
Abstract
Gallbladder adenomyomatosis is a benign non-inflammatory condition of the gallbladder characterised by hyperplastic changes of the mucosa and thickening of the muscular wall. It represents one of the three morphologic types of adenomyomatosis—fundal (localised), segmental and diffuse—with the segmental type being the second most common type. It can present as a symptomatic gallbladder disease since it is often associated with the formation of gallstones due to bile obstruction.
This case report views a 59-year-old male patient with a history of recurrent vomiting for the past two months, which is associated with intermittent pain in the upper quadrant of the abdomen and a significant reduction in appetite, thus requiring surgical treatment. A USG, along with magnetic resonance cholangiopancreatography (MRCP) analysis, confirmed the clinical diagnosis along with gallbladder stones. This case elaborates on the radiological, clinical, and surgical range of annular adenomyomatosis of the gallbladder and signifies the need for timely surgical intervention in a case of recurrent vomiting, which helped in improving patient outcomes.
Introduction
Gallbladder adenomyomatosis is a benign, acquired pathological condition affecting the gallbladder, typically characterised by a favourable prognosis. The majority of such cases are discovered incidentally, either through imaging or during the histopathological assessment of resected gallbladders.[1] The term adenomyomatosis was used by Jutras and associates for the gallbladder disease characterised by proliferation of mucosal epithelium and the formation of pockets in the thickened hypertrophic muscle layer. These pockets are called Aschoff-Rokitansky sinuses.[2] While most patients with adenomyomatosis are asymptomatic, the most commonly reported symptom is nonspecific pain localised to the right upper quadrant and epigastrium. The presence of gallstones is a very common associated complaint seen in almost 50% of patients.[3] The potential of gallbladder annular adenomyomatosis to mimic malignant lesions on radiological imaging is high, thus posing a diagnostic challenge.[4]
Based on the extent and distribution of these changes, GA is classified into three different types: fundal or localised, segmental or annular, and diffuse type. The localised type is the most common type and is confined to the gallbladder fundus, presenting as a focal thickening or nodular lesion that might mimic a localised mass on imaging.[5] The segmental or annular type involves circumferential mural thickening, typically at the middle of the gallbladder, producing an annular stricture that may divide the lumen into separate compartments, thus giving an hourglass appearance. This form is often associated with the formation of gallstones due to bile obstruction. The diffuse type represents uniform involvement of the entire gallbladder wall, characterised by generalised mural thickening and intramural cystic spaces, giving the gallbladder a ‘pearl necklace’ appearance on MRI.[6] Although adenomyomatosis is considered benign, the annular and diffuse types may occasionally mimic gallbladder carcinoma both radiologically and clinically; careful differentiation through advanced imaging modalities and histopathological evaluation becomes a necessity to avoid wrong treatment plans and unwanted surgical interventions. The localised type is described as the most common in the elderly, whereas in children, the diffuse type was the most encountered type.[7]
This article discusses a case of annular or segmental gallbladder adenomyomatosis that presented with cholelithiasis, characterised by vomiting, upper quadrant pain, and reduced appetite. MRCP confirmed the presence of annular gallbladder adenomyomatosis.
Case Presentation
A 59-year-old male patient presented with complaints of repetitive vomiting for the past two months, associated with intermittent pain in the upper quadrant of the abdomen. The vomiting was non-bilious, non-bloody, and usually occurred after meals. The abdominal pain was dull in nature, localised to the epigastric and right upper quadrant regions, unaccompanied by radiation, and was not related to food intake. The patient also reported early satiety and progressive loss of appetite. There was no history of hematemesis, melena or any altered bowel habits. His past medical history is pronounced for diabetes mellitus and hypertension, both of which have been under regular medication and follow-up. There was no significant family history or history of alcohol or tobacco use.
On examination, the patient was not icteric, and the abdomen was soft with mild tenderness in the right hypochondrium, no palpable mass or organomegaly [Figure 1].
MRCP image showing the biliary tree and common bile duct
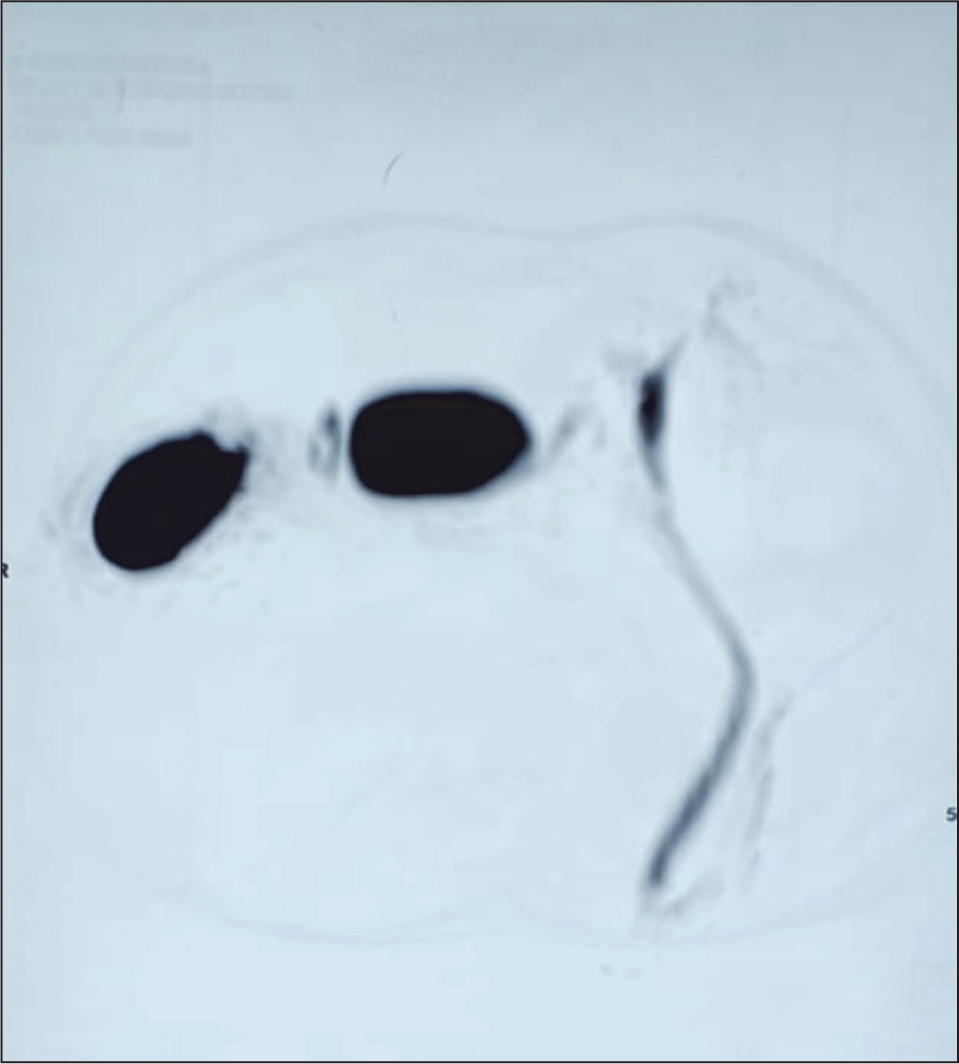
Ultrasound showed numerous gallbladder calculi (stones) measuring around 8–10 mm with sludge. magnetic resonance cholangiopancreatography (MRCP) findings showed annular narrowing at midbody with an hourglass configuration, with numerous tiny (2–3 mm) T2 hypointense filling defects seen in the body seen suggestive of adenomyomatosis with gallbladder stones [Figure 2].
MRCP reconstruction image demonstrating gallbladder (GB), common hepatic duct (CHD), common bile duct (CBD), and pancreatic duct (PD)

The patient underwent upper gastrointestinal endoscopy in view of repeated vomiting, which was not significant.
After a thorough preanesthetic workup, the patient underwent laparoscopic cholecystectomy under general anaesthesia. The procedure was completed without complications, and the gallbladder was successfully removed. The gallbladder opened after removal, which showed segmental adenomyomatosis with black pigment stones [Figure 3]. The postoperative course was uneventful, and the patient had complete resolution of symptoms, confirming the effectiveness of the surgical intervention.
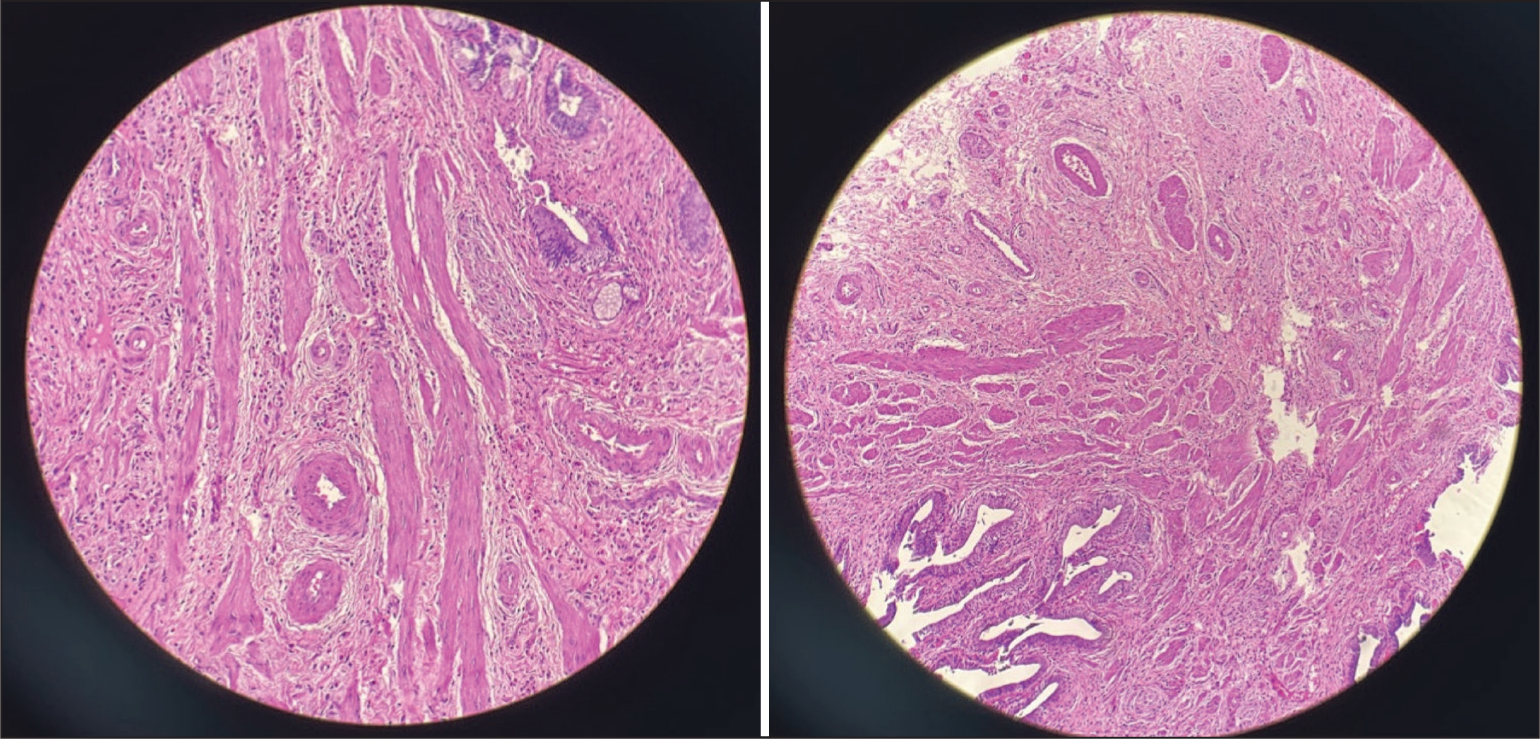
Gallbladder wall shows characteristic mucosal proliferation with Rokitansky-Aschoff sinuses and muscular hypertrophy, consistent with adenomyomatosis without dysplasia or malignancy identified
Discussion
Diffuse or localised thickening of the gallbladder wall can be seen in gallbladder adenomyomatosis, which is a benign, non-neoplastic condition identified by multiplication of the gallbladder mucosal epithelium, accompanied by hypertrophy of the muscularis propria. Rokitansky-Aschoff sinuses (RAS) are intramural diverticula formed due to the proliferative process in mucosal invaginations, which extend into or through the muscular layer.[5] On ultrasound, these can be seen as tiny cystic spaces within the thickened wall encompassing bile, cholesterol crystals, or minute calculi. Fundal, segmental and diffuse are three morphological subtypes of gallbladder adenomyomatosis based on their anatomic distribution. The most common type, the fundal type, is identified by focal thickening limited to the fundus of the gallbladder.[8] The mid-portion of the gallbladder is affected in the segmental type, which reveals a circumferential or annular constriction dividing the lumen into two communicating compartments. On the contrary, the complete gallbladder is involved in the diffuse type, leading to generalised mural thickening and an irregular external surface.[9]
Several cases of adenomyomatosis have been diagnosed with the help of ultrasound and peroral cholecystography in accordance with published literature. Peroral cholecystography usually shows multiple intramural collections or contrast-filled sinuses in relation to the Rokitasky-Aschoff sinuses in diffuse forms of the disease, thereby producing a spiculated or ‘thorny’ appearance of the gallbladder wall. Contrast filling defects can be seen in particular regions, like the fundus or body, depending on the affected site in localised or segmental types.[10] Clinically, intermittent pain in the right upper quadrant mimicking discomfort associated with gallstones or chronic cholecystitis can usually be seen in gallbladder adenomyomatosis. The pain is generally mild to moderate in severity, tends to occur intermittently and usually subsides on its own without the need for treatment. In numerous cases, these clinical features are believed to arise from associated gallstones or inflammatory processes rather than from the adenomyomatosis itself, which is frequently associated incidentally during injury or surgery.[11]
Since fewer than 10 cases have been identified in infants within one year of age, the condition is not likely to represent a congenital anomaly. Gallbladder adenomyomatosis is rather regarded as a degenerative or acquired disease. Although there has been a slight but noticeable correlation with gallbladder carcinoma, it is typically thought of as a non-premalignant process. ADM can mimic cancer both clinically and radiologically, making diagnosis difficult. Compared to focal or diffuse forms, the segmental type has been more commonly associated with coexisting carcinoma, even though the majority of cases are found by accident and remain asymptomatic. In order to rule out or keep an eye out for possible malignant transformation, careful radiologic evaluation and suitable clinical follow-up are advised, especially in segmental adenomyomatosis. A contributing factor is the intraluminal pressure caused probably due to neurogenic dysfunction of gallbladder motility. Another significant factor involves an anomalous pancreaticobiliary ductal junction, allowing chronic reflux of pancreatic secretions into the gallbladder, leading to mucosal proliferation and wall thickening. Though a direct causal relationship has not been determined, it is observed that gallstones are associated in over 50% of all adenomyomatosis cases and in up to 90% of the segmental type.[12] Since the cholesterol crystals precipitate in the bile trapped in RAS (intramural diverticula lined by mucosal epithelium), Intraluminal cholesterol accumulation can be seen in adenomyomatosis.[13] Though administration of intravenous contrast material is required for proper CT evaluation of the gallbladder, bile sludge and calculi can be seen as high-attenuation intraluminal material at nonenhanced CT. Common nonspecific CT features of adenomyomatosis include abnormal gallbladder wall thickening and enhancement. The extent and location of gallbladder involvement in adenomyomatosis hyperplasia vary, resulting in heterogeneous imaging features that correspond to diffuse, segmental, or focal forms of adenomyomatosis.[5] Widespread gallbladder involvement is seen in diffuse or generalised adenomyomatosis. A distinctive hourglass configuration can be seen in segmental or annular adenomyomatosis, as it seems to have a limited circumferential wall involvement with luminal narrowing, particularly within the gallbladder body.[8]
The management strategy principally depends on the patient’s clinical symptoms and associated symptoms if gallbladder adenomyomatosis is properly diagnosed preoperatively using advanced imaging modalities. Active surgical management is generally not required in cases where the condition is detected incidentally and when the patient remains asymptomatic. Rather, a conservative ‘wait-and-watch’ approach is preferred to avoid unnecessary surgical interventions. This strategy can be suitably followed only if the imaging studies, such as ultrasound, CT, or MRCP, significantly rule out the probability of gallbladder carcinoma or any other serious pathology. If diagnostic ambiguity exists or malignancy is suspected, a cholecystectomy becomes an appropriate and cautious measure to ensure the patient’s safety and to arrive at a definitive diagnosis.[4]
Patients treated conservatively should undergo periodic follow-up to check for any alterations in the gallbladder wall, such as progressive thickening, newly developed irregularities, or the onset of symptoms such as right upper quadrant pain or dyspepsia. Routine ultrasonography continues to be the desired imaging modality for follow-ups as it is non-invasive, cost-effective and readily available. In order to balance patient safety along with the avoidance of unwarranted procedures, it is significantly advised to take follow-up scans every three to six months to detect any early indicators of disease progression, thereby allowing timely surgical interventions.[14]
Conclusion
To conclude, gallbladder adenomyomatosis is a benign, acquired pathological condition affecting the gallbladder. This case highlights the importance of maintaining a high index of suspicion for gallbladder pathology when a patient presents with recurrent vomiting and underscores the role of surgery in both diagnosis and definitive management.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
NA.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Credit author statement
Aadithya Siddarth S: Conceptualised the work, collected relevant information, and prepared the manuscript draft. Responsible for writing, revising, and finalising the article.
Dr Asfar Ahamed Nawabjan: Provided the clinical case, supervised the work, and offered expert guidance throughout the preparation of the manuscript.
Dr Lalith Kumar: Contributed to supervision and provided valuable guidance and critical review to enhance the quality and accuracy of the manuscript.
Data availability statement
NA.
Use of artificial intelligence
NA.