
Abstract
Introduction:
Self-regulated learning (SRL) is a useful concept to facilitate learning among medical students at the individual level so that they become lifelong learners. This study was planned to examine the SRL practices of year 1 and 2 medical students during the COVID-19 pandemic and correlations with their motivations to join medicine and their future career preferences.
Methods:
The study was conducted between January and April 2022. Modified Motivated Strategies for Learning Questionnaire instrument and an in-house validated and published questionnaire to assess motivation to study medicine and career preference were administered online after written informed consent. The challenges perceived and measures taken by students during remote learning were collected by open-ended questions. Pearson correlations between factor scores and an independent samples t-test to compare mean factor scores were done in SPSS v21. Content analysis of qualitative responses was done.
Results:
88 out of the 200 eligible students participated. Positive significant correlations were found between the factors related to SRL and positive factors related to motivation to study medicine (Pearson’s r > 0.3 and P < .001) but not to negative motivational factors. Similar associations were observed for factors related to specialty preference as well.
Introduction
The success of the competency-based medical education (CBME) curriculum for undergraduate medical students introduced from the academic year 2019–2020 onwards in our country is dependent on ensuring that they employ self-directed learning (SDL) practices.[1] SDL is introduced with the goal of making medical students transform into lifelong learners.[2] SDL is described as a process in adult learning where the initiative comes from the learners on what to learn.[3] A related but theoretically distinct concept to SDL is self-regulated learning (SRL).[4] While SDL focuses on how an individual, through their choices of learning, influences the external environment, SRL focuses on the reflection of the learner to achieve mastery or competence in a subject.[5,6] Although both SDL and SRL are used interchangeably in the literature, there are distinct differences, and they are derived from different theoretical perspectives.[7] SRL is a concept which focuses on how to learn to achieve mastery or competence in a subject. Both the concepts of SDL and SRL, developed around the 1960s and 1970s, are influential in educating the learners. While SDL is instrumental in bringing the learners to institutions of learning, SRL is focused on developing learners into competent professionals.[8,9]
SRL is based on the integrated and recursive role of (meta)cognition, emotion, and motivation in the learning process.[10] A self-regulated process involves a preparation and planning phase, an execution phase, and a self-reflection phase where the learner adjusts plans for the future.[11] Application of SRL principles in the field of education has been on the rise in the past two decades. However, its role in higher education contexts and among medical students has not been studied adequately. In the context of medical education, motivation to join medicine and clear goals on their future specialty preferences are essential aspects that are directly related to SRL. The relationships between these aspects have not been investigated so far.
SRL is mainly addressed in classroom contexts and in children and adolescents. The focus of SRL on medical education has been recent, and there are a handful of studies which have focused on SRL.[12,13] These studies have shown that the learners differ in their SRL practices, and those with efficient SRL have been shown to perform well academically.[14,15] The onset of the COVID pandemic forced the medical students to engage in online classes while the teachers and their peers were remotely connected.[16] In this context, the importance of SRL and related practices was studied and was found to be of use to cope as well as improve academic performance.[17]
Our study was mainly driven by the need to explore the learning processes of medical students in the pre-clinical phases (years 1 and 2 of the MBBS course) by means of assessing SRL practices and then to explore the association between SRL constructs and their motivations to study medicine and future career preferences. It was done during the COVID pandemic as students were in remote locations. It provided a natural setting for us to investigate SRL practices in our students to see how they cope with online and remote learning with minimal feedback provided by peers, seniors, and teachers that they would have obtained if there had been no pandemic. Hence, we obtained information on the challenges perceived by the medical students during online and remote learning and the ways in which they coped with this situation. We explored the association of SRL, which is critical to facilitate learning at an individual level, with motivation and career preference among year 1 and 2 medical students. We hypothesised that there would be a positive association between factors related to SRL and motivations to study medicine and their future career preferences.[18] Theoretical frameworks used in the study were social-cognitive theory (SRL is based on it), which would require students to use SRL practices and expectancy-value theory, as the efforts taken would be related to their motivations and career aspirations.[19]
Our aim was to analyse the factors of SRL among year 1 and 2 undergraduate medical students using a validated questionnaire and then explore their associations with motivation to study medicine and their future career preferences. We chose the first- and second-year medical students mainly because these students usually require more input from their teachers due to high cognitive load. The main objectives of the study were to assess the correlation of factors of SRL with those of motivation to study medicine and career choice, and secondarily to identify the challenges faced during remote learning and the measures used to overcome them during the COVID pandemic.
Methods
Study Participants
Medical students admitted in Christian Medical College Vellore, during the academic year 2019–2020 and 2020–2021, who were in the first and second year of the MBBS course, respectively, for whom the new competency-based curriculum was implemented, were the study participants. The study participants were recruited voluntarily and were enrolled on the study only after obtaining written consent, which was administered online on the Microsoft Teams platform along with the questionnaires. No sample size calculation was done for this study. The total number of eligible students was 200.
Study Instruments
Two questionnaires were used in this study. One of the questionnaires to study the factors associated with motivations to study medicine and specialty preference was standardised in our setting and published elsewhere.[20,21] Students were asked to rate lists of items pertaining to the motivations to study medicine and specialty preference on a Likert scale of 1–5 (where 1 = not important, 2 = slightly important, 3 = moderately important, 4 = important and 5 = very important) in the questionnaire, which was designed in-house in our previous studies.
MSLQ (Motivated Strategies for Learning Questionnaire) is one of the standard instruments used in published literature to assess SRL.[22] We used the modified MSLQ instrument, which has been adopted from Soemantri et al. (2018), to assess SRL in medical students.[23] The response process of this questionnaire was tested in about 10 medical/paramedical students who were not included in the study, to ensure that the questionnaire can be used in our medical students. The items related to SRL were rated by the study participants on a scale of 1–7 (where 1 = not at all true of me, 7 = very true of me), as per the information provided in the study conducted by Soemantri et al. (2018).[23] Ratings of items for a given factor were added to and divided by the number of items to obtain the mean factor scores. Mean and standardised scores of each factor were used for correlational analyses. Demographic data and all other data were extracted from the study questionnaires used in this study. The main demographic variables collected were gender, place of birth and family members as doctors.
Data Collection
Data collection was done between January and April 2022. At least three reminders were sent by email to participate in the study, as the students were not present in the institution due to the COVID pandemic. Those who did not complete the questionnaires or failed to submit the responses after the reminders were considered as not willing to participate in the study and hence were not pursued further. Questionnaires were administered online on Microsoft Forms to the study participants. Written informed consent which was set as a required field for participation in the study. Both the modified MSLQ instrument (Soemantri et al., 2018) and the other in-house validated questionnaires to assess motivation and career preference published previously were administered online. A link to participate in the study was created and was sent through the Microsoft Teams app to all the eligible study participants. After collecting the data from the participants, anonymisation was done by allocating unique participant codes for analysis purposes.
Study Variables and Validation of Factor Scores
Factor scores of subscales related to SRL, motivation to study medicine, and preference for specialty were calculated as published in the literature for the respective questionnaires. Four factors extracted from MSLQ were SRL_SO (self-orientation), SRL_FS (feedback seeking), SRL_CT (critical thinking), and SRL_SR (self-regulation) (Soemantri et al., 2018).[23] Four factors related to motivation to study medicine were MMPersGro (personal growth), MMProfCal (professional calling), MMPersCon (personal concerns), and MMProfCon (professional concerns) as described elsewhere.[20] The factors related to specialty preference were SCPersGro (personal growth), SCProfGro (professional growth), and SCPersSat (personal satisfaction).[21] The internal consistency reliability of the factor scores was assessed by the values of Cronbach’s α. Two open-ended questions on challenges faced by students during remote learning and the measures taken to overcome them were added as additional items. Verbatim comments were analysed for their contents.
Statistical Analysis
Independent samples t-tests were done to compare the mean factor scores between different sub-groups of students based on demographic variables. Pearson correlations between mean factor scores were done to assess the association between SRL and motivation to study medicine and specialty preference factors. A P value of <.05 was considered statistically significant for this study. All analyses were done in SPSS v21. Content analysis of qualitative responses was done separately.
Results
Characteristics of Study Participants
The total number of students who participated in the study was 88 (response rate 44%), out of which 35 were from year 1 and 53 were from year 2 of the MBBS course. The mean age of the participants was 20 ± 1.2 years. Forty-seven study participants were females, 78 were from an urban background, and 46 had at least one doctor in their close family.
Mean Factor Scores of Study Participants
Mean factor scores were calculated from the filled-in questionnaires and are provided for all the subscales on SRL, motivation to study medicine, and specialty preference [Table 1]. The factor scores showed good internal consistency (Cronbach’s α ranged from 0.6 to 0.8). No significant differences were found between the mean factor scores for the four subscales related to SRL across the different sub-groups of students based on MBBS phase of study, gender, geographical background, and presence/absence of doctors in the family (data not shown).
Overall mean factor scores of study participants (n = 88)
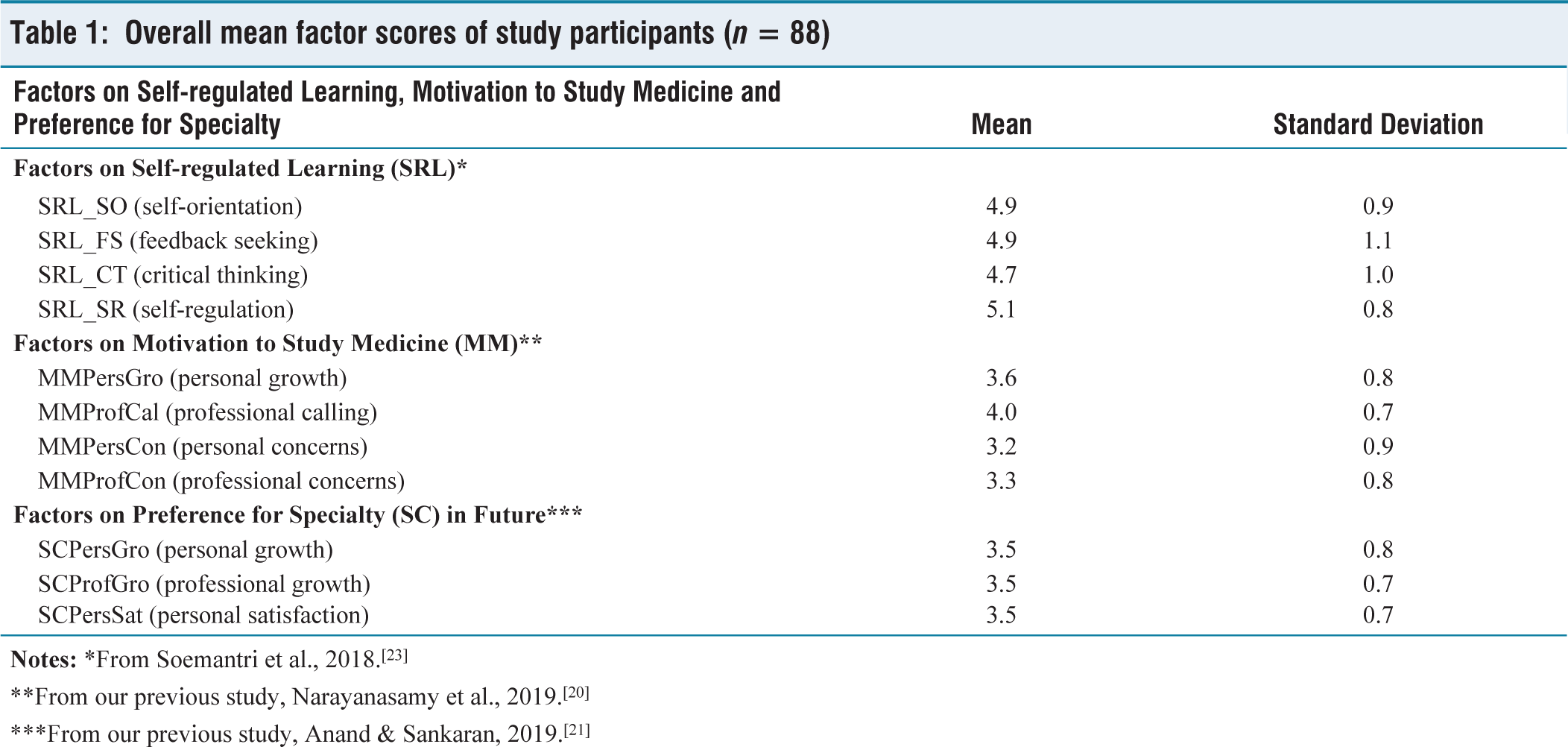
**From our previous study, Narayanasamy et al., 2019.[20]
***From our previous study, Anand & Sankaran, 2019.[21]
Correlation Between Self-regulation and Motivation
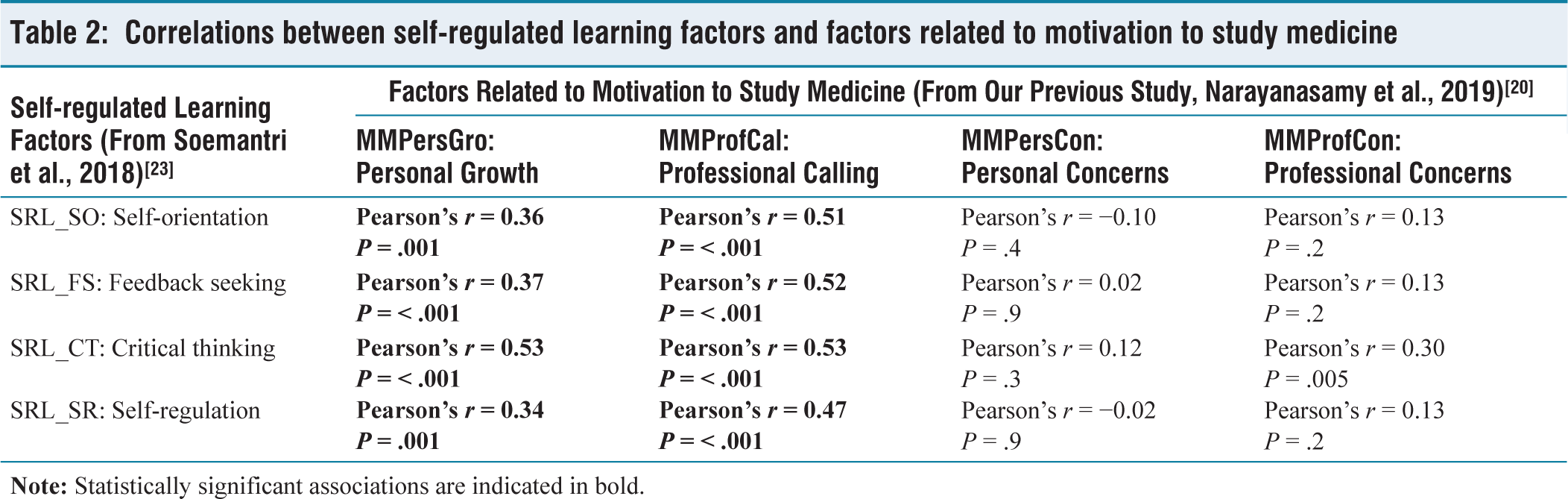
We first analysed the association between the factors related to SRL and motivation to join medicine [Table 2]. All four factors of SRL were positively and significantly correlated with the two positive motivational factors to join medicine, namely MMPersGro and MMProfCal. Factors related to motivational concerns to join medicine, however, were not correlated to factors of SRL with one exception. The motivational factor related to professional concerns, MMProfCon, was positively associated with the SRL factor on critical thinking (SRL_CT). This may probably imply that the critical thinking component of SRL, an essential element in medical education, especially in today’s digital and artificial intelligence era, might pose a genuine concern for the learners as they progress through the training. This is an element which must be addressed by the educators and teachers of medical education involved in training future doctors.
Correlations between self-regulated learning factors and factors related to motivation to study medicine
Correlation Between Self-regulation and Specialty Preference
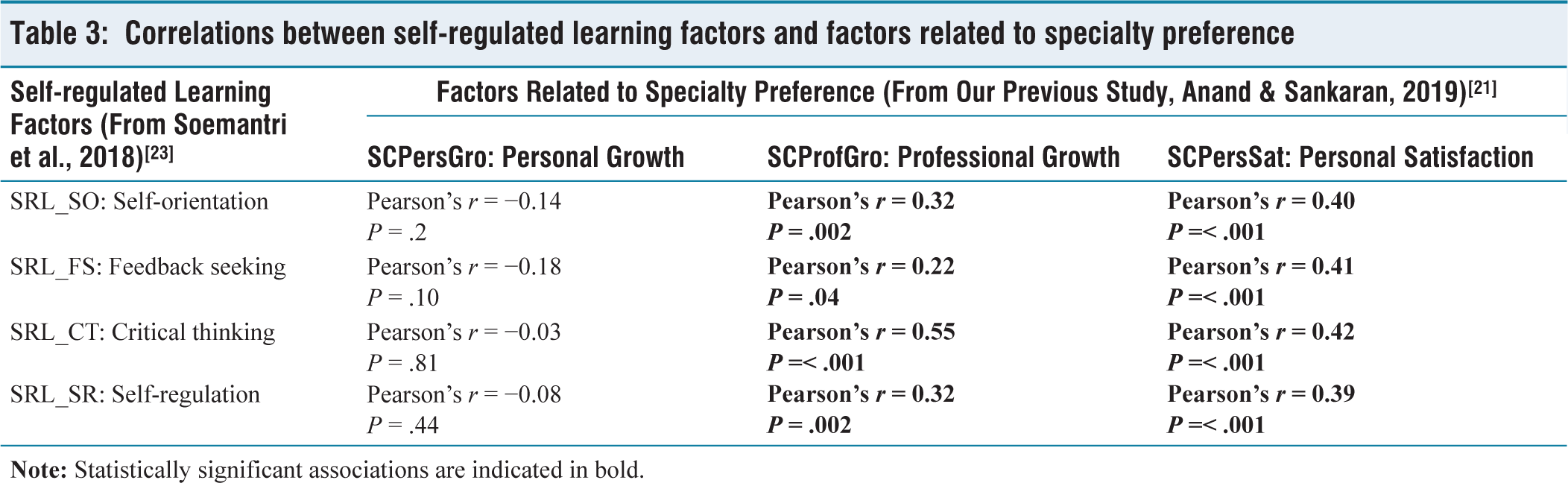
We then analysed the association of SRL factors with those related to specialty preference in our students [Table 3]. Specialty preference factors related to professional growth (SCProfGro) and personal satisfaction (SCPersSat) but not personal growth (SCPersGro) were positively and significantly associated with all four SRL factors. It is likely that when it comes to specialty preference, SRL is more likely to contribute towards career growth in their preferred specialty and probably lead to personal satisfaction as well. However, SRL may not play any specific role towards the personal growth that accompanies the medical students as they progress from undergraduate to postgraduate degrees.
Correlations between self-regulated learning factors and factors related to specialty preference
Challenges Faced and Measures Taken During Remote Learning
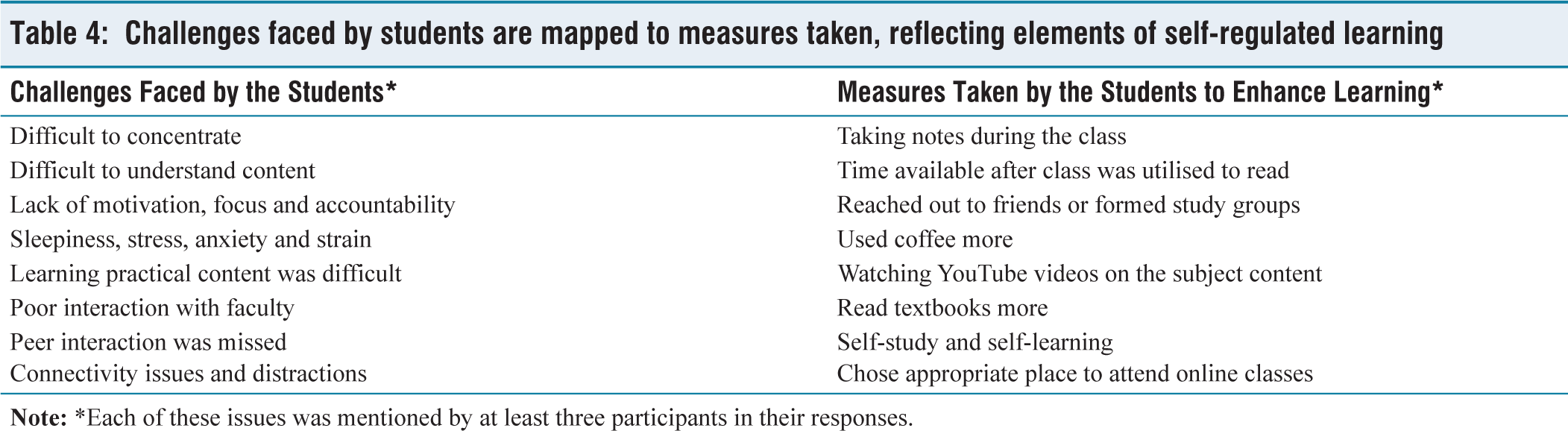
Next, we analysed the responses of the study participants on the challenges experienced by them during the online classes imposed by the COVID pandemic. It provided us with an opportunity to identify whether the students took measures that align with the concepts of SRL, as the usual support systems in terms of their peers, teachers, classrooms, laboratories, and library were unavailable to them. We found that many of the issues reported by students during this part of the training were managed by various measures taken by the students themselves that match the behaviours derived from the concept of SRL [Table 4]. Factors related to SRL, such as self-orientation and self-regulation, were evident from the measures taken by students on how they managed their available extra time by doing self-study. In addition, feedback seeking element of SRL was evident when they tackled the lack of motivation by forming study groups.
Challenges faced by students are mapped to measures taken, reflecting elements of self-regulated learning
Discussion
The new curriculum for undergraduate medical education in our country, introduced in 2019, lays emphasis on learner-centred delivery of medical education. However, its implementation was impacted by the COVID pandemic that soon followed that year. It affected the routine academic activities and reduced student support due to the lack of traditional learning environments provided by the institution. Students had to remain in their homes and attend all classes in an online environment. In this study, we utilised this natural opportunity to study the association between SRL factors and motivations to join medicine and their future career preferences.
We found some interesting positive associations between the factors related to SRL and those related to positive motivational factors to join medicine, and the factors related to specialty preference, especially with respect to professional growth and personal satisfaction. Our analyses on how the students coped with the various challenges imposed by the online learning environments due to the COVID pandemic provided us insights as to how aspects of SRL are relevant, especially when the learners need to take more responsibility in their learning during an undergraduate medical degree. It is especially important during the initial years of medical training, when many of the basic science subjects are learnt. Promoting SRL practices in the initial years of medical training can be promoted by motivating the learners.
Studies around the world show that in many settings, the move towards online learning environments due to the COVID pandemic forced the learners to employ SRL practices.[24–26] Employment of SRL was found to be useful for learners to overcome academic challenges, and in some cases was associated with improved academic performance as well.[27,28] Some of the challenges which could not be overcome with online learning, even with SRL practices, were the ability to achieve mastery and to employ critical thinking.[29,30] We also found similar results where the critical thinking factor of SRL correlated with the professional concerns motivation factor [Table 2].
SDL, self-efficacy and SRL are essential to professional identity formation and future career choices of medical students. In our settings, medical students join the course at a younger age compared to Western countries and often at the behest of influence from others. In this context, it is essential that medical students understand their role as future medical professionals. Although the roles of the teachers and facilitators are crucial in imparting knowledge in the initial years of medical training, it is important that the medical students self-regulate their learning processes as well.
The internal control and processes that regulate learning are captured by the concept of SRL. It was not clear how the different aspects of SRL were among the medical students in our context. Learning among medical students can be influenced by several aspects such as the motivation level of the students, learning environments, context of learning, teaching-learning practices, quality of assessments and so on.[31] Among the various learning theories, social-cognitive theory, from which SRL is derived, places emphasis on the fact that learning is not merely individualistic but a social phenomenon.[32] In that context, expectancy-value theory can be a useful framework to assess the learning processes and their associations with motivations and future career preferences, as they are all related to the expectations of the learner, and the value society places on medical students as they become doctors. In agreement with this, we found in this study that the factors related to SRL were positively associated with both the positive motivations to join medicine [Table 2] and their preference for a specialty in the future [Table 3].
The onset of the COVID pandemic forced the learners to engage online with the teachers, and the traditional way of assessing students had come to a halt. Medical students were forced to adopt remote and distant learning. It is critical that both teachers and students need to embrace the concepts of SRL. The results obtained in this study emphasised that the capacity to adopt SRL practices was observed with our students [Table 4], and this can be useful for the educators and administrators to plan the curriculum and teaching-learning methods that facilitate the incorporation of SRL and SDL to achieve the goal of making medical students to be life-long learners.
Our study had the following limitations. The response rate was low despite repeated reminders (at least 3) to students to participate. Hence, the relationships obtained in this study are likely to be underpowered and must be confirmed in larger samples. What is not addressed in this study are the metrics that help to evaluate SRL in online learning environments, as there have been no specific modules created for medical students. The sessions that are normally held in the traditional classrooms and laboratories have been moved to online platforms, and hence, the major changes were in the learning environment. Also not addressed in this study are the associations between SRL and academic performance, as the usual way of assessing the students in classroom written tests and practical assessments was not held owing to the pandemic situation. No specific topics or subjects were considered; instead, the practices in online classes overall were reflected upon to assess elements of SRL.
Conclusions
SRL factors were not significantly different with respect to the baseline characteristics of students. SRL factors were positively associated with motivation to study medicine, factors and specialty preference factors. Several measures taken by medical students during the online classes conducted during the COVID pandemic demonstrated elements of SRL to overcome the challenges they faced. Some of the implications of these findings could be to promote SRL in online learning programmes by motivating the learners.
Footnotes
Acknowledgements
We thank the study participants. We thank Dr Laxmi G, who was working in the Department of Pharmacology at our institution, for her input during the planning phases of the study. This educational research project was done as part of the Advanced Course in Medical Education of the National Medical Commission, conducted at the nodal centre for the National Faculty Development Programme at our institution.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The study proposal was approved by the Institutional Review Board (IRB Min. No. 14210 [OBSERVE], dated 25 August 2021).
Informed consent
Written informed consent was obtained online from all participants prior to their participation in the study.
Credit author statement
Prakash SS conceived the proposal, conducted the study, collected data, analysed and wrote the manuscript.
Data availability
All data pertaining to the manuscript are available in the manuscript.
Use of artificial intelligence
None to declare.