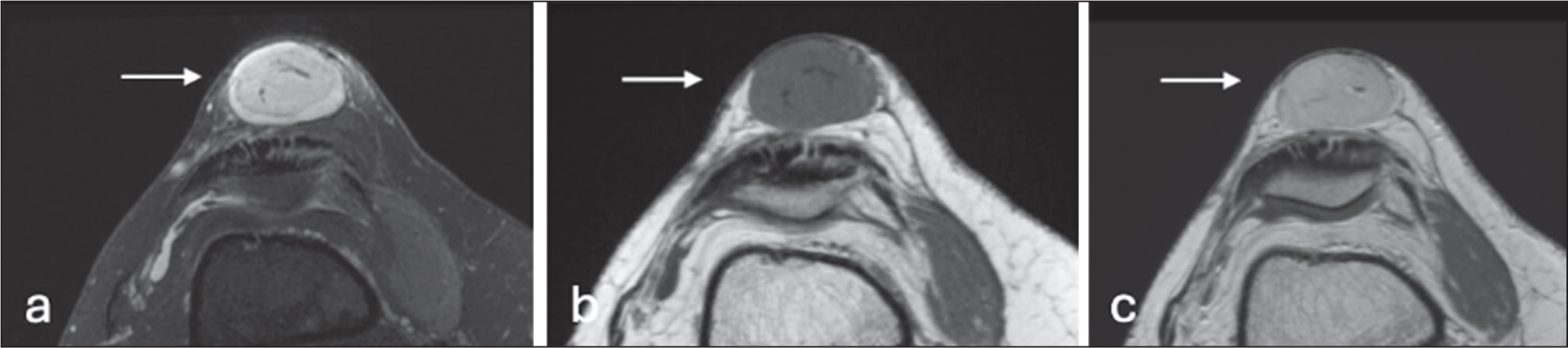
Contrast-enhanced imaging was available in eight cases, demonstrating heterogeneous enhancement in three cases, homogeneous enhancement in four cases and peripheral enhancement in one case. The corresponding mean maximum diameters were 3.3 cm, 2.7 cm and 1.9 cm, respectively [Figures 5–7].
Axial T2 fat-saturated (a), T1-weighted (b) and T2-weighted (c) images demonstrating a myopericytoma in the subcutaneous tissue (arrow)
Short-axis ultrasound (a), colour Doppler (b), axial T1-weighted (c), T1 fat-suppressed pre-contrast (d) and post-contrast (e) images demonstrating a myopericytoma in the subcutaneous tissue (arrow)

Functional imaging was performed in four cases. None of these lesions demonstrated a significant signal drop on chemical shift imaging or diffusion restriction on DWI [Figures 8–10].
Axial T1-weighted (a), STIR (b), DWI (c) and apparent diffusion coefficient (ADC) (d) images demonstrating a myopericytoma in the trapezius muscle (arrow), not showing restricted diffusion

Axial STIR (a), T1-weighted (b), DWI (c) and apparent diffusion coefficient (ADC) (d) images demonstrating a myopericytoma (arrow) located between the flexor tendons, without significant diffusion restriction

Coronal T1-weighted (a), STIR (b), in-phase (c) and out-of-phase (d) images demonstrating a myopericytoma (arrow) located between the flexor tendons of the hand

Ultrasound evaluation was available in 26 cases. On sonographic assessment, the lesions were well-defined and predominantly hypoechoic, with a few cases demonstrating heterogeneous echogenicity. Colour Doppler imaging revealed increased vascularity in all cases.
Discussion
Before this study, scattered case reports and small case series have been used to describe imaging characteristics of myopericytoma. This study not only reviews imaging findings in 51 cases of myopericytoma but also reviews the findings of existing literature to delineate reliable trends in myopericytoma appearances.
Our study highlights that a lesion showing a low signal on T2-weighting or a homogeneous high signal on T1-weighting is unlikely to represent myopericytoma with a good degree of confidence, as none of the cases in our cohort exhibited such signal characteristics. Although in isolation this is not dissimilar to many other soft tissue lesions, including related pediatric myofibroma, and solitary fibrous tumour (encompassing tumours formerly termed haemangiopericytomas), their diagnostic value increases when interpreted along with clinical features and additional imaging characteristics reflecting internal architecture.
This series also builds upon T1-weighted and T2-weighted assessment by further examining DWI, opposed-phase imaging and contrast enhancement, providing a comprehensive assessment of myopericytoma. The results show that abnormal diffusion restriction and evidence of chemical shift are also unlikely in myopericytoma and if present, can reliably exclude this entity from the differential.
Our study has also helped to clarify the role of gadolinium-enhanced MR imaging, which has previously been uncertain. The findings show that internal enhancement is the most common pattern, with a slight increase in likelihood of heterogeneous internal enhancement with increasing size, possibly representing the growth of a vascular lesion exceeding its blood supply and thus resulting in pockets of necrosis.
As with chemical shift imaging, the demonstrated utility of contrast-enhanced imaging supports the inclusion of these additional sequences as part of the MRI protocol in suspected cases.
These findings help to differentiate myopericytoma from a range of other soft tissue tumours. But, as with other lesions sharing a spectrum, imaging differentiation of myopericytoma from its closely related entities (e.g., myofibroma) can be difficult. However, the literature outlines that clinical features can aid in diagnosis, as unlike myofibroma, myopericytoma is rare in children, relatively rare in the head and neck and often presents as a solitary lesion. This is supported by our study, which shows that the majority of myopericytoma cases occurred in the appendicular skeleton, particularly the lower limbs and that all lesions were solitary. Imaging is less definitive, with both showing similar T1- and T2-weighted signal appearances, but contrast enhancement can be helpful as it is generally heterogeneous in myofibroma, whereas myopericytoma typically shows peripheral or homogeneous enhancement. Nevertheless, it is reasonable to expect that many of these will proceed to histopathological analysis, with immunohistochemistry potentially contributing to clarity on the diagnosis.
Conclusion
This study represents the largest case series to date evaluating the radiological appearances of myopericytoma. The descriptions and images presented provide insight into the imaging characteristics of myopericytoma and may facilitate optimising imaging protocols, as well as improving the reporting of suspected lesions, giving radiologists greater confidence in narrowing the differential diagnosis.
Footnotes
Consent to participate
Not applicable.
Consent for publication
Yes.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Local ethical committee approval was obtained and research was carried out in n accordance with the Declaration of Helsinki.
Credit author statement
Saavi Reddy Pellakuru, Scott Evans, Rajesh Botchu: Conception and design or acquisition of data or analysis and interpretation of data.
Saavi Reddy Pellakuru, Hasaam Uldin, Rajesh Botchu: Design or acquisition of data or analysis and interpretation of data.
Saavi Reddy Pellakuru, Jonathan Gibson, Hasaam Uldin, Vaiyapuri Sumathi, Scott Evans, Rajesh Botchu: Drafting the article or revising it critically for important intellectual content.
Saavi Reddy Pellakuru, Jonathan Gibson, Hasaam Uldin, Vaiyapuri Sumathi, Scott Evans, Rajesh Botchu: Final approval of the version to be published.
Data availability statement
Data is available to share on request.
Use of artificial intelligence
No artificial intelligence was used.