
Abstract
Introduction:
The serum calcium levels are likely to drop following thyroid surgery due to the manipulation of adjacent parathyroid glands, which regulate serum calcium. Hypocalcaemia is a well-recognised complication of thyroidectomy. Severe hypocalcaemia is a morbid complication of thyroidectomy.
Methods:
A comprehensive review of literature from databases like Google Scholar, PubMed, Medline, and Scopus was conducted to discuss serum calcium levels in patients following thyroid surgery.
Results:
Following thyroid surgery, low serum calcium is caused by transient or persistent hypoparathyroidism. Postoperative hypocalcaemia results in patient discomfort, prolonged hospital stays, and higher treatment costs.
Conclusion:
Postoperative hypocalcaemia usually occurs following extensive thyroid surgery and may need calcium and/or vitamin D supplements to alleviate or prevent the clinical symptoms.
Introduction
The monitoring of the serum calcium following thyroid surgery is very crucial, as injury or removal of parathyroid glands can lead to hypocalcaemia. Calcium homeostasis is maintained by different metabolic processes that keep the plasma concentration of calcium within narrow limits, ranging from 8.8 to 10.4 mg/dl.[1] These metabolic processes are orchestrated by parathyroid hormone (PTH), thyroid hormone, vitamin D, calcitonin, phosphorus and magnesium.[1] Hypocalcaemia following thyroid surgery is a well-known complication in patients, and it delays the hospital stay.[2] A total blood calcium level below the lower limit of the centre-specific reference range is known as hypocalcaemia.[3] Hypocalcaemia is more common and potential life threatening among patients undergoing total thyroidectomy.[4] Hypocalcaemia following thyroid surgery can cause severe morbidities that affect the patient’s quality of life and require serial laboratory serum calcium monitoring, prolonged hospitalisation, and treatment.[4] Neurological and cardiac consequences, which can include muscle cramps, tetany, seizures, prolonged Q-T syndrome, disorientation, and perioral and peripheral paraesthesia, are frequently among the clinical signs of hypocalcaemia.[5] The objective of this review is to discuss serum calcium levels in patients following thyroid surgery, including clinical presentations and their management.
Methods of Literature Search
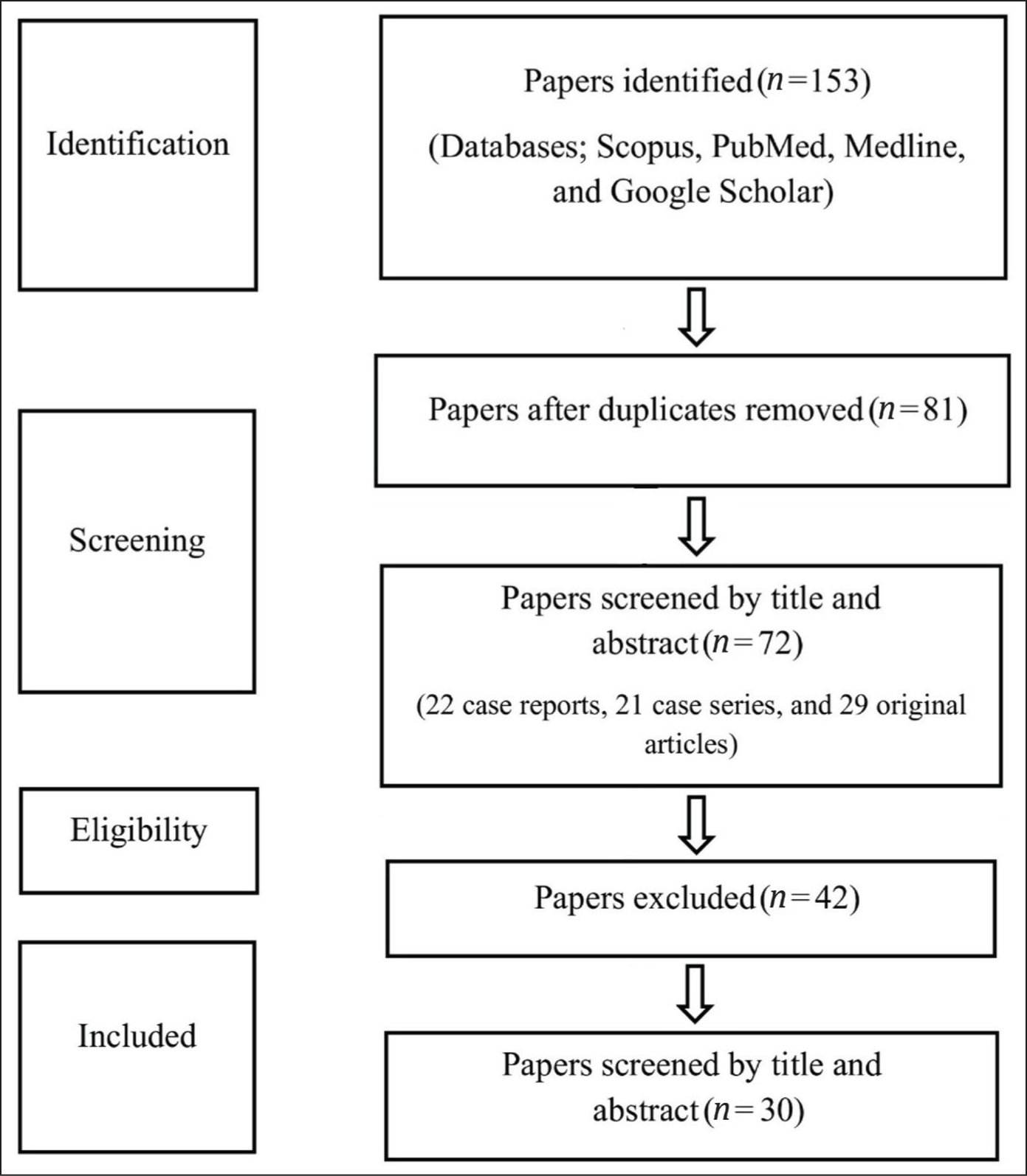
A search was done for research articles on the serum calcium levels in patients following thyroid surgery using various methods. This began with searching online databases such as Google Scholar, PubMed, Scopus, and Medline. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) served as the foundation for the development of a search strategy. This method located published article abstracts, and more research articles were manually located using citations. Evaluations were conducted to determine whether observational studies, case series, comparative studies, case reports, and randomised controlled trials were appropriate for this review. Across databases, a total of 72 papers (22 case reports, 21 case series, and 29 original articles) were located; 30 of them were included in this evaluation [Figure 1].
Methods of literature search
Prevalence
Thyroidectomy is a common surgery performed worldwide. The incidence of thyroid diseases and thyroid surgery has increased over the years.[6] Hypocalcaemia is a frequent complication among patients who have undergone thyroidectomy, occurring in as many as 30% of patients.[6] The incidence of temporary hypocalcaemia (decrease in calcium levels following thyroidectomy that lasts for 6–12 months) is 63.7%.[7] Another study showed that the incidence ranged between 50% and 68%, particularly following total thyroidectomy.[8] According to a study, the incidence of hypocalcaemia after thyroid surgery varies greatly, ranging from 1.7 to 68%; however, this significant variance may be caused by differing classifications.[9] The majority of thyroidectomy-related hypocalcaemia instances are temporary, however 1.5%-4% of procedures may result in permanent hypocalcaemia, which may be caused by hypoparathyroidism.[1]
Serum Calcium
The most prevalent mineral in the human body is calcium. About 98% of an adult’s 1,200 g of calcium is found in the skeleton as hydroxyapatite.[9] Calcium, phosphorus, and hydroxide combine to form the lattice-like crystal known as hydroxyapatite. The extracellular fluid (50%) and various tissues, particularly skeletal muscle, contain the remaining calcium. A relatively small range of 8.5–10.5 mg/dl (4.3–5.3 mEq/L or 2.2–2.7 mmol/L) is maintained for calcium.[10] The calcium homeostatic system is dependent on a number of substances, including magnesium, phosphate, vitamin D, and PTH.[11] In order to rectify changes in the steady state level of serum calcium, PTH acts as a receptor arm. PTH secretion will rise rapidly in response to a slight decrease in ionised calcium. This rise in PTH causes calcium to be released from bone more quickly. This release is not reliant on bone turnover or an increase in osteoclasts, but it does require the active form of vitamin D, 1,25-dihydroxycholecalciferol.[9]
Causes of Hypocalcaemia
The medical literature has a wide range of definitions for postoperative hypocalcaemia. Some authors use biochemical data, such as calcium and PTH levels, while others emphasise the existence of clinical symptoms that necessitate intravenous or oral calcium and vitamin D supplements.[11] Multifactorial hypocalcaemia can be caused by parathyroid excision, devascularisation, and gland damage, which can lead to either temporary or chronic hypoparathyroidism.[11] This situation is undoubtedly caused by the associated processes, such as vitamin D deficiency, calcitonin realisations, and hungry bone syndrome.[11] Vitamin D plays a crucial part in maintaining calcium homeostasis in the body. Risk variables such as age, gender, gland size, thyroid disease type, presence of inflammation and fibrosis, extent of thyroidectomy, and lymph node dissection are frequently linked to problems following thyroidectomy.[12] Though about 10% of patients may experience persistent hypocalcaemia, postoperative hypocalcaemia is typically temporary and can be brought on by both hypoparathyroidism and an imbalance between electrolyte levels and hydration.[13]
A drop in PTH levels below the laboratory standard’s lowest normal limit, often 12 pg/mL, combined with hypocalcaemia, is known as biochemical hypo-parathyroidism.[3] According to a study, comorbidities, advanced disease, and advanced age are significant risk factors for complications following thyroidectomy, particularly in cases of thyroid cancer.[14] Hypocalcaemia may be temporary or permanent. A drop in calcium levels that lasts for 6–12 months after thyroidectomy is known as temporary hypocalcaemia.[15] On the other hand, a drop in serum calcium levels following a total thyroidectomy that lasts more than a year is known as permanent hypocalcaemia.[16] Temporary hypocalcaemia following thyroidectomy is more likely to occur in patients with low calcium levels prior to thyroid surgery. Permanent hypocalcaemia is more likely to occur if the calcium level is less than 1.88 mmol/L in the first 24 hours after thyroid surgery.[15] The risk of developing transient post-thyroidectomy hypocalcaemia increased to 69%–100% if the postoperative parathyroid level dropped to 6–35 pg/mL within an hour to a day after thyroid surgery.[15] A multivariate analysis reveals that female sex and advanced age are important risk variables for hypocalcaemia following thyroidectomy.[17] Age has little effect on the development of hypocalcaemia following thyroidectomy, according to another study.[16] However, some research revealed that young people are more likely to experience transient hypocalcaemia following thyroidectomy, while other investigations found that older patients are more likely to experience this condition.[15,17] However, a study showed that post-thyroidectomy patients presented with hypocalcaemia more often among female patients.[18]
According to some authors, maintaining normal gland function only requires one parathyroid gland. Others, however, think that in order to restore the glands’ normal functions, at least three parathyroid glands are required.[15]
Thyroid Surgery
Thyroidectomy, such as partial or total thyroidectomy, is one of the most common surgeries performed worldwide.[19] Thyroid surgery is usually indicated in compression symptoms, malignancy, a solitary cold nodule of the thyroid gland in patients of age less than 20 years, cosmetic reasons or a cyst with more than 4 cm in diameter.[20] Hemithyroidectomy is performed for different indications like compression symptoms secondary to unilateral thyroid lobe enlargement, as in benign pathology, cosmetic reasons and indeterminant pathology on fine needle aspiration cytology.[20] Since postoperative hypoparathyroidism is often treated aggressively, it is linked to several risk factors, including extensive bilateral thyroid surgical operations, central neck dissection, retrosternal goitre, autoimmune thyroid disease, inexperienced surgeon(s), revision thyroid surgeries, and malignancy.[21] Transient or permanent hypocalcaemia is one of the complications following total thyroidectomy, which is rarely found following hemithyroidectomy. Neck dissection for thyroid malignancy and Graves’ disease increases the chance of post-thyroidectomy hypocalcaemia.[22] Both short-term and long-term hypocalcaemia are frequently linked to total thyroidectomy with central neck dissection.[23] More extensive neck dissection, along with thyroid surgery, has a higher risk of hypocalcaemia.[24] Furthermore, compared to total thyroidectomy, partial thyroidectomy has been linked to a decreased risk of hypoparathyroidism.[24] Patients with Graves’ disease are at risk for thyrotoxic osteodystrophy and impaired parathyroid gland visibility due to prolonged inflammation of the thyroid tissue.[1]
Role of Parathyroid Glands
There has been debate in the literature over the significance of identifying parathyroid glands in preventing hypocalcaemia. In order to prevent hypocalcaemia, one study recommended that at least three parathyroid glands be identified.[1] There was no correlation between the number of parathyroids discovered and another investigation.[5] According to a study, identifying the parathyroid glands is not a protective measure and may actually raise the risk of hypocalcaemia, which is likely caused by either direct trauma or surgically disrupting the blood flow.[5] Failure to release or produce PTH, a reduced bone response to this hormone, bone resistance to vitamin D, enhanced calcitonin action, or a major change in the solubility, growth rate, or dissolution of bone crystals could all be the cause of this condition.[25]
Postoperative Serum Calcium
There are various causes for postoperative hypocalcaemia, such as surgical technique, iatrogenic parathyroid injury, extent of thyroidectomy, malignancy, gender, preoperative serum calcium levels, PTH levels, thyroiditis, presence of hypothyroidism, and diabetes.[1,26] Patients undergoing completion thyroidectomy seem to be less prone to develop hypocalcaemia as a result of any iatrogenic effects on the parathyroid glands at the first operation being reversed before the second surgery. Identification and, therefore, exposure of parathyroids during surgery may have an adverse effect on the blood supply to the glands, affecting their function.[5]
Clinical Presentations of Postthyroidectomy Hypocalcaemia
The severity and sharpness of the onset determine the clinical manifestations of hypocalcaemia. The initial neurological symptom of acute hypocalcaemia is paraesthesia in the hands, feet, and perioral area. If left untreated, this condition can escalate to cramps, hyperreflexia, and muscle spasms. There may be associated with irritability, depression, and psychotic symptoms. In extreme conditions, a shift in contractility or cardiac electrical conduction may result in syncope, angina pectoris, or congestive heart failure. These patients may also present with epileptic crisis, laryngospasm, and bronchospasm, which compromise the patient’s life.[18] When the facial nerve is tapped at the angle of the jaw (the masseter muscle), Chvostek’s sign is elicited by seeing the contraction of the ipsilateral side of the face (the lip or nose). When a blood pressure cuff is placed on the arm and inflated to 10 mm Hg above the systolic pressure for at least two minutes, the brachial artery becomes obstructed, causing spasms in the hand and forearm, called Trousseau’s sign. Despite this, prolonged hypocalcaemia can cause serious side effects include intracerebral haemorrhages, calcification of the basal ganglia, subcapsular cataracts, papilledema, and Parkinsonism.[13]
Management of Low Serum Calcium Levels
The postoperative transient hypocalcaemia is often corrected by contralateral normal functioning parathyroid glands. Serial calcium measurements are typically taken after surgery to identify hypocalcaemia, which typically necessitates a minimum of 48 hours in the hospital. Clinicians often practice to measure serum calcium preoperatively, 6 hours post-operatively and 24 hours postoperatively. After a thyroidectomy, some patients might not experience hypocalcaemia for four days.[27] Patients who are at risk may be identified by routine intraoperative PTH tests.[5] Patients at risk of hypocalcaemia can be identified by tracking the rate of change in serum calcium during the first 24 hours after thyroid surgery.[5] Reimplantation of the parathyroid gland fragments into the sternocleidomastoid muscle is the recommended intraoperative treatment for a devascularised parathyroid gland.[18] In order to reduce the incidence of symptomatic hypocalcaemia after total thyroidectomy, prophylactic use of calcium and vitamin D is advised if the preoperative vitamin D level is less than 15 ng/ml. This is because the risk of hypocalcaemia following surgery increased 15 times if the level was less than 15 ng/ml.[28]
Prognosis
Post-thyroidectomy hypocalcaemia is usually transient, but it can take several months to go away.[29] The more frequent type, such as a temporary/transient one, usually goes away in a few days or weeks after thyroid surgery. Although the cut-off time between a temporary and permanent hypocalcaemia varies between six months and a year, hypocalcaemia persists past this point and stays permanent in 0%–12% of instances.[29] When the parathyroid glands are inadvertently removed, a permanent hypocalcaemia frequently results.[5] The severity of low serum calcium following thyroid surgery has reduced as parathyroid-preserving techniques have improved over the years.[5]
Conclusion
When carried out by a skilled surgeon, thyroid surgery is a safe surgical procedure with few problems. Longer hospital stays and increased expenses could result from these issues. Hypocalcaemia is the most frequent complication following thyroidectomy. Patients who undergo a total thyroidectomy are prone to experiencing hypocalcaemia after the procedure. It lowers quality of life and mortality risk while lengthening hospital stays and raising expenses. Early diagnosis by assessing the predictive factors can prevent hypocalcaemia.
Footnotes
Acknowledgements
The acknowledgements for this review are extended to those who have previously contributed to and conducted research on the same topic. This recognition acknowledges the existing body of work and the collective efforts of researchers in the field. The author expresses gratitude to those who contributed to the development and execution of this research, acknowledging their invaluable support and collaboration.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval from an Institutional Ethical Committee was not applicable for this article, as it is a review article compiled from various research studies and does not involve direct patient data or interventions.
Credit author statement
SKS: Conceptualisation, Methodology, Writing-review and editing, Supervision, and draft.
Data availability
Not applicable.
Informed consent
Not applicable.
Use of artificial intelligence
No use of AI.