
Abstract
Background and Aims:
Delayed gastric emptying (DGE) remains a common, costly source of morbidity after major upper gastrointestinal (GI) surgery, particularly after pancreaticoduodenectomy (PD) and oesophagectomy, despite advances in technique and enhanced recovery pathways.
Objective:
To synthesise contemporary evidence on definitions, diagnosis, risk stratification, prevention and treatment of postoperative DGE and to present a pragmatic, evidence-aligned prokinetic algorithm.
Methods:
Targeted narrative review of PubMed/PMC, focusing on consensus definitions, randomized controlled trial (RCT)s, meta-analyses and high-quality observational studies in PD, distal pancreatectomy (DP), gastrectomy and oesophagectomy.
Results:
The International Study Group of Pancreatic Surgery (ISGPS) criteria underpin DGE grading after pancreatic surgery; a 2020 international consensus exists for early DGE after oesophagectomy. Incidence after PD varies (≈10%–30%), influenced by technical and patient factors; risk increases with older age, preoperative biliary drainage, soft pancreas, postoperative pancreatic fistula (POPF) and high opioid exposure. Reconstruction route may affect DGE (inconclusively), while pylorus preservation versus resection shows no consistent benefit in RCTs. Enhanced recovery after surgery (ERAS) adherence reduces DGE-related sequelae. Prokinetics with the strongest footing are metoclopramide and domperidone; 5-HT4 agonists and ghrelin agonists (e.g., relamorelin) show promise in trials but are not yet standard postoperative care.
Conclusions:
Accurate phenotyping and structured care, excluding obstruction, optimise ERAS elements, treat contributors (POPF, infection, opioids) and deploy short, monitored prokinetic courses, can shorten DGE. We propose a stepwise algorithm integrating these elements.
Keywords
Introduction
Delayed gastric emptying (DGE) is a functional delay in gastric transit without mechanical obstruction, presenting with early satiety, nausea, vomiting and feeding intolerance after major upper gastrointestinal procedures. The International Study Group of Pancreatic Surgery (ISGPS) definition, still the lingua franca for pancreatic surgery, grades DGE severity by need for nasogastric (NG) decompression and failure to resume diet.[1] In contemporary series, clinically relevant (grade B/C) DGE after pancreaticoduodenectomy (PD) occurs in approximately 10%-30% of patients and contributes substantially to morbidity.[2–4] Beyond perioperative morbidity, DGE is consistently linked with longer hospital stay and higher early readmission rates after PD, with contemporary series indicating a measurable drag on early convalescence and patient-reported recovery trajectories.[2,4,5] After oesophagectomy, an international consensus proposed criteria for early DGE (delayed gastric conduit emptying [DGCE]) in 2020; subsequent comparative work highlights definitional sensitivity/specificity trade-offs.[6,7] These complications persist despite a decade of enhanced recovery after surgery (ERAS) implementation, prompting renewed focus on standardising diagnosis and rationalising therapy.[3,8,9]
The persistence of DGE despite refinements in operative technique and perioperative care highlights its complex, multifactorial pathophysiology. Patient factors such as age, comorbidity and nutritional status intersect with technical variables, including anastomotic configuration, pyloric preservation and conduit orientation to influence outcomes.[3–4,10] Moreover, the frequent coexistence of DGE with postoperative pancreatic fistula (POPF) or intra-abdominal infection complicates its diagnosis and management.[4,5] As such, DGE remains a key determinant of both resource utilisation and patient satisfaction and it continues to challenge surgeons striving to optimise short-term recovery while maintaining oncologic safety.
Methods
We searched PubMed/PMC using combinations of the terms ‘DGE’, ‘PD’, ‘oesophagectomy’, ‘gastrectomy’, ‘ERAS’, ‘prokinetic’ and specific agents such as metoclopramide, domperidone, erythromycin and relamorelin. Priority was given to consensus statements, randomised controlled trials, meta-analyses and large multicentre registries, while seminal pre-2015 publications were selectively included for definitional context. Reference snowballing was employed to capture additional pivotal studies. No quantitative synthesis was attempted.
This article adheres to the Scale for the Assessment of Narrative Review Articles guidelines to ensure methodological transparency, comprehensive literature inclusion and balanced critical appraisal. If the scope is later expanded into a systematic review, a preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart and checklist will be incorporated to further enhance reproducibility and reporting standards.
Definitions and Diagnosis
Pancreatic Surgery
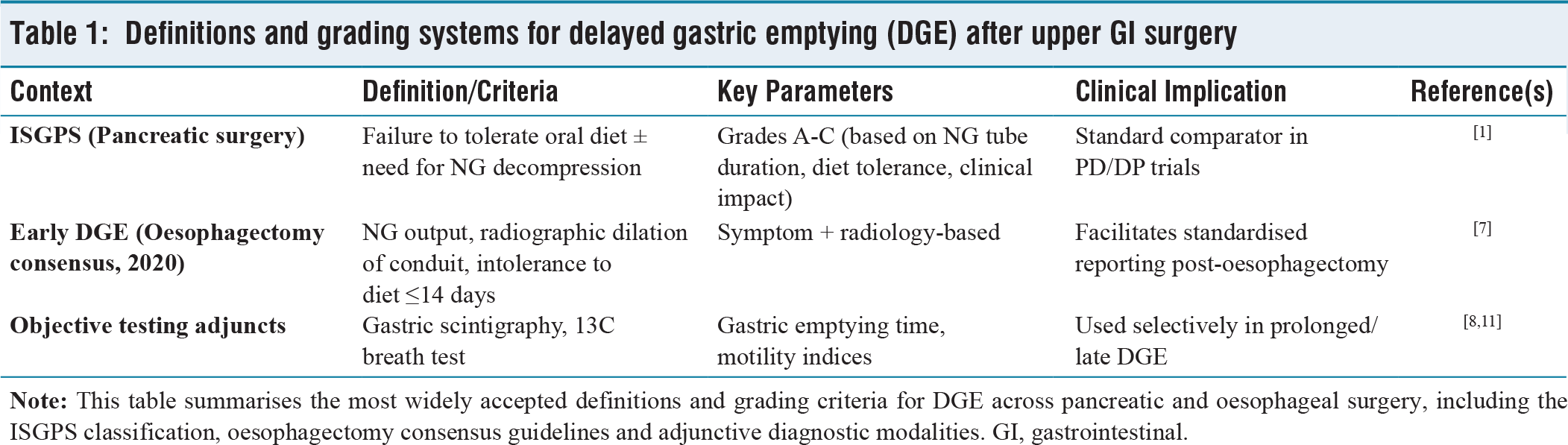
The ISGPS definition of DGE remains the standard comparator in pancreatic surgery, grading severity by failure to tolerate diet and the need for NG decompression (grades A-C).[1] Objective tests such as gastric scintigraphy are primarily research adjuncts in the immediate postoperative period but may have value in selected cases with persistent or late symptoms after discharge. In such patients, gastric scintigraphy or a 13C breath test can help differentiate true motility delay from functional dyspepsia, in line with approaches described for gastroparesis in broader gastroenterology guidelines.[8,11]
Oesophagectomy
In 2020, an international consensus group proposed criteria for early DGE after oesophagectomy (DGCE), emphasising NG output and radiographic conduit dilation within 14 days.[7] Comparative studies have demonstrated that while these criteria provide a standardised framework, they may underdiagnose patients who ultimately require pyloric interventions, reinforcing the importance of integrating clinical judgement with formal definitions.[7]
Table 1 provides a summary of existing definitions and grading systems for DGE in pancreatic and oesophageal surgery.
Definitions and grading systems for delayed gastric emptying (DGE) after upper GI surgery
Pathophysiology
The mechanisms underlying DGE are multifactorial and procedure-specific. Vagal disruption, antral or pyloric ischaemia and oedema, duodenal loss of motilin cycling, local inflammation from POPF, opioid-induced dysmotility and metabolic derangements such as electrolyte imbalance and hyperglycaemia all contribute to impaired gastric transit.[3,4,10,12] In oesophagectomy, conduit denervation, altered pyloric tone and conduit redundancy further exacerbate motility disturbances.[6]
Importantly, these mechanisms correspond to specific pharmacologic targets that underpin current and emerging therapies. Dopamine receptor antagonists such as metoclopramide and domperidone counteract dopamine-mediated inhibition of gastric contractility.[8,13] Macrolides such as erythromycin act as motilin receptor agonists, enhancing antral contractions, but are limited by tachyphylaxis.[12] Ghrelin agonists such as relamorelin promote gastric motor activity and accelerate emptying.[14–16] Meanwhile, 5-HT4 receptor agonists augment acetylcholine release at the enteric synapse, stimulating coordinated gastric and small bowel motility.[8,12]
Beyond direct motility effects, the interplay between inflammation, analgesia and metabolic control is pivotal. Inflammatory mediators released during POPF or intra-abdominal infection delay gastric transit by impairing neural coordination, explaining why DGE often resolves once sepsis is controlled.[3,4] Similarly, opioid analgesics exert dose-dependent inhibition of gastric peristalsis, reinforcing the importance of multimodal, opioid-sparing analgesic strategies.[10] Hyperglycaemia and electrolyte imbalance can independently suppress gastric contractility, highlighting the need for meticulous perioperative metabolic management.[12] Collectively, these overlapping pathways demonstrate why single interventions rarely abolish DGE and why multimodal, algorithm-based strategies remain essential for effective prevention and management.
Incidence and Risk Stratification
After PD
Clinically relevant DGE (ISGPS B/C) occurs in approximately 10%-30% of patients in contemporary cohorts, with risk strongly associated with POPF and intra-abdominal abscess, older age, preoperative biliary drainage, soft pancreatic texture, high opioid exposure and elevated preoperative bilirubin.[3–5,17] Large registry analyses and meta-analyses have refined these predictors and facilitated risk modelling, including the development of scoring systems such as predicting delayed gastric emptying after pancreaticoduodenectomy tool (PrEDICT)-DGE.[4,10,17,18] Recently, machine-learning-based risk tools have also been explored, although their external validity remains unproven and requires further multi-institutional testing.[19]
After Distal Pancreatectomy
DGE is less common than after PD, with large registry data suggesting an incidence of 5%-12% depending on definition and patient mix.[17] Predictors include both technical and patient-related factors, but the absolute burden is smaller compared to PD.
After Oesophagectomy
The reported incidence of early DGE varies widely, ranging from 15% to 35%, depending on whether only symptom-based or combined radiographic criteria are applied.[7] Institutions that incorporate radiographic assessment tend to capture more patients who ultimately require pyloric intervention.
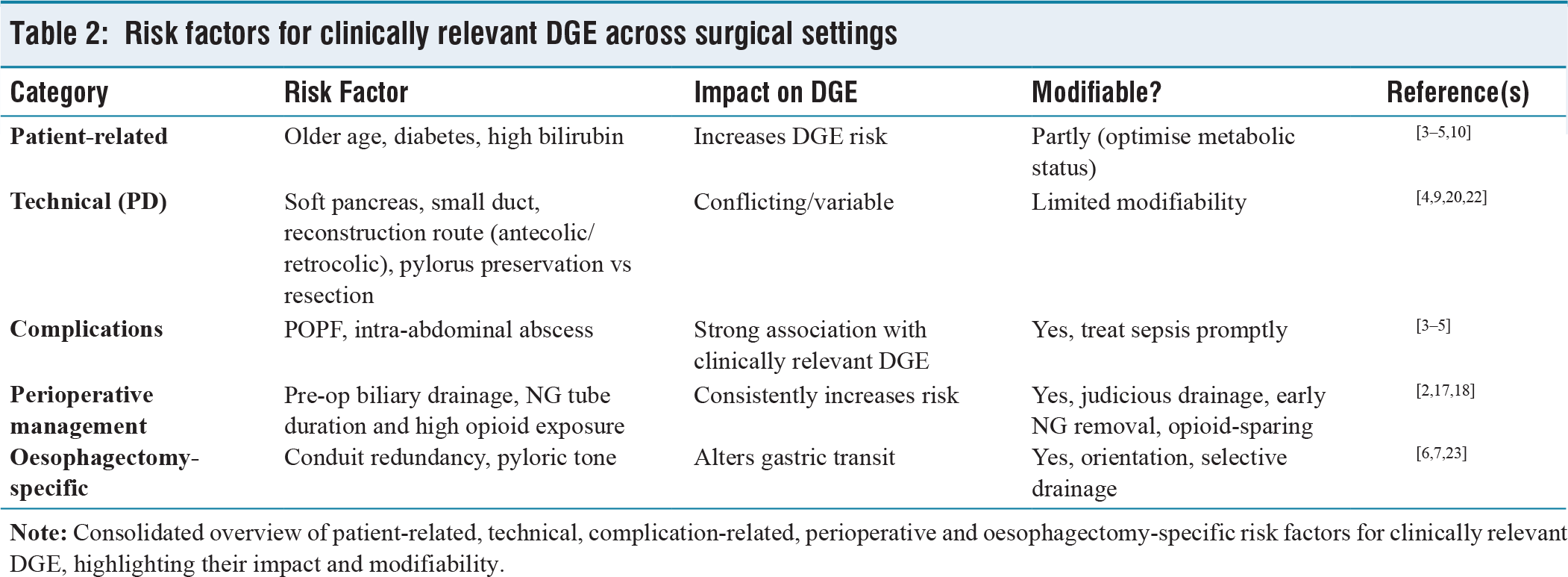
Modifiable predictors deserve special emphasis: Minimising perioperative opioid use through multimodal analgesia, judicious selection of patients for preoperative biliary drainage and careful timing of NG tube removal can all reduce the likelihood of clinically significant DGE.[2,5,18]
Table 2 outlines major risk factors for DGE, stratified by clinical category and highlighting those amenable to intervention.
Risk factors for clinically relevant DGE across surgical settings
Prevention: Operative Technique and ERAS
Gastro/duodenojejunostomy Route (PD)
Meta-analyses and comparative studies have shown conflicting results regarding antecolic versus retrocolic routing. While some earlier series suggested lower DGE with an antecolic approach, higher-quality syntheses demonstrate no uniform advantage; technique should therefore be individualised, prioritising avoidance of kinking and ensuring adequate vascularity.[9,20]
Pylorus Preservation vs Resection (PD)
The pylorus resection versus pylorus preservation trial (PROPP) trial demonstrated no reduction of DGE with pylorus-resecting PD compared to pylorus-preserving pancreaticoduodenectomy (PPPD)[21] and the quality of life and nutritional outcomes after pancreaticoduodenectomy trial (QUANUPAD) randomised trial confirmed no significant difference between classical Whipple and PPPD in terms of DGE incidence and severity.[22] Together, these data suggest that pylorus management strategies alone are unlikely to eliminate DGE risk.
Pyloric Manipulation (Oesophagectomy)
A 2024 meta-analysis of randomised trials concluded that intraoperative pyloric drainage is generally unnecessary.[6] Although earlier practice often favoured routine pyloroplasty or dilatation, pooled contemporary evidence demonstrates that such interventions may increase reflux-related sequelae without consistently preventing DGE, thereby supporting a selective approach rather than blanket application.[6]
Technical Pearls
Beyond these trial-driven considerations, practical surgical nuances remain essential. Proper orientation of the gastrojejunostomy, avoidance of redundant jejunal loops and meticulous construction of the mesenteric window reduce the risk of functional obstruction.[23] Single-centre comparative series emphasise that attention to these factors can significantly improve gastric transit and shorten recovery.[23] Furthermore, ensuring a tension-free anastomosis and minimising mesenteric torsion are key elements that complement the technical evidence provided by randomised trials.[21,22] Consistency in stapling technique, careful mesenteric handling and vigilant intraoperative assessment of gastric conduit orientation are additional safeguards that can prevent subtle but clinically relevant delays in emptying.[23]
ERAS Elements
Enhanced recovery protocols, including early mobilisation, selective NG tube removal, goal-directed fluid therapy, multimodal opioid-sparing analgesia and early enteral feeding, consistently mitigate the downstream consequences of DGE.[2] Early institution of jejunal feeding when gastric stasis is anticipated, together with active engagement of physiotherapy and dietetics, further optimises nutritional resilience.[2] Adherence to ERAS pathways has also been shown to shorten hospital stay and improve patient-reported recovery, underlining their central role in the holistic prevention of clinically significant DGE.[2]
Management: A Stepwise Prokinetic-centred Algorithm
Step 1: Exclude mechanical problems and treat contributors (post-op day 3–5 or when suspected).
Assess for anastomotic twist/kink, intra-abdominal collections or POPF; CT as indicated. Optimise electrolytes (K, Mg), control glucose, minimise/rotate opioids, consider epidural or non-opioid analgesics.[3,4,10]
NG decompression for symptomatic relief; keep tubes to the minimum necessary. ERAS-concordant hydration and mobilisation.[2]
Step 2: Initiate first-line prokinetic (short, monitored course).
Metoclopramide 10 mg PO/IV every 6–8 hours, reassess at 48–72 hours; limit course to the shortest effective duration (watch for akathisia, dystonia; avoid >12 weeks total exposure).[8,13]
Where available, domperidone 10 mg PO every 8 hours (ECG/QTc precautions; avoid in significant cardiac disease).[8,13]
Consider short course erythromycin (e.g., 125–250 mg PO/NG q8–12 h) when a rapid effect is desired, anticipating tachyphylaxis; reserve for monitored settings. (Support from gastroparesis literature; limited modern PD-specific RCT data.)[8,12]
Step 3: Escalate/adjuncts if inadequate by 72–96 hours.
5-HT4 agonists (where accessible) can accelerate emptying; evidence is evolving.[8]
Ghrelin agonist (relamorelin) has improved symptoms and gastric emptying in diabetic gastroparesis RCTs; not standard post-surgical care, but a consideration in trials or refractory cases with specialist input.[14–16]
Antiemetics (ondansetron, etc.) for symptom control; avoid anticholinergics or opioids that worsen motility.[8]
Step 4: Nutrition strategy.
If oral fails by day ~5–7 despite step 2, institute post-pyloric feeding (nasojejunal or jejunostomy) to meet targets; continue prokinetics and re-challenge gastric feeding periodically.[2,8]
Parenteral nutrition is reserved for refractory intolerance or when enteral access is unsafe.
Step 5: Pyloric interventions (select contexts).
Oesophagectomy conduit DGE: Endoscopic pyloric balloon dilatation after day seven is effective in institutional pathways; consider when criteria for early DGE are met or symptoms persist despite medical therapy.[7]
PD: Routine pyloroplasty/myotomy is not supported by RCTs; selective endoscopic pyloric therapy may be considered for proven pylorospasm in protracted cases (evidence limited; ongoing RCTs such as 2025 pyloromyotomy versus pyloric stretching for reduction of delayed gastric emptying trial [PORRIDGE] suggest interest).[21,22]
Selective pyloric interventions remain under investigation, with emerging randomized data including the PORRIDGE trial evaluating pyloric techniques aimed at reducing delayed gastric emptying after pancreatic surgery.[24,25]
Step 6: Rehabilitate and de-escalate.
As gastric transit recovers, step down medication burden, maintain small low-fat/low-fibre feeds and reassess opioids and glycaemic control.[8]
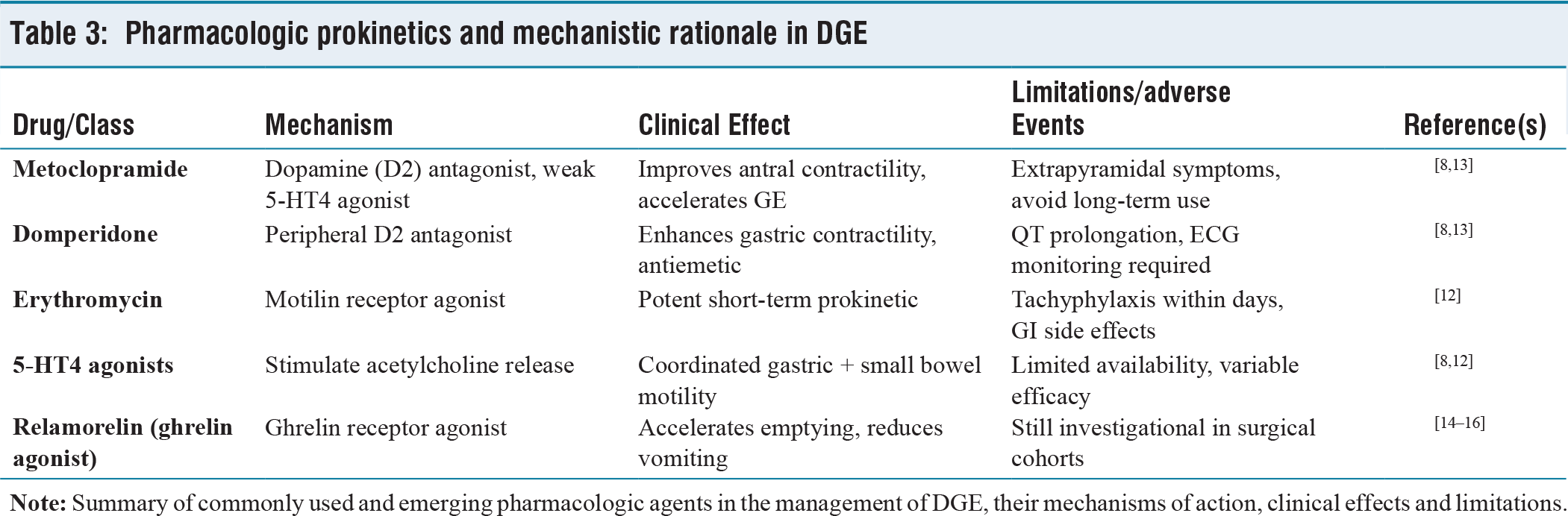
Table 3 details the pharmacologic agents used in DGE management, their mechanisms, efficacy and key limitations.
Pharmacologic prokinetics and mechanistic rationale in DGE
Special Scenarios
When POPF/infection Co-exists
Treating the septic source is paramount, as DGE often resolves once intra-abdominal inflammation abates.[3,4] This observation highlights that DGE is frequently a secondary phenomenon rather than a primary motility disorder and addressing the root complication usually restores gastric transit.
Distal Pancreatectomy
DGE is less common after distal pancreatectomy (DP), with an incidence of around 5%–12%.[17] Although its clinical impact is milder than after PD, patients who develop DGE can still experience prolonged recovery and impaired nutritional intake. Management mirrors that of PD, with particular attention to ERAS adherence, minimisation of opioid exposure and early mobilisation to support gastric motility.[2,17]
Oesophagectomy
Early DGE after oesophagectomy occurs in 15%-35% of cases, depending on the diagnostic criteria applied.[6,7] These patients often require endoscopic interventions such as balloon dilatation when medical therapy fails. Because definitions differ across institutions, reported incidence varies, underscoring the need for harmonisation of diagnostic standards.[7] The absence of benefit from routine pyloric drainage in randomised trials strengthens the argument for a selective, criteria-driven approach.[6]
Patient-centred Outcomes
While DGE prolongs recovery and worsens short-term quality of life by delaying oral intake and increasing dependence on NG or jejunal feeding, most series demonstrate that it rarely compromises long-term oncologic outcomes after PD.[2,4,5] This distinction is essential in counselling patients: DGE should be framed as a temporary but reversible challenge rather than a determinant of cancer prognosis. Clear communication about expected recovery timelines and reassurance on oncologic outcomes can significantly improve patient satisfaction and reduce anxiety during postoperative care.
Conclusion
Postoperative DGE is not one problem but a family of motility setbacks with overlapping mechanisms. Definitions are improving (ISGPS; oesophagectomy consensus), but management success springs from algorithms that: Exclude obstruction, treat drivers (sepsis, opioids, electrolytes), adopt ERAS rigour and apply time-limited prokinetics with stepwise escalation to post-pyloric feeding and selective pyloric therapy. The proposed pathway is evidence-aligned yet pragmatic; future RCTs should test bundled protocols rather than isolated levers. Equally important, attention to modifiable perioperative factors, integration of surgical ‘pearls’ and patient-centred outcome measures will ensure that advances in DGE prevention and treatment translate into tangible improvements in recovery, satisfaction and resource utilisation.[2–7,23]
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval statement
Ethical approval was not required for this study as it represents a narrative review of previously published literature and does not involve human participants, patient data, or experimental interventions.
Credit author statement
Dr Supreet Kumar conceived the review, performed the literature synthesis and drafted and finalised the manuscript.
Data availability
Data sharing is not applicable to this article as no datasets were generated or analysed.
Use of artificial intelligence
No AI-assisted tools were used for language refinement or formatting. All scientific content, analysis and interpretations are original and the responsibility of the author.