
Abstract
Background:
India carries the highest global burden of tuberculosis (TB), with children contributing approximately 6%-7% of cases reported under the National Tuberculosis Elimination Programme (NTEP). Paediatric TB poses unique diagnostic and therapeutic challenges due to its paucibacillary nature, difficulty in specimen collection and increasing prevalence of drug-resistant TB. Recent advances in diagnostics, therapeutics and preventive strategies have transformed the management of TB in children.
Methods:
This narrative review summarises recent evidence, World Health Organisation (WHO) recommendations and updated NTEP guidelines on the diagnosis, treatment and prevention of TB in children. Literature was identified from WHO reports, national programme guidelines and recent peer-reviewed studies focusing on molecular diagnostics, drug-resistant TB regimens and TB preventive treatment (TPT).
Results:
Rapid molecular diagnostics such as Xpert MTB/RIF, Truenat assays, Xpert MTB/XDR and line probe assays allow early detection of TB and drug resistance. Use of less invasive specimens, including stool and nasopharyngeal aspirates, is upcoming. The C-Tb skin test is a newer diagnostic tool for the detection of latent TB with greater specificity than the tuberculin skin test (TST). Treatment outcomes have improved with newer drugs such as bedaquiline and delamanid, and short-duration all-oral regimens for drug-resistant TB. Shorter rifamycin-based TPT regimens have enhanced adherence and completion rates.
Conclusion:
Recent advances in diagnostics, treatment and prevention have significantly improved the management of paediatric TB. Integration of rapid molecular testing, child-friendly all-oral regimens and shorter preventive therapies can improve outcomes and support India’s efforts towards TB elimination.
Introduction
India has the largest global burden of tuberculosis (TB), accounting for approximately 25% of total TB incidence worldwide.[1] According to the WHO reports of 2020, 1.1 million children and young adolescents (aged below 15 years) and 0.5 million older adolescents (15–19 years of age) are diagnosed with TB annually.[2] Children (0–14 years of age) consistently account for 6%-7% of all the TB patients treated under the National Tuberculosis Elimination Programme (NTEP), with an estimated 3.42 lakh new cases of paediatric TB every year in India.[3] The increasing burden of drug-resistant TB is a major challenge for the elimination of TB, with India contributing approximately 32% of the reported cases.[1] Although the rate of successfully treated multidrug-resistant tuberculosis (MDR-TB) patients in India has increased from 49% in 2017 to 75% in patients in the 2021, TB elimination still seems like a distant goal.[4] Recent advances in the diagnosis and treatment of TB have revolutionised disease management and represent an important step towards the goal of TB elimination.
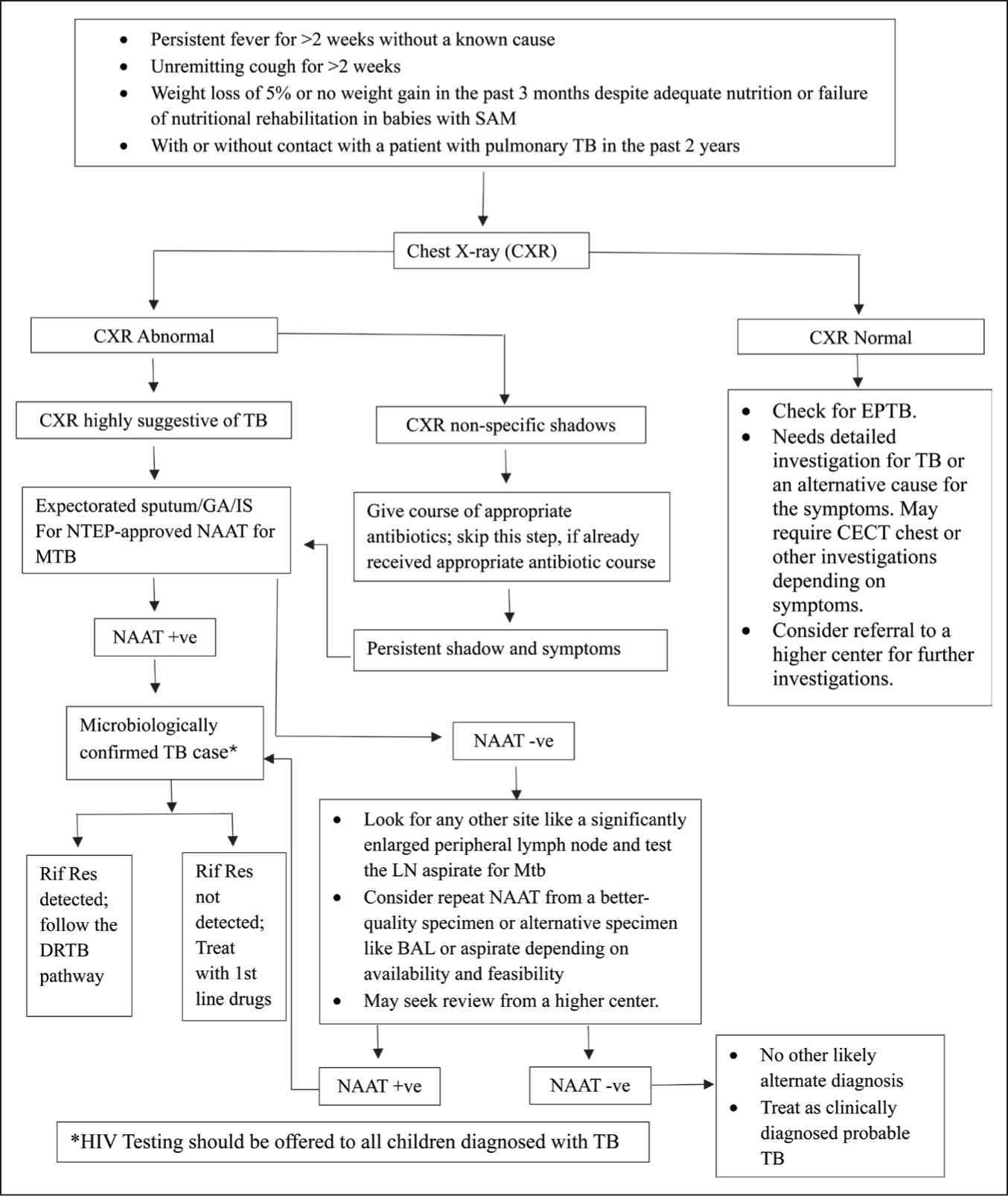
A child is suspected to have TB (presumptive paediatric TB) based on any of the following symptoms: persistent fever, unremitting cough for more than 2 weeks, >5% weight loss in the past 3 months or inadequate weight gain in the past 3 months, with no other apparent cause, with or without a history of contact with an infectious TB patient. All such cases should be investigated for TB, and the initial specific investigation recommended is a chest X-ray. This is a significant change from the earlier guidelines, where a sputum smear examination was the initial recommended investigation.
The initial chest X-ray is considered to be highly suggestive of TB if it shows miliary shadows or intrathoracic lymphadenopathy (hilar or mediastinal) or chronic fibro-cavitary shadows. Such a child is further subjected to nucleic acid amplification test (NAAT) based tests on sputum/induced sputum/gastric aspirate samples for the detection of Mycobacterium tuberculosis (MTB).
What Is New in Diagnostics?
The updated approach in NTEP involves universal drug-susceptibility testing (UDST) for all TB patients, with a particular emphasis on rifampicin resistance using NTEP-approved rapid NAAT on appropriate clinical specimens, such as sputum, induced sputum, gastric aspirate or lavage, lymph node aspirate and other body fluids. NAATs are real-time PCR-based diagnostic tests. There are various NAAT-based tests available; the NTEP-approved rapid NAAT include Xpert MTB/RIF, Truenat MTB or MTB Plus and Truenat MTB-RIF Dx.
Molecular Methods Used for Testing of Drug Resistance
NAAT
Xpert MTB/RIF: It is a cartridge-based nested real-time PCR test for simultaneous detection of MTB and its resistance to rifampicin. The sample processing time is around 2 h. It has high sensitivity with a lower limit of detection of 130 CFU/ml. Xpert ultra: It has higher sensitivity to detect TB (16 CFU/ml) and more reliable rifampicin resistance detection. It is particularly useful in sputum smear-negative TB, HIV with TB and extrapulmonary TB. In a systematic review, the overall sensitivity of Xpert Ultra was higher than Xpert MTB/RIF (73% vs. 66%), but the specificity was borderline lower (95% vs. 99%).[5] The WHO has recommended it as the initial diagnostic test due to superior performance in smear-negative cases, but it has not yet been included in the NTEP.[6] Truenat MTB or MTB Plus and Truenat MTB-RIF Dx: They are chip-based, micro real-time PCR-based tests to detect MTBb and sequential rifampicin resistance, respectively. The sample processing time is around 1 h. Studies have shown that the performance of both GeneXpert MTB/RIF and Truenat MTB-Rif Dx is comparable.[7] Xpert MTB/XDR: It is a nested PCR-based test which detects MTB and resistance to isoniazid (INH), fluoroquinolones (FQ), ethionamide (ETH) and second-line injectable drugs (amikacin, kanamycin and capreomycin) in a single test. It is particularly useful for excluding fluoroquinolone resistance before initiating the bedaquiline-based short oral MDR/RR-TB treatment regimen.
Table 1 compares and contrasts the various NAAT-based molecular tests for the diagnosis of TB. Molecular tests cannot be used for treatment monitoring, unlike smear microscopy, as they cannot distinguish between viable and non-viable organisms. The major advantage of these tests is that they provide results within a few hours, have higher sensitivity and specificity than the smear for acid-fast bacilli (AFB) and can also detect rifampicin resistance. Despite these advantages, these tests have moderate sensitivity but high specificity and therefore, a negative test does not rule out TB disease.
NAAT-based molecular tests for diagnosis of tuberculosis
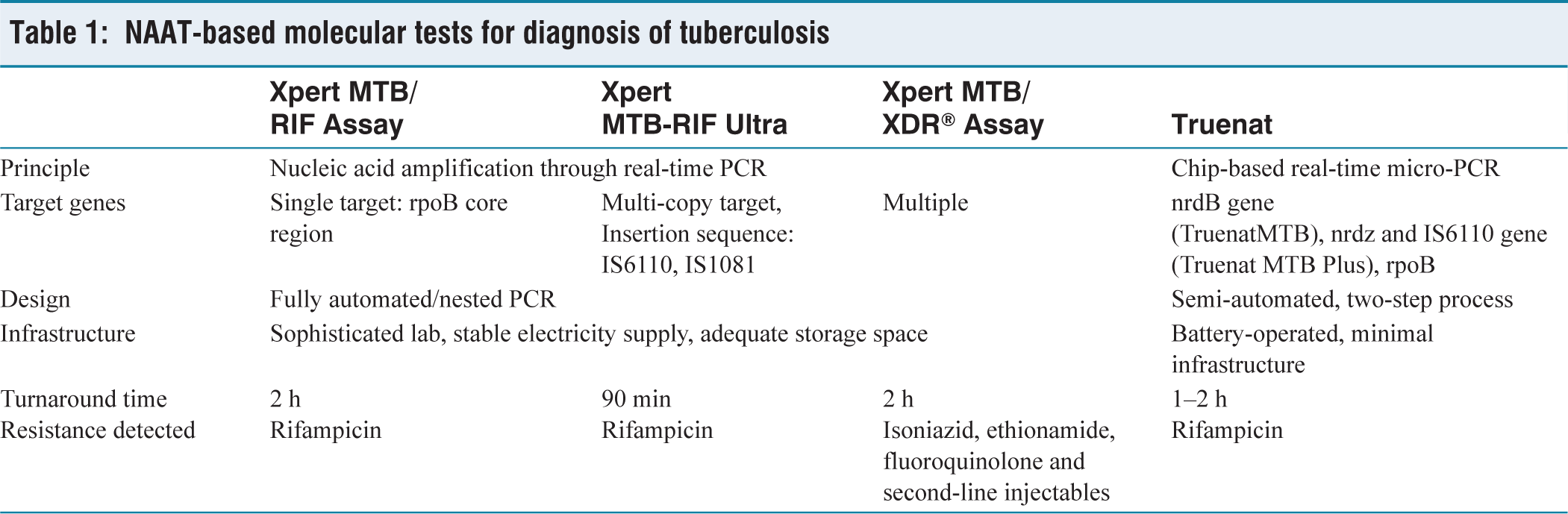
The sensitivity of the tests also depends upon the clinical specimen; the respiratory specimens, lymph node aspirate and CSF perform better than pleural or ascitic fluid, which have very poor sensitivity. It is difficult to collect a sputum specimen for NAAT in children. The gastric aspirate collection requires some training, and improper collection technique results in a poor yield of bacilli. Therefore, NAAT testing on stool specimens has been studied, and stool Xpert has shown a pooled sensitivity of 0.60 (0.48–0.71) and a pooled specificity of >0.99 to detect TB. However, the major concern for this test is the stool processing method, and the reference standard has not been established.[8] Similarly, nasopharyngeal aspirates have shown a similar yield to more invasive gastric aspirate samples.[9] Stool and nasopharyngeal aspirates are now being recommended as the alternative, less invasive specimens for NAAT in suspected pulmonary TB cases by the WHO, but have not yet been included in the NTEP.[2,4]
Line probe assay (LPA): It is a rapid molecular test based on PCR amplification and reverse hybridisation to detect MTB and its resistance. The first-line LPA detects MTB and resistance to rifampicin and isoniazid. The second-line LPA is used to identify resistance to fluoroquinolones and second-line injectable drugs. This is the only WHO and NTEP-recommended rapid test for detecting additional drug resistance in patients with MDR-TB and XDR-TB. It can only be performed on smear-positive sputum samples or culture isolates (like MGIT) for genotypic drug-susceptibility testing (DST). It has a low sensitivity, with a limit of detection of 10,000 CFU/ml. The sample processing time is around 72 h.
Lateral flow urine lipoarabinomannan (LF-LAM) assay: It is a rapid, point-of-care test for the diagnosis of TB in HIV-positive adults and children. It detects LAM, a cell wall component of MTB, which is excreted in urine in active TB. WHO recommends the use of the LF-LAM assay in inpatient HIV-positive patients with signs and symptoms of TB, critically ill patients, advanced HIV disease or CD4 cell count less than 200 cells/mm3 and outpatient HIV-positive patients with signs and symptoms of TB, critically ill patients or CD4 cell count less than 100 cells/mm3.
Whole genome sequencing: The drug resistance in MTB is mainly conferred through point mutations, and hence targeted sequencing seems promising for rapid diagnosis of DR-TB. Targeted sequencing can be performed by pyrosequencing, Sanger sequencing or next-generation sequencing. Currently, these tests are limited to research laboratories.
Growth-based Phenotypic DST
Mycobacteria Growth Indicator Tube (MGIT)
This is a fluorescence-based technique with a shorter turnaround time compared to solid LJ media.[10] It is the preferred method for testing drug sensitivity under NTEP.[2] It can test both pulmonary and extrapulmonary samples for first as well as second-line antitubercular drug sensitivity.
Immunodiagnostic Tests for Diagnosis of Latent TB
TST/Mantoux test is an age-old intradermal test using 0.1 ml tuberculin 2TU PPD RT23. It is a low-cost test and easy to use. However, the utility of this test has decreased since the original lot of RT23 PPD is not available now.
Interferon gamma (IFN-γ) release assay (IGRA) is an in vitro measure of MTB hypersensitivity, and the information provided is the same as TST. TB Quantiferon GoldTM and TB SpotTM are the currently approved tests by the WHO. Unlike the TST, the IGRA test does not cross-react with BCG vaccination but needs efficient transportation of the sample to the lab and is expensive. Both IGRA and TST had similar but lower performance in countries with high TB incidence.[11]
C-Tb (or Cy-Tb) is a novel skin test for the detection of TB infection developed by Statens Serum Institute, Copenhagen. It uses ESAT-6 and CFP-10 antigens specific for M. tb, similar to IGRA. It has IGRA-like specificity with the ease of a skin test. The results are read 48–72 h after intradermal injection with a universal cut-off of 5 mm for TB infection. It is unaffected by BCG vaccination. It is recommended in the NTEP programme guidelines, but has not been adopted yet, due to commercial unavailability and approval.
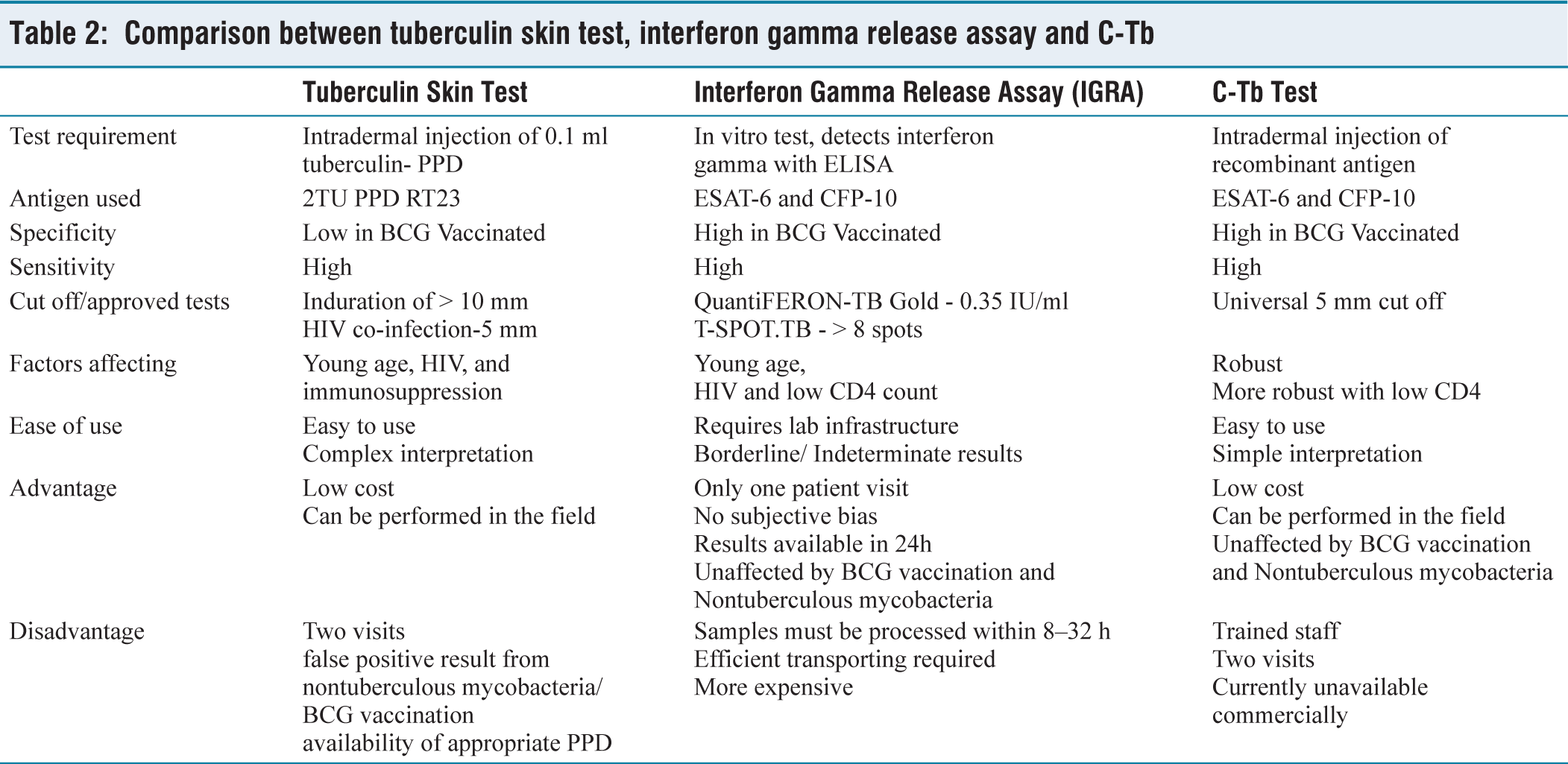
The sensitivities of C-Tb, TST and QuantiFERON-TB Gold test were similar (72% vs. 75% vs. 73%; P > .5), with similar positivity rates in HIV-infected participants with active TB. Overall, C-Tb and the TST showed a similar safety profile.[12] However, all these tests indicate current or previous infection with MTB but do not indicate TB disease. Table 2 compares and contrasts the various immunodiagnostic tests used for the diagnosis of latent TB.
Comparison between tuberculin skin test, interferon gamma release assay and C-Tb
The algorithm for the diagnosis of pulmonary TB in children is depicted in Figure 1.
What Is New in Treatment?
Treatment of Drug-sensitive TB
The treatment for drug-sensitive/rifampicin-sensitive TB includes daily therapy of antitubercular drugs; four drugs, isoniazid, rifampicin, pyrazinamide and ethambutol (HRZE) given for 2 months in the initial C (IP) and three medications-isoniazid, rifampicin and ethambutol (HRE) given for 4 months in the continuation phase (CP) (2HRZE+ 4HRE). The CP is extended for 10 months in neurological and spinal TB (2HRZE+10HRE). No extension of IP beyond 2 months is recommended. Ethambutol plays an important role in preventing the emergence and amplification of drug resistance, particularly when the background prevalence of isoniazid resistance is high, thereby strengthening the effectiveness of both the intensive and continuation phases of TB treatment. Hence, it is included in the continuation phase in our country. The drugs are administered as fixed drug combinations with dispersible paediatric formulations available under NTEP and given as per the weight bands. Adjunctive therapy with pyridoxine (10 mg) is recommended for all patients. The dosages of individual drugs are given in Table 3.
Individual drug dosages for drug-sensitive tuberculosis

New Short Regimens for Drug-sensitive TB in Children
Paediatric 4-month [2HRZ(E)/2HR] Regimen
In children and adolescents between 3 months and 16 years of age with non-severe TB (without suspicion or evidence of MDR/RR-TB), a 4-month treatment regimen [2HRZ(E)/2HR] can be used. It consists of standard-dose 2 months of HRZ, with or without ethambutol, followed by 2 months of H and R. Recent WHO guidelines also recommend the use of this regimen due to better compliance and non-inferiority to the standard 6-month regimen as observed in the SHINE trial (Shorter Treatment for Minimal Tuberculosis in Children).[13] However, the regimen has not been approved by NTEP due to the difficulty in defining patients with non-severe paediatric TB.[4]
Shorter Intensive Regimen (6 Month Daily Isoniazid, Rifampicin, Pyrazinamide and Ethionamide) for Tubercular Meningitis
A 6-month shorter intensive regimen consisting of daily isoniazid, rifampicin, pyrazinamide and ethionamide (6HRZEto) may be used in children who are diagnosed with TB meningitis, either microbiologically confirmed or clinically diagnosed without suspicion or evidence of drug resistance, as an alternative to the longer 12-month regimen (2HRZE/10HR). This regimen is a monophasic regimen and uses higher doses of isoniazid, rifampicin, pyrazinamide and ethionamide compared to standard pulmonary TB treatment. Ethionamide has better blood-brain barrier penetration than ethambutol. WHO recommends conditional use of this regimen as studies have found higher treatment success and lower mortality, but higher neurological sequelae.[14] This regimen is not included in NTEP yet.
New Medications
Bedaquiline (Bdq)
Bedaquiline is a diarylquinoline compound with a unique mechanism of action. It inhibits mycobacterial ATP synthase and is effective against both actively replicating and dormant MTB. Bdq has been fully integrated into India’s NTEP for the management of drug-resistant TB. While WHO recommends its use in children of all ages, NTEP generally recommends Bdq in children above 5 years and a weight of ≥15 kg, with individualised consideration for younger children. The major side effect of this drug is QTc prolongation (QTc >450 ms or >60 ms from baseline), which needs to be monitored at regular intervals.
Delamanid (Dlm)
Delamanid is a nitroimidazole derivative used in the treatment of MDR-TB. It inhibits the synthesis of methoxy- and ketomycolic acids, which are essential components of the mycobacterial cell wall, thereby suppressing bacterial growth. Dlm shows activity against both replicating and dormant MTB. Both WHO and NTEP recommendations have approved Dlm for all age groups. WHO classifies Dlm as a group C drug and recommends it for longer treatment regimens (18–20 months) on an individual basis when shorter regimens such as BPaLM/BPaL cannot be used.
New Regimens for Drug-resistant (DR)-TB in Children
Recent WHO and NTEP guidelines focus on shorter, all-oral regimens that eliminate the need for injections and improve compliance for management of DR-TB.
All-oral Bdq-containing Regimen (9–11 Months)
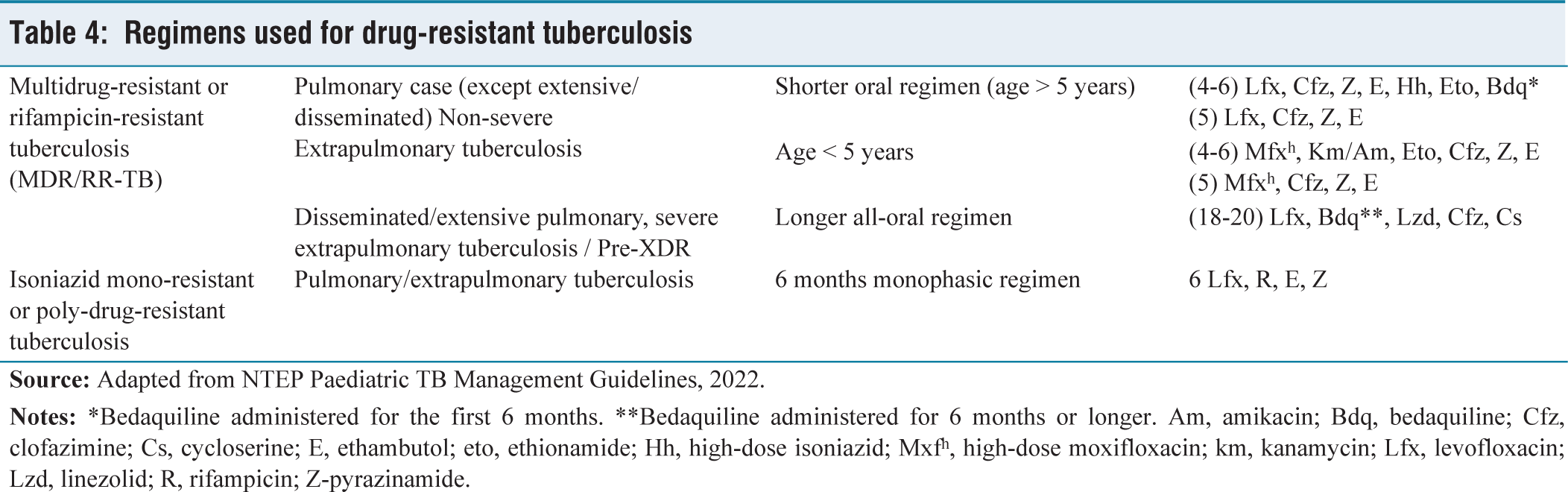
WHO recommends a shorter all-oral Bdq-containing regimen of 9–11 months duration in eligible patients with confirmed MDR/RR-TB across all age groups, provided that fluoroquinolone resistance has been excluded and they have not been exposed to second-line TB drugs included in this regimen for more than 1 month. It comprises a structured 4–6-month intensive phase including bedaquiline (6 months), levofloxacin/moxifloxacin, clofazimine, pyrazinamide, high-dose isoniazid and ethionamide (or linezolid), followed by a 5-month continuation phase consisting of levofloxacin/moxifloxacin, clofazimine, ethambutol and pyrazinamide. This aims to improve adherence, reducing toxicity and offer a more effective, shorter alternative to longer treatments, with good success rates.[2,12] NTEP recommends the shorter oral regimen as the first preferred treatment in children above 5 years of age with MDR/RR pulmonary TB (except extensive and disseminated TB) and non-severe extrapulmonary TB. Rapid tests to rule out fluoroquinolone resistance are required before starting this regimen. In children below 5 years of age, until Bdq is approved, it is replaced by injectable amikacin, and levofloxacin is replaced by high-dose moxifloxacin [Table 4].[15]
Longer Individualised Regimens (18–20 Months)
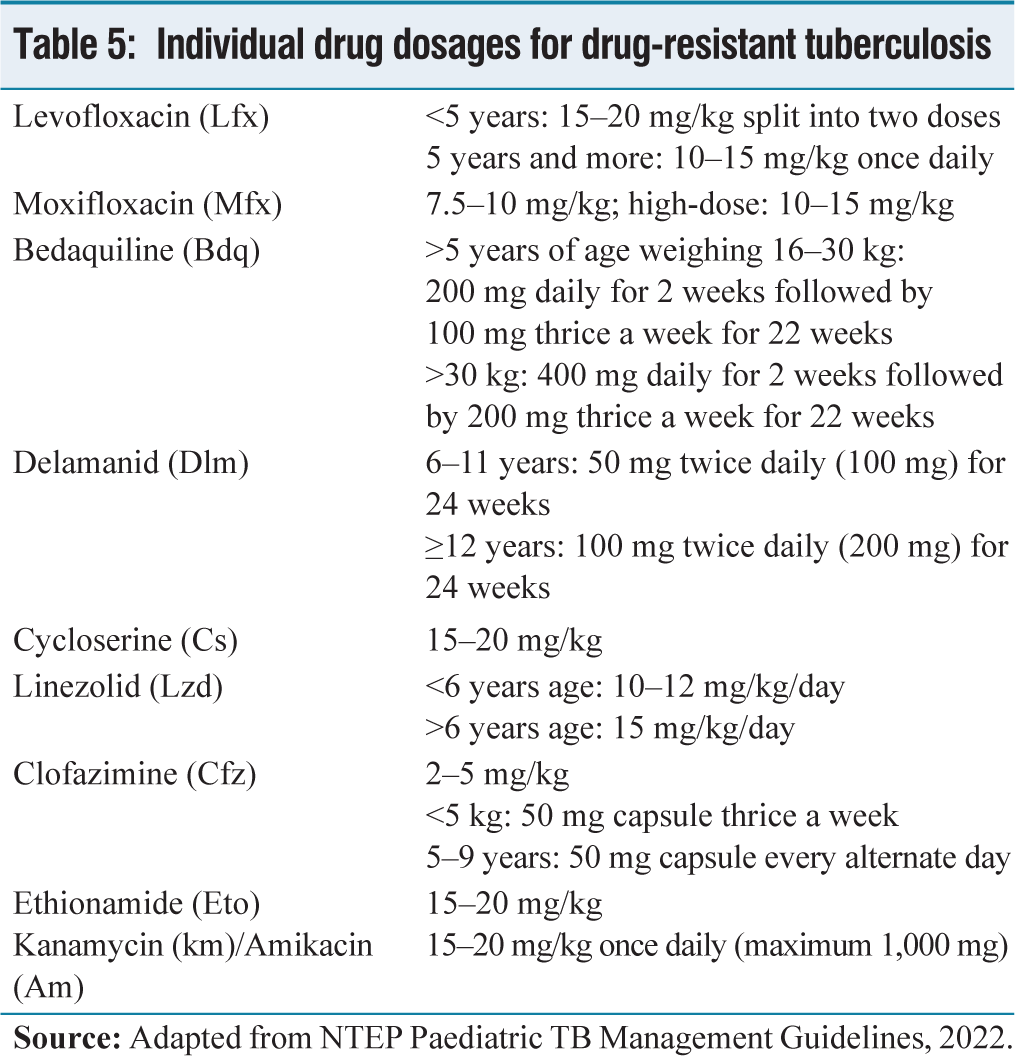
Both WHO and NTEP reserve longer regimens for complex drug-resistant cases across all age groups, including disseminated MDR-TB, extensive pulmonary disease, severe EPTB, Pre-XDR-TB, XDR-TB, or contraindications to shorter regimens. Treatment is individualised based on DST and may include Bdq and Dlm [Table 4]. The individual drug dosages for DR-TB is shown in Table 5.
Regimens used for drug-resistant tuberculosis
Individual drug dosages for drug-resistant tuberculosis
6-month BPaLM Regimen
Both WHO and NTEP recommend the 6-month BPaLM regimen as the preferred first-line treatment for patients aged ≥14 years with MDR/RR-TB and no fluoroquinolone resistance. It comprises Bdq, pretomanid, linezolid and moxifloxacin, all administered orally for 6 months.[2,15]
6-month BPaL Regimen
WHO recommends the use of Bdq, pretomanid and linezolid (BPaL) regimen in patients above 14 years of age having MDR-TB, along with fluoroquinolone resistance and who have either had no previous exposure to Bdq and linezolid or have been exposed for no more than 2 weeks.[2]
Regimen for Rifampicin-susceptible and Isoniazid-resistant TB
In patients with confirmed rifampicin-susceptible, isoniazid-resistant tuberculosis (Hr-TB), a 6-month regimen including rifampicin, ethambutol, pyrazinamide and levofloxacin is recommended.
What Is New in TPT?
Tuberculosis preventive treatment (TPT) is a key pillar of TB elimination strategies, aimed at preventing progression from TB infection to active disease in high-risk populations. Worldwide, the highest burden of TB infection is in India, and approximately 30% of the Indian population has the infection. Of these, 5%-10% are estimated to develop TB disease annually. Preventive treatment has been shown to reduce the overall risk for TB disease by 60% and up to 90% in people with HIV infection.
Eligibility for preventive therapy after ruling out active TB disease includes adults and children >12 months with HIV infection, infants <12 months with HIV in contact with a case of active TB and children less than 5 years of age who are household contacts of pulmonary TB patients. Children above 5 years and adolescent contacts of pulmonary TB patients and high-risk groups, such as patients on immunosuppressive treatment, are also eligible for preventive therapy if the test for TB infection is positive and active TB disease has been ruled out. Recent years have seen a shift from prolonged isoniazid monotherapy to shorter, rifamycin-based regimens, which have improved treatment completion and safety profiles.
6 Months Daily Isoniazid
This is the standard 6 months daily isoniazid (H) regimen given at the dose of 10 mg/kg/day (maximum 300 mg).
Weekly Rifapentine Plus Isoniazid for 3 Months (3HP)
Both WHO and NTEP recommend the 3HP regimen for the treatment of latent TB in individuals aged ≥2 years. The regimen consists of 12 once-weekly doses of rifapentine and isoniazid administered over 3 months. Compared with the conventional 6-month daily isoniazid (6H) regimen, 3HP has comparable efficacy, significantly higher treatment compliance and lower hepatotoxicity, making it a preferred option in eligible patients.[2,3]
Daily Isoniazid Plus Rifampicin for 3HR Regimen
WHO recommended a 3HR regimen that consists of daily isoniazid and rifampicin administered for 3 months. It is recommended for individuals of all age groups, including children and offers a shorter alternative to isoniazid monotherapy with better treatment completion. NTEP has included this regimen in the selected population.
Daily Rifampicin for 4R Regimen
WHO recommended the 4R regimen, which comprises daily rifampicin for 4 months. It is strongly recommended for HIV-negative individuals and remains an option for people living with HIV, provided there are no significant drug-drug interactions with antiretroviral therapy (ART). The regimen is associated with good tolerability and lower hepatotoxicity compared with prolonged isoniazid use.
Currently, only 6H and 3HP regimens are approved by NTEP.
TPT in DR-TB Contacts
Under NTEP guidelines, preventive therapy for contacts of drug-resistant TB is individualised based on the drug-susceptibility pattern of the index case. For household contacts of rifampicin-resistant, fluoroquinolone-sensitive TB patients, a 6-month regimen of daily levofloxacin (6Lfx) is recommended. A 4-month daily rifampicin (4R) regimen is recommended for contacts of TB patients who are isoniazid-resistant but rifampicin-sensitive. Exclusion of active TB and confirmation of drug-susceptibility of the source case are essential before starting the TPT in DR-TB contacts.[3]
In conclusion, paediatric TB is a major concern in India. The advancements in molecular diagnostics, upfront testing for rifampicin resistance, introduction of newer drugs, including Bdq and Dlm, along with simplified therapy for children for both drug-sensitive and drug-resistant TB have improved the diagnosis, adherence and reduced adverse effects for drugs. Shorter rifamycin-based preventive regimens are a major step towards the elimination of TB. These combined developments have the potential to improve treatment outcomes, reduce morbidity and support India’s efforts towards TB elimination.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Not applicable.
Credit author statement
SA: Conceptualised the manuscript, literature review, data synthesis, finalised manuscript.
AD: Literature review, data synthesis, prepared initial manuscript.
Both authors critically reviewed the manuscript and approved it for publication.
SA will act as a guarantor for this manuscript.
Data availability
Data sharing is not applicable to this article as no new data were created or analysed in this study.
Use of artificial intelligence
This manuscript was assisted by ChatGPT, an AI language model developed by OpenAI, which helped in refining the language.