
Abstract
Background and Aims:
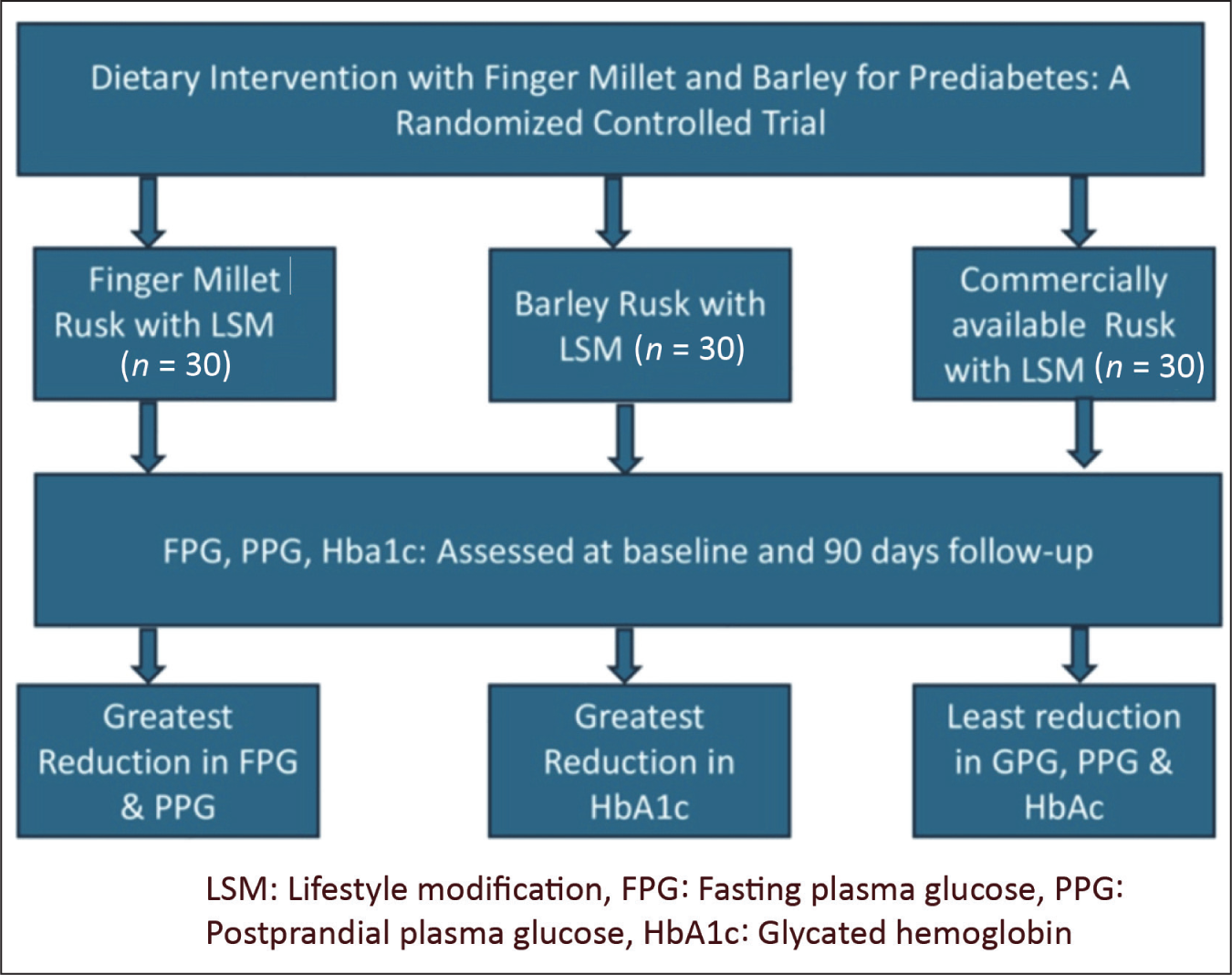
In India, one in four people has obesity, diabetes or prediabetes. India has around 101 million people with diabetes and 136 million people with prediabetes. Each year, approximately 5%-10% of individuals with prediabetes progress to type 2 diabetes. Lifestyle modification, including dietary changes, is key to prevention and management. This study examined the efficacy of finger millet (Eleusine coracana) and barley (Hordeum vulgare) diets, combined with lifestyle modifications, in the management of prediabetes.
Methods:
A 90-day, randomised, controlled, single-blinded, multi-arm experiment with 90 people with prediabetes in three groups was conducted. Group A received finger millet, Group B barley and Group C a standard diet with lifestyle modifications. All groups were encouraged to exercise 150 minutes per week at moderate intensity. Six follow-ups were done. Changes in fasting and postprandial plasma glucose, HbA1c were the primary objective analysed at baseline and 90 days.
Results:
The results showed significant reductions in fasting plasma glucose (P < .001) and postprandial plasma glucose (P < .05) between Groups A and B and Groups A and C. Additionally, HbA1c levels show statistically significant results (P < .001) between Groups A and B and Groups B and C. There were no significant adverse events in all the groups.
Conclusion:
Our study revealed the effectiveness of dietary interventions involving finger millet, barley and lifestyle modifications in the management of individuals with prediabetes.
Introduction
Prediabetes represents a condition of dysglycaemia that exists between normal blood glucose levels and diabetes mellitus. The American Diabetes Association (ADA) defines the diagnostic criteria for prediabetes as glycated haemoglobin (HbA1c) levels ranging from 5.7% to 6.4%, FPG levels between 100 mg/dL and 125 mg/dL, and two-hour PPG levels of 140 mg/dL to 199 mg/dL.[1,2] Individuals with prediabetes exhibit a significantly increased risk of progressing to type 2 diabetes mellitus (T2DM). The risk of progression can be significantly reduced through dietary modifications and increased physical activity.
Numerous high-quality evidence demonstrate that lifestyle modification (LSM) can effectively postpone or avert the onset of T2DM. In the Chinese Da Qing study, participants with prediabetes who engaged in lifestyle treatments had a relative risk decrease of 31%-46% over six years in comparison to control groups.[3] The Finnish Diabetes Prevention Study documented a 58% reduction over three years, but the Indian Diabetes Prevention Program noted an approximate 30% relative risk reduction by lifestyle adjustments and metformin.[4,5] Pharmacological interventions may be useful for high-risk patients; however, lifestyle adjustments often provide greater long-term benefits without the adverse effects associated with drugs. A systematic review and meta-analysis confirmed that lifestyle modifications reduce the risk of diabetes for up to 10 years.[6] Over 15% of individuals in Uttar Pradesh, India exhibit prediabetes, with a diabetes-to-prediabetes ratio of less than 1:2. A significant proportion of individuals with prediabetes are at risk of progressing to diabetes if timely intervention is not provided.[7]
Millet (Eleusine coracana, Hordeum vulgare and other species) is a nutritious grain that remains underutilised despite its numerous health benefits.[8] It resembles wheat and rice. Millets exhibit a low glycaemic index (GI 54–68), a moderate glycaemic load (GL 12–20 per 100 g) and a high dietary fibre content (72–76 g carbohydrates per 100 g, predominantly non-starchy carbohydrates). They are rich in proteins, polyunsaturated fatty acids (PUFAs), vitamins, minerals and phytochemicals.[8–10] In vitro studies indicate that millet phenolic compounds inhibit carbohydrate-hydrolysing enzymes, resulting in reduced postprandial hyperglycaemia. Barley includes a high content of both insoluble and soluble dietary fibre, with the majority of the soluble fibre being β-glucan. β-glucan has been indicated to mitigate the risk of cardiovascular diseases through its cholesterol-lowering properties and other benefits. In vivo studies indicate that whole-grain and finger millet flours provide protection against hyperglycaemia and oxidative stress while also promoting wound healing.[9–12] Notwithstanding the multiple benefits of millet, its intake in India is minimal owing to insufficient awareness among the populace. Such grains are commonly termed ‘orphan cereals’ because of their limited utilisation. In our region, individuals with and without diabetes frequently consume tea and rusk. There is a lack of data concerning the use of millet-based preparations in individuals with prediabetes. We hypothesised that dietary supplementation with finger millet or barley, along with LSM, would result in significant improvements in glycaemic and metabolic parameters in prediabetic adults compared to lifestyle modification alone.
Methods
Study Design
This was a randomised, controlled, single-blinded, multi-arm clinical trial conducted in accordance with the principles of Good Clinical Practice and the Declaration of Helsinki. The final study protocol and informed consent forms were approved by the Institutional Ethics Committee (IEC) and registered prospectively with the Clinical Trials Registry of India. Written informed consent was obtained from all participants before enrolment.
Participants
Participants were recruited from the outpatient department of a tertiary care centre in Uttar Pradesh, North India between October 2023 and October 2024. Eligible subjects were adults aged 18–65 years of either sex, diagnosed with prediabetes as per ADA criteria: HbA1c 5.7%–6.4%, FPG 100–125 mg/dL and PPG 140–200 mg/dL. Inclusion criteria required willingness to provide written informed consent and comply with the study protocol. Exclusion criteria included pregnancy or lactation; age <18 or >65 years; plasma glucose values outside the specified ranges; known systemic illnesses (e.g., chronic kidney disease, chronic liver disease or coronary artery disease) and unwillingness to adhere to dietary and LSMs.
Sample Size
The sample size was estimated using following formula n = (r + 1) (Z α/2 + Z 1-β) 2 σ2 /rd2 where n = sample size required, d = expected mean difference in HbA1c = 15.8, Zα/2 = 1.96 (P < .05), Z1-β = 1.28 (90%), the sample size ratio necessary for two groups is r = n1/n2 (1:1:1), σ = common standard deviation = 22.3 was obtained from a previous study.[13] Based on prior research, the expected mean difference and standard deviation were determined, leading to an initial calculated sample size. Considering a 20% expected dropout rate, the final estimated sample size was 90 participants, distributed equally across three groups.
Randomisation and Allocation
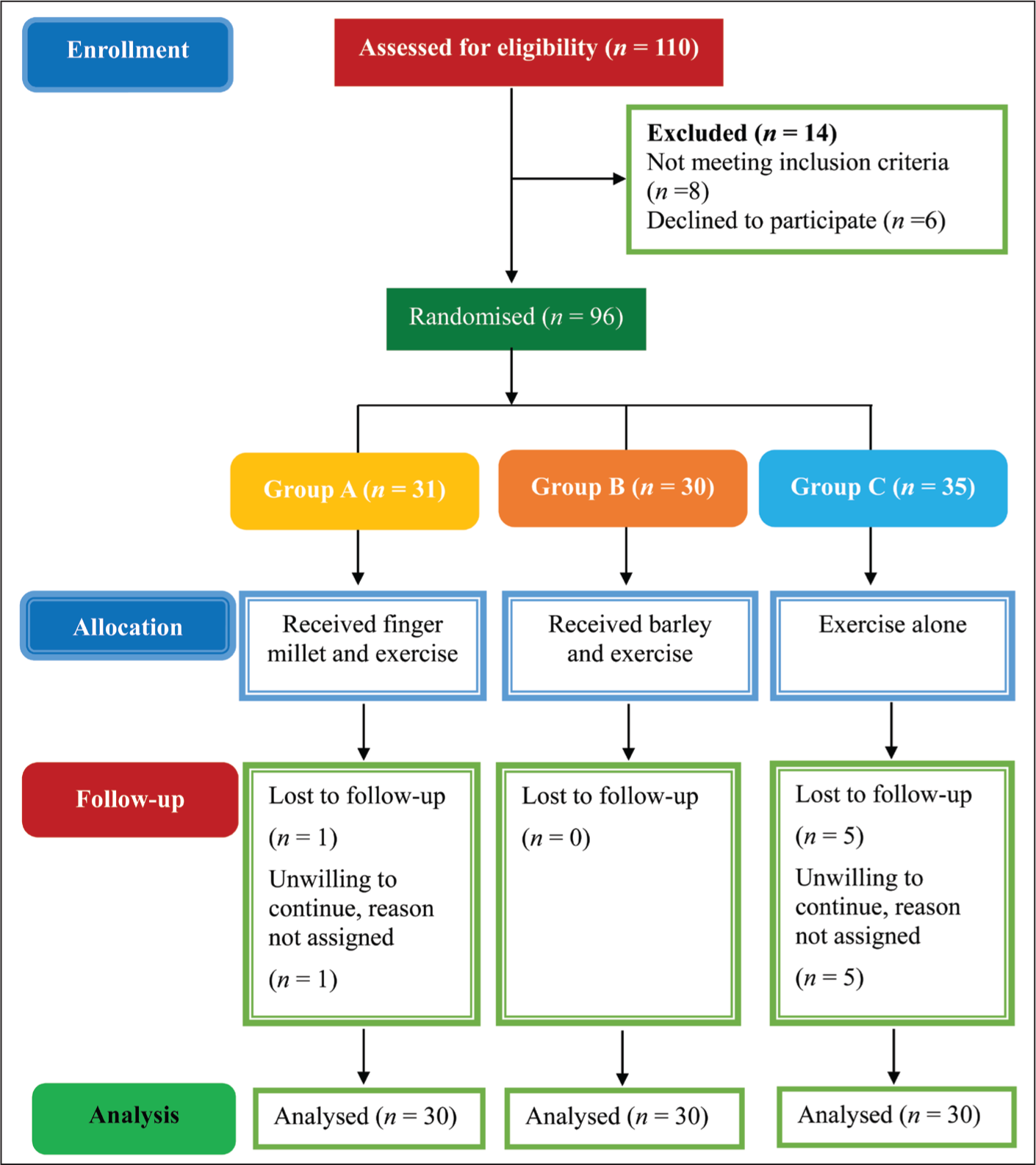
Participants were randomised into three groups using a computer-generated random sequence obtained from www.randomization.com. Figure 1 illustrates the enrolment process and the progression of participants throughout the study.
Flow chart of the study process (adapted from the CONSORT flow chart)
Study Interventions
All participants were prescribed a structured aerobic exercise regimen of at least 150 minutes per week at moderate intensity (50%–70% maximum heart rate), as per ADA recommendations. Standardized dietary counselling was provided by a qualified dietitian, advising avoidance of high-glycaemic index foods, refined sugars, deep-fried foods and calorie-dense snacks to ensure dietary uniformity across groups.
Test Intervention
Group A: Finger millet rusks (~56 g/day; four rusks of ~14 g each, consumed at breakfast).
Group B: Barley rusks (~56 g/day; prepared and consumed as in Group A).
Group C: Standard diet only, with LSM (control).
The rusks were prepared using a standardised formulation: 80 g test flour (finger millet or barley), 20 g whole wheat flour, 10 g skimmed milk, 6 g jaggery, 9 g mustard oil and 1 g yeast, yielding nine rusks per 126 g dough. Technical support was provided by the Department of Post-harvest Engineering and Technology [Figure 1].
Outcome Measurements
Primary outcome measures included HbA1c (measured at baseline and day 90), FPG and PPG measured at baseline and every 15 days (days 15, 30, 45, 60, 75 and 90). Secondary outcome measures included haemoglobin, serum triglyceride and serum calcium measured at baseline and day 90 to assess nutritional impact and metabolic effects. All laboratory measurements except PPG were performed on fasting blood samples drawn after an overnight fast.
Follow-up and Adverse Events
Follow-up visits occurred on days 15, 30, 60, 75 and 90. Adverse events were assessed using the Naranjo Causality Assessment Score, and severity was graded using the Modified Hartwig and Siegel Scale. Withdrawal criteria included non-compliance or the occurrence of adverse effects.
Statistical Method
Continuous variables were expressed as mean ± SD (minimum-maximum), while categorical variables were summarised as counts and percentages. Within-group comparisons were performed using paired t-tests; between-group differences were assessed with unpaired t-tests. Data analysis was carried out using SPSS v22.0 and R v3.2.2, with Microsoft Excel and GraphPad InStat v3.06 used for visualisation. The statistician remained blinded to group allocation to minimise bias. A P value <0.05 was considered statistically significant.
Results
Demographic Characteristics
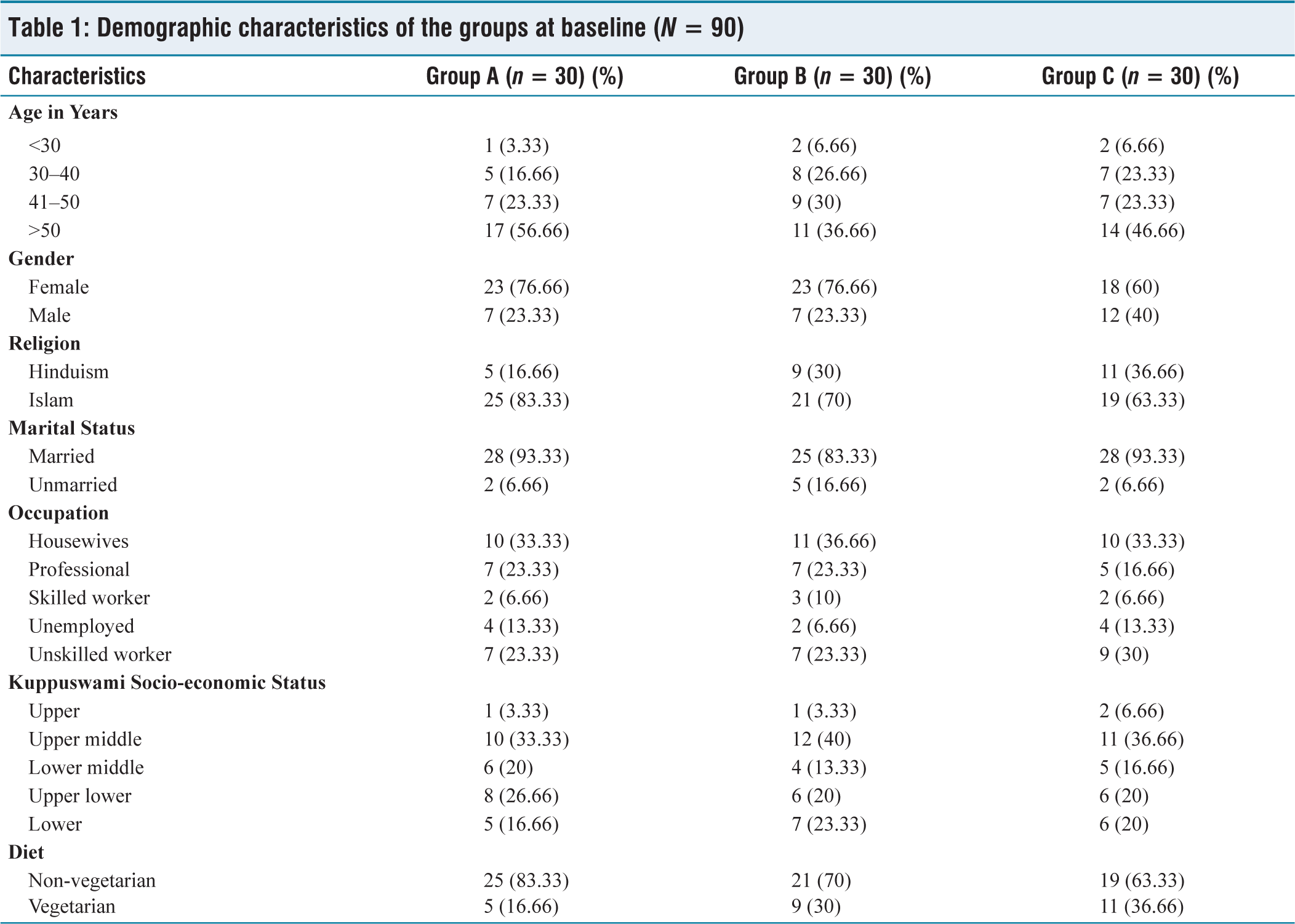
The mean age was 47.2 ± 8.5 years, 71.1% were females and 27.8% followed a vegetarian diet. There were no statistically significant differences between the groups at baseline, confirming effective randomisation. The baseline demographic features have been provided in Table 1.
Demographic characteristics of the groups at baseline (N = 90)
Glycaemic Parameters
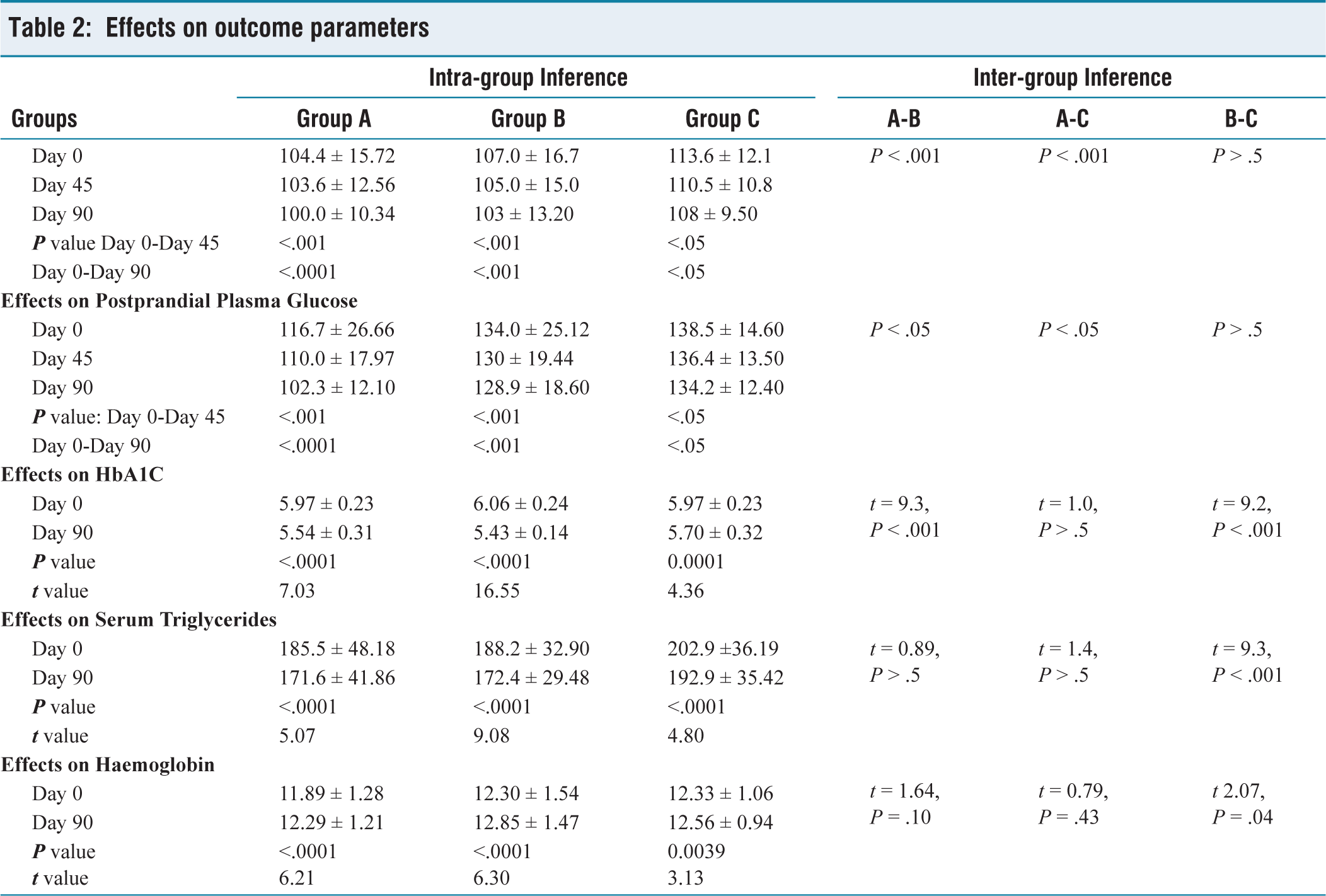
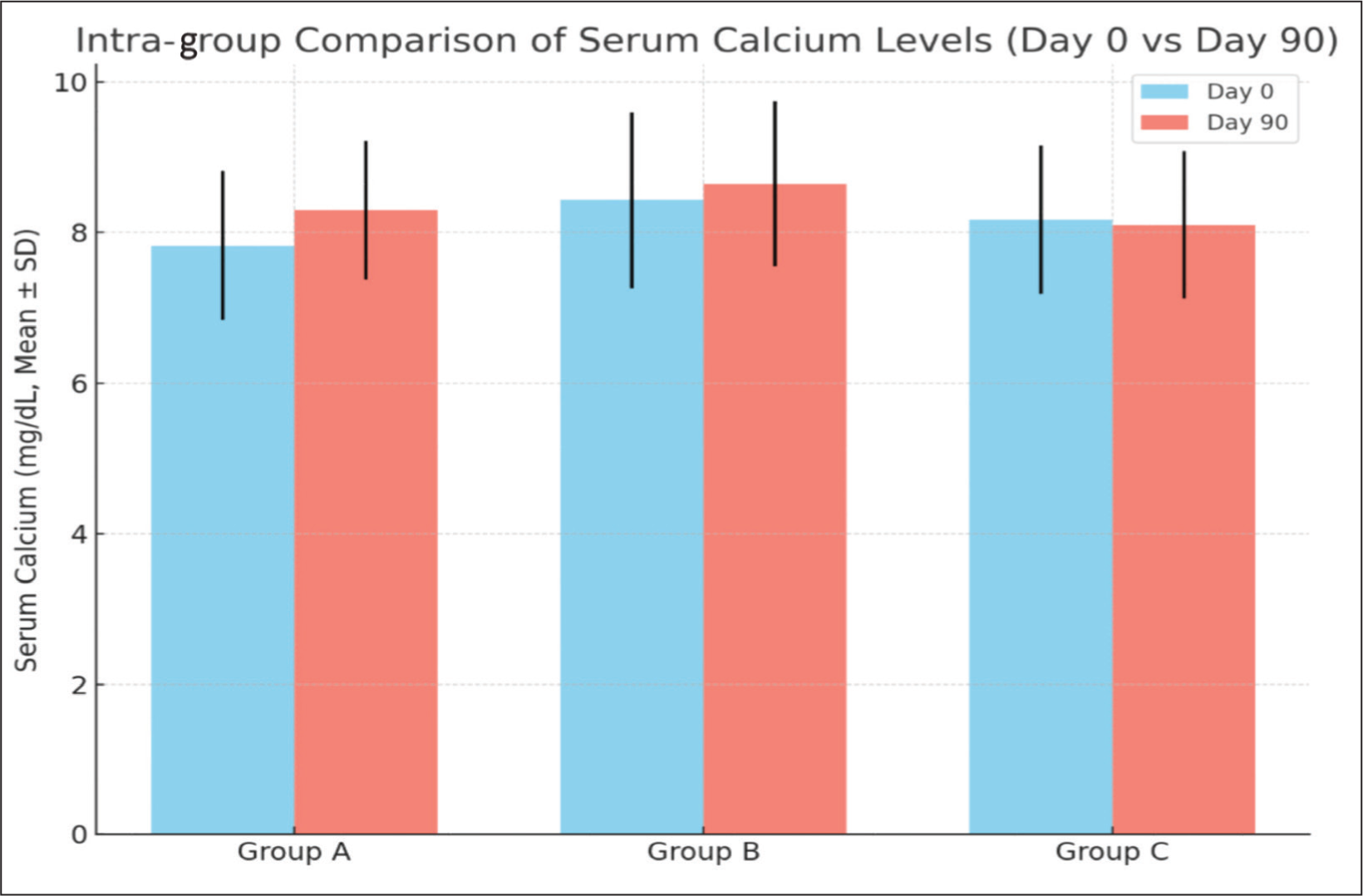
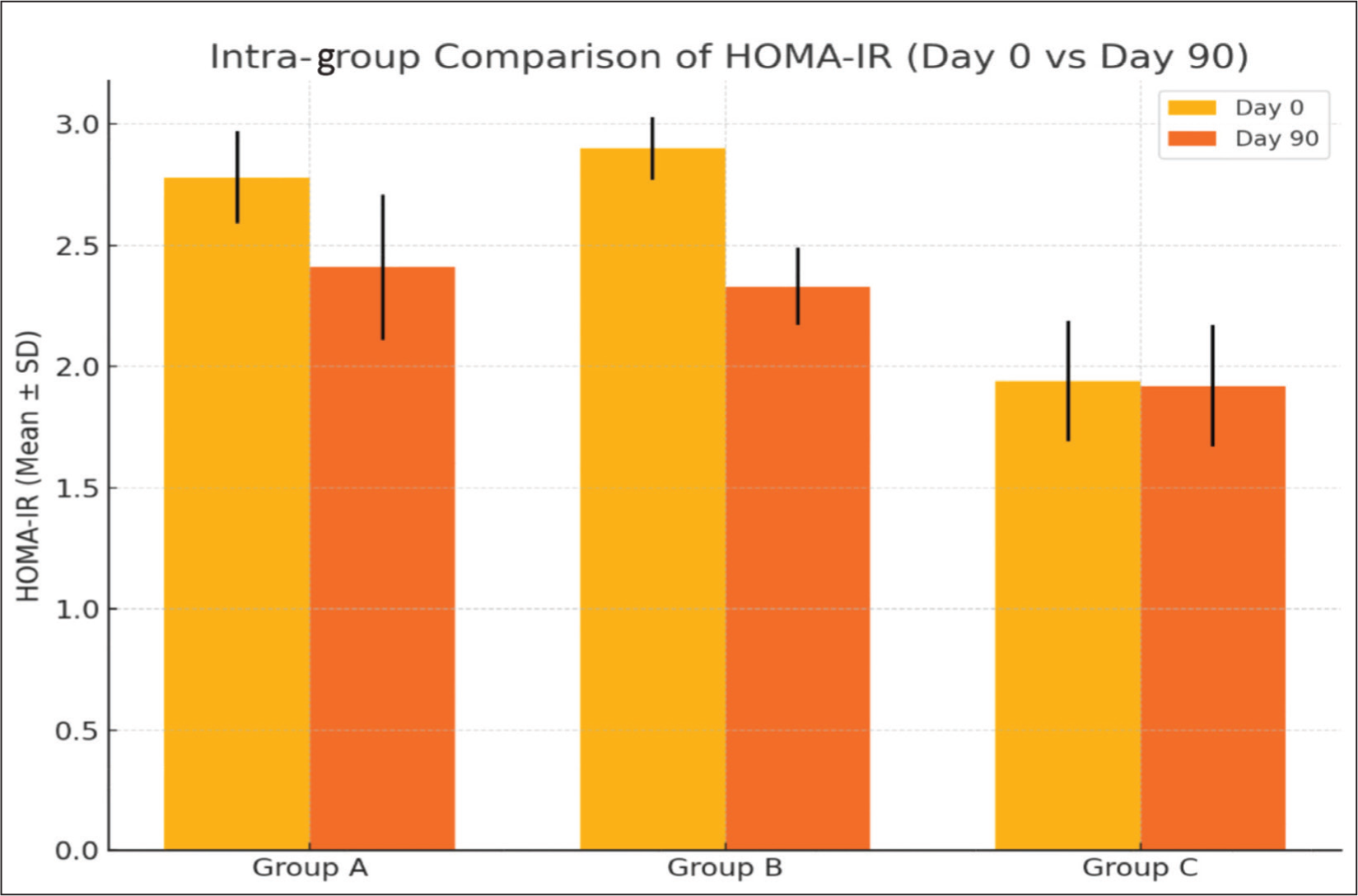
Over the 90-day intervention, all three groups showed significant improvements in FPG, PPG, HbA1c and serum triglycerides, with Group A demonstrating the greatest reductions in FPG and PPG (P < .0001), followed by Group B (P < .001) and Group C (P < .05). HbA1c decreased significantly in all groups, revealing significant differences between Group A and B, and between Group B and C (P < .001). Serum triglycerides significantly improved across groups, with inter-group differences favouring Group B over Group C (P < .001). Haemoglobin levels increased slightly but significantly in all groups; however, significant inter-group differences were observed only between Group B and Group C (P = .04). These results underscore the superior efficacy of finger millet and barley interventions combined with LSM in improving glycaemic and metabolic parameters relative to standard diet alone [Table 2]. Serum calcium levels improved significantly in Groups A and B compared to Group C [Figure 2]. Inter-group comparisons demonstrated statistically significant differences between all groups (P <.001). HOMA-IR analysis, conducted on a representative subset of participants, showed a more pronounced reduction in insulin resistance in GroupsA and B compared to GroupC [Figure3]. This improvement is likely attributable to the high dietary fibre content of finger millet and barley, which may enhance insulin sensitivity and glycaemic control.
Effects on outcome parameters
Effects on serum calcium
Effects on HOMA-IR
Discussion
Diet and lifestyle modification remain the cornerstone of the management of individuals with prediabetes. Millets are tiny grains belonging to the Poaceae family. These are crops that thrive in India and yield a single harvest per year. India is the largest producer of millets, accounting for almost 40% of the global total.[13] Consequently, millets serve as an excellent alternative to refined cereals due to their high fibre content, low glycaemic index and low glycaemic load. We conducted this study to assess the efficacy and safety of interventions involving finger millet and barley, in conjunction with lifestyle improvements, against LSMs alone in patients with prediabetes. The results revealed clinically and statistically substantial benefits in several glycaemic and non-glycaemic parameters. Within the group analysis of FPG and PPG, Group A demonstrated the most significant reduction (finger millet with exercise; P < .0001). Among the groups, the comparison validated Group A’s greater efficacy compared with Group B and Group C (P < .001). Inter-group differences favoured Group A over Group B and Group C (P < .05). HbA1c values, evaluated at baseline and day 90, exhibited a significant reduction across all groups, with marked inter-group differences between Group A and Group B, as well as between Group B and Group C (P < .001). Serum triglyceride declined significantly in all the groups (P <.0001), with Groups B and C showing the largest inter-group differences (P <.001). Haemoglobin levels rose slightly but significantly in Groups A and B (P <.0001) and C (P = .003), with Groups B and C showing significant inter-group differences (P = .0429). The groups experienced a significant improvement in serum calcium levels (P < .0001 for Groups A and B; P = .0002 for Group C). Significant differences between Groups A and B, Groups A and C (P < .001) and Groups B and C (P < .01) were observed during inter-group comparisons. Groups A and B showed a more noticeable improvement in insulin sensitivity, as assessed by HOMA-IR analysis in a subset of participants.
Better glycaemic control in groups A and B can be attributed to the high soluble dietary fibre content, which slows glucose absorption, as well as its bioactive components, such as phenolics and tannins.[14] The inhibition of α-glucosidase and α-amylase delays carbohydrate digestion and absorption, consequently promoting a delayed and subtle rise in postprandial glucose levels—mechanisms regarded to be vital in the management of postprandial hyperglycaemia. These findings are similar to previous studies[15–19] and presumably indicate the elevated β-glucan content in barley, which delays gastric emptying, slowing glucose absorption and better postprandial glycaemic control. Improvement in the lipid parameters can be an effect of β-glucan, which can enhance lipid metabolism. This is consistent with results of previous studies.[20] Improvement in haemoglobin levels are in line with past research showing that barley consumption may substantially increase haemoglobin levels.[21] Also, improvements in calcium values are consistent with previous research and data from the Nutritive Value of Indian Foods (ICMR), which show that finger millet is one of the cereals with the highest calcium content, with about 344 mg of calcium per 100 g.[22,23] According to Jagati et al., the calcium content of finger millet is approximately three times higher than that of milk and 10 times higher than that of wheat, maize or rice. This demonstrates its potential to help prevent calcium deficiency. Better insulin sensitivity may be due to finger millet’s high fibre and polyphenol content, and to barley’s β-glucan, both of which have been demonstrated to improve insulin sensitivity and lower insulin resistance, and are probably responsible for the effects.[24–26] To assess the safety of the intervention, haematological and biochemical tests, including liver and renal function tests, were performed at baseline and post-treatment. No significant alterations were observed, indicating that the intervention was well tolerated and did not adversely affect these parameters. None of the study participants discontinued the intervention because of adverse events.
This randomised, controlled, single-blinded, multi-arm clinical trial provides valuable insights into the effects of finger millet and barley rusks, alongside lifestyle modification, on glycaemic control in individuals with prediabetes. One of the major strengths lies in its pragmatic design, which reflects a real-world approach by avoiding strict dietary restrictions throughout the day. While this enhances the external validity of the findings, it also presents a limitation, as dietary intake variability may have influenced individual outcomes. In real-world settings, complete dietary control is often impractical; however, future research may benefit from integrating more systematic dietary adherence measures to enhance the likelihood of causality. The relatively short duration of the intervention and hospital-based study limits the ability to assess the long-term sustainability of the observed improvements. Prolonging the study period and including a post-intervention follow-up would help determine how long the beneficial effects can be maintained during the prediabetic stage.
The findings of our study demonstrate clinically that targeted dietary interventions with finger millet and barley, combined with lifestyle modifications, offer a practical and effective strategy for managing prediabetes, particularly significant in populations with high prevalence, such as India. These findings highlight the potential for accessible, culturally relevant food-based approaches to reduce progression to T2DM. Future research should explore the long-term sustainability and cost-effectiveness of these interventions in larger, multi-ethnic cohorts and investigate the underlying physiological mechanisms and dose-response relationships to optimize their therapeutic utility.
Footnotes
Acknowledgements
The authors are grateful for the facilities provided by the Chairperson of the Ilaj-Bit-Tadbeer Department, Ajmal Khan Tibbiya College and Hospital, AMU Aligarh, UP (India), during the trial and the patients who participated in the trial.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional Ethical Committee Approval Number
D.NO.1401/FUM, dated 1 May 2023.
Informed Consent
Written and informed consent was obtained from all the study participants.
Patient Consent
Consent was obtained from the participants at the time of recruitment. The same has been mentioned in the methodology part.
Credit Author Statement
Dr Rafat Afzal: Conceptualisation, data curation, writing the original draft, editing, data formal analysis, validation, investigation and conducted clinical research work for the thesis.
Professor Asia Sultana: Supervision, methodology, validation and guidance for the research.
Dr Hamid Ashraf: Co-supervision, editing and validation.
Dr Mohammad Shoaib: Co-supervision and contribution to the research.
Professor ZRA Ahmad Azad: Assisted in quantitative analysis related to rusk formation.
All authors have read and approved the final manuscript.
Data Availability
Data is available from the authors.
Credit Note
All authors are equally credited for their invaluable contributions to the conception, design, execution and interpretation of the research. Each author has read and approved the final version of the manuscript and agrees to take public responsibility for its content.
Use of Artificial Intelligence
Artificial Intelligence was not used in the preparation of this manuscript.