
Abstract
Introduction:
Central line-associated bloodstream infections (CLABSI) impose a significant financial burden on patients and hospitals. This study evaluates the impact of CLABSI on hospital revenue loss and explores recovery potential through bed backfilling in an Indian tertiary care setting.
Materials and Methods:
A mathematical simulation model using a static decision tree was developed using published data to assess the economic impact of CLABSI over a 1-year time horizon from a hospital perspective, assuming 80% occupancy. This study was conducted between January and October 2025 and estimated the revenue loss per CLABSI case and modelled scenarios for 25% and 50% CLABSI rate reductions and varying backfill ratios. One-way sensitivity analysis (OWSA) varied inputs by ±10% to test robustness. Input parameters included CLABSI incidence, central line utilisation ratio, length of stay (LOS) and revenue for matched CLABSI versus non-CLABSI cohorts.
Results:
Each CLABSI case resulted in an estimated revenue loss of ₹2,86,132 (0.38% of potential revenue), driven by lower average revenue per bed-day (ARPOB) for CLABSI patients (₹27,990) versus non-CLABSI patients (₹50,000). Reducing CLABSI rates by 25% and 50% decreased revenue loss to 0.28% and 0.19% of potential revenue, respectively. Backfilling at a 3.33:1 ratio offset all lost revenue, while a 1.67:1 ratio recovered half of the lost revenue.
Conclusions:
Preventing CLABSI can significantly reduce hospital revenue loss, improve financial sustainability and lower patient treatment costs by minimising prolonged stays and out-of-pocket expenses. This health system projection model underscores the importance of allocating accurate and continued funding for healthcare-associated infections (HAIs) reduction programmes.
Keywords
Introduction
Globally, millions of patients are affected by healthcare-associated infections (HAIs) each year. On average, about 1 in 10 patients develops an HAI.[1,2] The World Health Organisation estimates that HAIs have a lesser incidence in high-income countries and a higher incidence in low- and middle-income nations.[2-4] Central line-associated bloodstream infections (CLABSI) remain one of the most serious and preventable HAIs worldwide.[5] These infections not only compromise patient safety but also place a significant burden on healthcare systems.[5-8]
In India, the challenge is even more pronounced. A surveillance study across 54 tertiary hospitals under the International Nosocomial Infection Control Consortium reported a pooled CLABSI rate of 8.83 per 1,000 central line-days.[5] Alarmingly, mortality associated with these infections reached over 40% by the end of the surveillance period.[5] Factors such as poor hand hygiene, inadequate catheter care, antimicrobial resistance and limited access to advanced diagnostics all play a role in this concerning trend.[9,10]
Beyond the clinical impact, HAIs also carry a heavy economic toll.[11-16] Out-of-pocket expenditure (OOPE) accounted for 47.1% of India’s total health spending in 2019–2020, remaining a major financial burden despite a declining trend.[16] Studies have shown that HAIs can double treatment costs due to extended hospital stays.[12,17] A prospective study from a tertiary hospital in western India found that HAIs significantly increase treatment costs. Patients with HAIs incurred more than double the direct costs compared to non-HAI patients, primarily driven by prolonged intensive care unit (ICU) stays.[13] Another study on paediatric patients also reported that HAIs increased total costs by 3.6 times, with length of stay (LOS) being the primary driver.[18] Similarly, CLABSI substantially increases hospital resource utilisation and overall treatment costs, imposing a significant financial burden on patients through higher OOPE.[13,19] Overall, evidence from Indian studies over the past decade indicates a rising economic burden of hospital-acquired infections on patients.[13,14,17]
While patient-level costs are well studied, the financial impact on hospitals themselves is less understood, particularly in low- and middle-income countries. Hospitals face increased resource demands for infection control, including isolation protocols, enhanced cleaning and additional staffing.[10] In private tertiary care settings, where revenue depends on bed turnover and procedural volumes, prolonged stays due to CLABSIs can disrupt patient flow and reduce profitability.[20] Although HAI prevention programmes are cost-effective, many hospitals hesitate to invest in infection control programmes due to perceived high costs and a lack of localised data showing return on investment.[20–22]
Globally, some institutions have begun to quantify the financial benefits of preventing HAIs. For instance, a Stanford Hospital study reported that eliminating CLABSIs could boost hospital revenue annually per infection type avoided.[20,21] However, such data is scarce in the Indian context, where healthcare financing is complex and varies widely across public and private sectors.
We developed a health system projection model tailored for Indian hospitals to estimate revenue losses from CLABSIs. The study aims to quantify the economic impact of CLABSIs in a hypothetical Indian tertiary care setting and assess potential financial recovery.
Methods
Study Design and Setting
This health economic evaluation was conducted at the Department of Health Economics and Outcome Research, B. Braun Medical (India) Pvt Ltd and B. Braun Medical Industries, Pulau Pinang, Malaysia, from January 2025 to October 2025. This economic evaluation was conducted in a mathematically simulated 300-bed Indian tertiary care corporate hospital with an occupancy rate of 80%. This modelling study was based on disparate sources of evidence from published estimates from literature.
Input parameters were derived from peer-reviewed literature, Indian hospital financial reports and expert consultations to ensure contextual relevance. The static model avoided dynamic transitions, focusing on aggregated annual estimates to align with hospital budgeting cycles. No primary patient data were collected and ethical approval was not required due to the study’s hypothetical, modelling-based design.
Model Structure
This study conceptualised a static decision tree model in Microsoft Excel. The decision tree comprised two arms: One calculating revenue in the absence of CLABSIs (non-CLABSI arm) and the other accounting for revenue with CLABSI incidences (CLABSI arm). This structure enabled the quantification of revenue losses directly attributable to CLABSIs. The non-CLABSI arm calculated revenue using standard bed occupancy, LOS and average revenue per bed-day (ARPOB) for non-CLABSI patients. The CLABSI arm adjusted for extended LOS, variable revenue per bed-day due to complications and lost bed turnover opportunities.
The model incorporated several key components to estimate the impact of CLABSIs. Central line utilisation was calculated by estimating total central line-days using hospital bed capacity, occupancy rate and central line utilisation ratio. CLABSI incidence was modelled as events per 1,000 central line-days, directly influencing LOS and revenue. Revenue was calculated by multiplying occupied bed-days by revenue per bed-day, differentiated by CLABSI status.
A backfilling mechanism was included to simulate revenue recovery by applying a backfill ratio representing additional patient admissions to offset extended bed-days from CLABSI cases.
Perspective
The study adopted a health system perspective, focusing on ARPOB in CLABSI and non-CLABSI patients. This perspective was selected to provide insights relevant to hospital budgetary considerations, particularly in private tertiary care settings where revenue is tied to bed turnover and procedural volumes.
Time Horizon
The model’s time horizon for the base case was 1 year. The 1-year time horizon eliminated the need for discounting, as all costs and revenues were contemporary.
Input Parameters
Parameters were sourced from both Indian and international literature and validated against local data. Average revenue per regular non-CLABSI patient was taken as ₹150,000, based on industry estimates for corporate hospitals in India. For CLABSI patients, revenue was calculated by adding the base revenue of ₹150,000 to the inflated CLABSI management cost of ₹213,868 (Chacko 2017, adjusted at 3% inflation till 2025),[17] resulting in ₹363,868 per-patient.
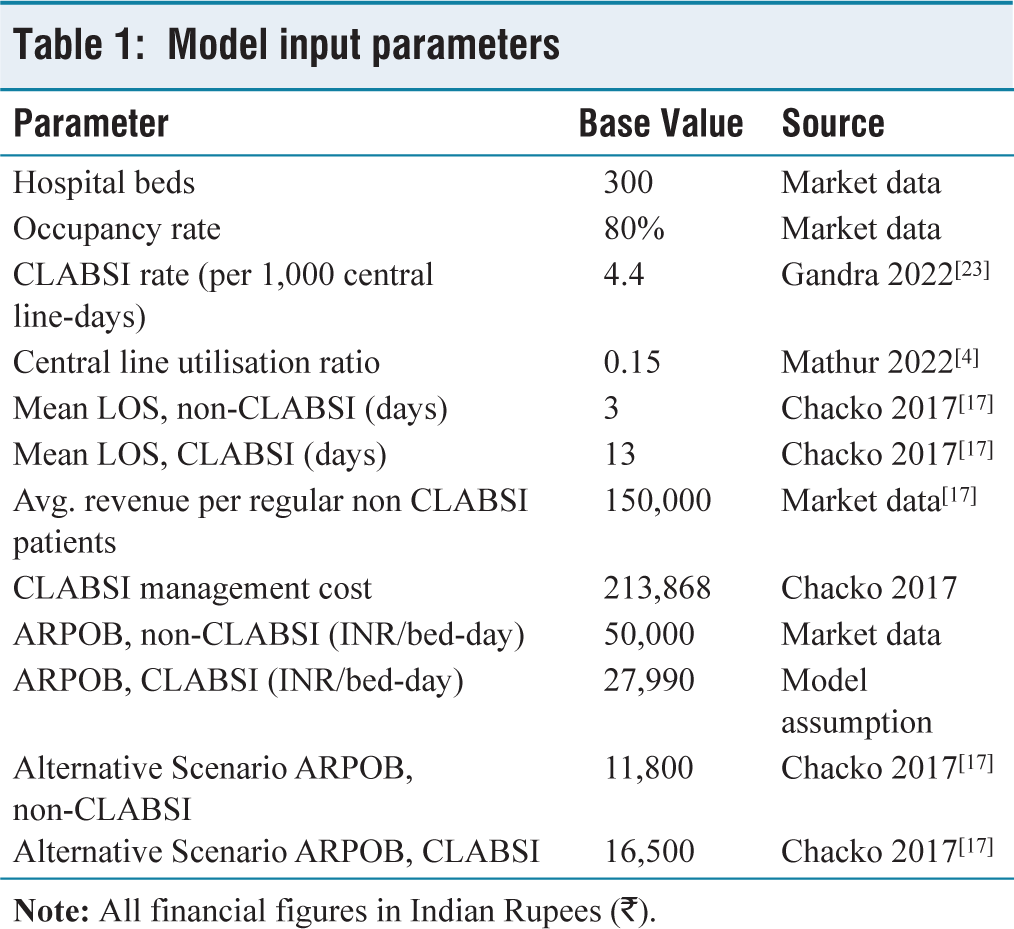
Revenue per bed-day was then derived by dividing total revenue per-patient by the respective LOS. For regular non-CLABSI patients, this amounted to ₹150,000 divided by 3 days, yielding ₹50,000 per bed-day. For CLABSI patients, ₹363,868 was divided by 13 days, resulting in ₹27,990 per bed-day. These values were used to compute ARPOB for both patient categories within the model [Table 1].
Model input parameters
Analyses
The primary outcome was revenue loss (or gain) attributable to CLABSIs, calculated as the difference in total revenue between non-CLABSI and CLABSI arms and as a percentage of potential revenue (i.e., revenue if all beds were used by non-CLABSI patients). All analyses were performed using Microsoft Excel.
Scenario Analyses
Two key scenario analyses were conducted to assess the impact of CLABSI rate reductions and backfill strategies. In the first scenario, CLABSI rate reductions were modelled at two levels: A 25% reduction, which resulted in an incidence of 3.3 per 1,000 central line-days and a 50% reduction, which lowered the rate to 2.2 per 1,000 central line-days.
The second scenario explored backfill strategies, incorporating four different backfill rates: 0%, 25%, 50% and 100%. These rates represented the proportion of additional non-CLABSI patient admissions per prevented CLABSI case, quantified using a backfill ratio.
An alternative scenario (non-surgical medical ICU) was modelled to enhance generalisability, where we considered higher per-bed-day revenue in CLABSI due to intensive resource use, such as costly antibiotics and prolonged ICU billing, based on Indian ICU cohorts excluding surgical, haematological or chronic liver disease patients.[17]
Sensitivity Analyses
Sensitivity analyses were performed using one-way approaches. The one-way sensitivity analysis (OWSA) involved a ±10% variation in each model input to evaluate the robustness of outcomes.
Results
Base Case Analysis
The decision tree model analysed a hypothetical 300-bed tertiary care hospital in India operating at 80% occupancy over 1 year, resulting in 87,600 occupied bed-days. With a central line utilisation ratio of 0.15, this translates to 13,140 central line-days. At a baseline CLABSI incidence rate of 4.4 per 1,000 central line-days, the model estimated approximately 58 CLABSI cases annually. These infections accounted for 751.6 bed-days, as each CLABSI patient had an average LOS of 13 days, compared to 3 days for non-CLABSI patients.
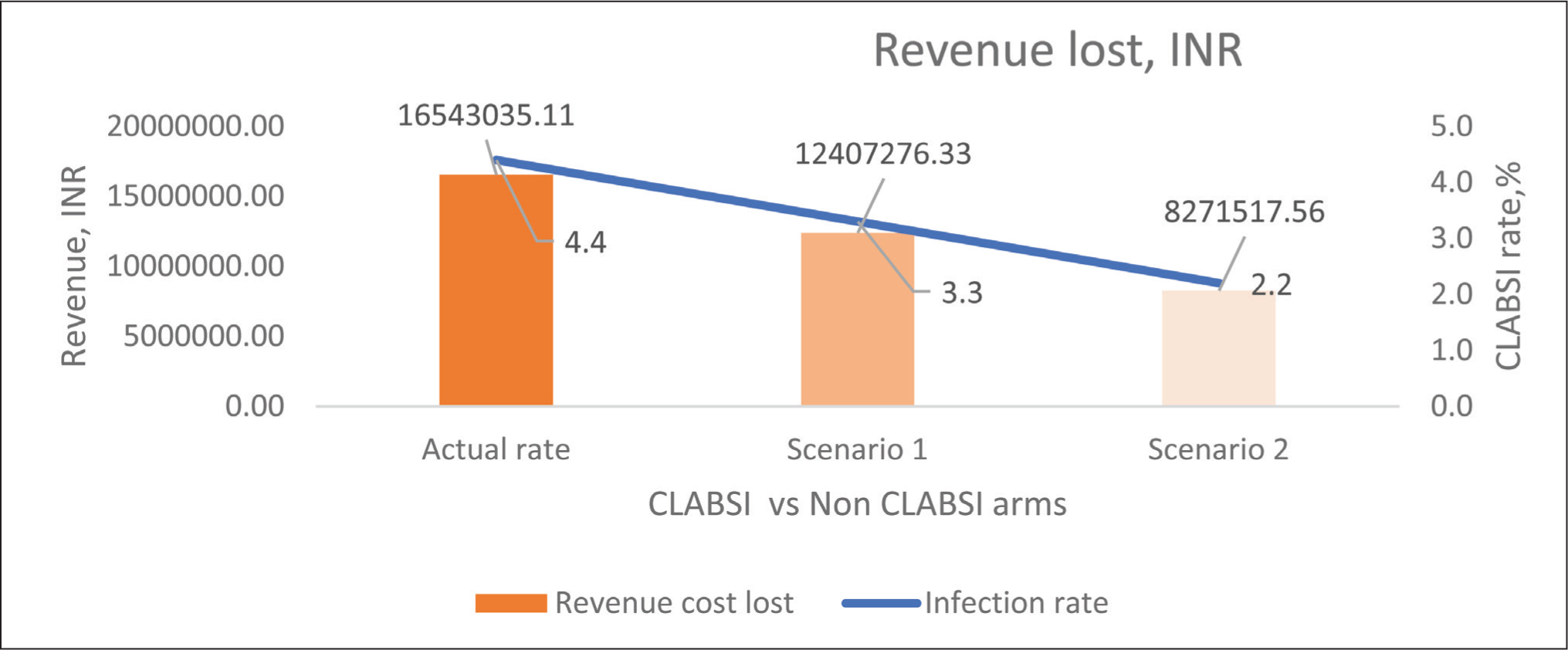
The difference yielded a revenue loss attributable to CLABSIs of ₹16,543,035, equivalent to 0.38% of the potential revenue in a CLABSI-free scenario. This loss was primarily driven by the reduced effective revenue per bed-day for CLABSI cases and the opportunity cost of extended bed occupancy, which limited admissions of additional non-CLABSI patients. On a per-case basis, each CLABSI resulted in an estimated revenue loss of ₹286,132 [Figure 1].
Scenario Analyses
Two projected scenarios evaluated the financial impact of reducing the CLABSI rate through prevention programmes. In Scenario 1, a 25% reduction in the CLABSI rate led to a reduced loss of ₹12,407,276 (0.28% of potential revenue). This represented savings of ₹4,135,759 compared to the base case, highlighting the proportional benefit of rate reductions.
In Scenario 2, a 50% reduction (to 2.2 per 1,000 central line-days) further lowered CLABSI cases with a loss of ₹8,271,518 (0.19% of potential revenue). Savings relative to the base case were ₹8,271,517, demonstrating that halving the CLABSI rate could nearly halve the associated revenue loss.
These scenarios assume full backfilling of freed bed-days with new non-CLABSI patients to maintain occupancy, reflecting an optimistic but achievable outcome in demand-constrained settings [Figure 1].
Revenue loss due to CLABSIs
Backfilling Scenarios
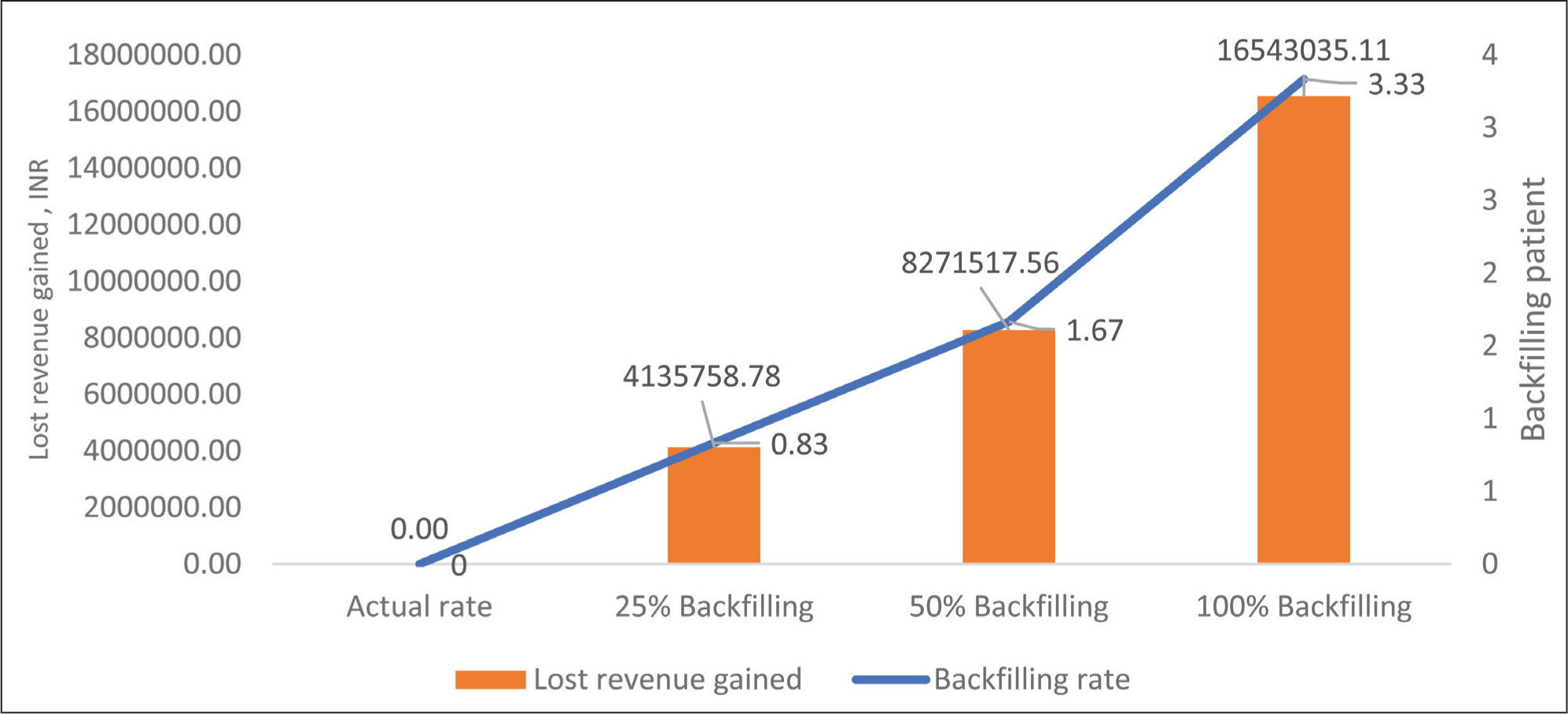
Preventing CLABSI released an average of around 10 bed-days per-case, which can be used for new admissions. If fully backfilled (3.33 new patients per-case), turning the total loss of ₹16.5 million into a full recovery across 58 cases.
At 50% backfill (1.67:1), recovering about 8.3 million of the loss. At 25% backfill, recovering about 4.1 million of the loss [Figure 2].
Lost revenue gained with backfilling after CLABSI prevention
One-way Sensitivity Analysis
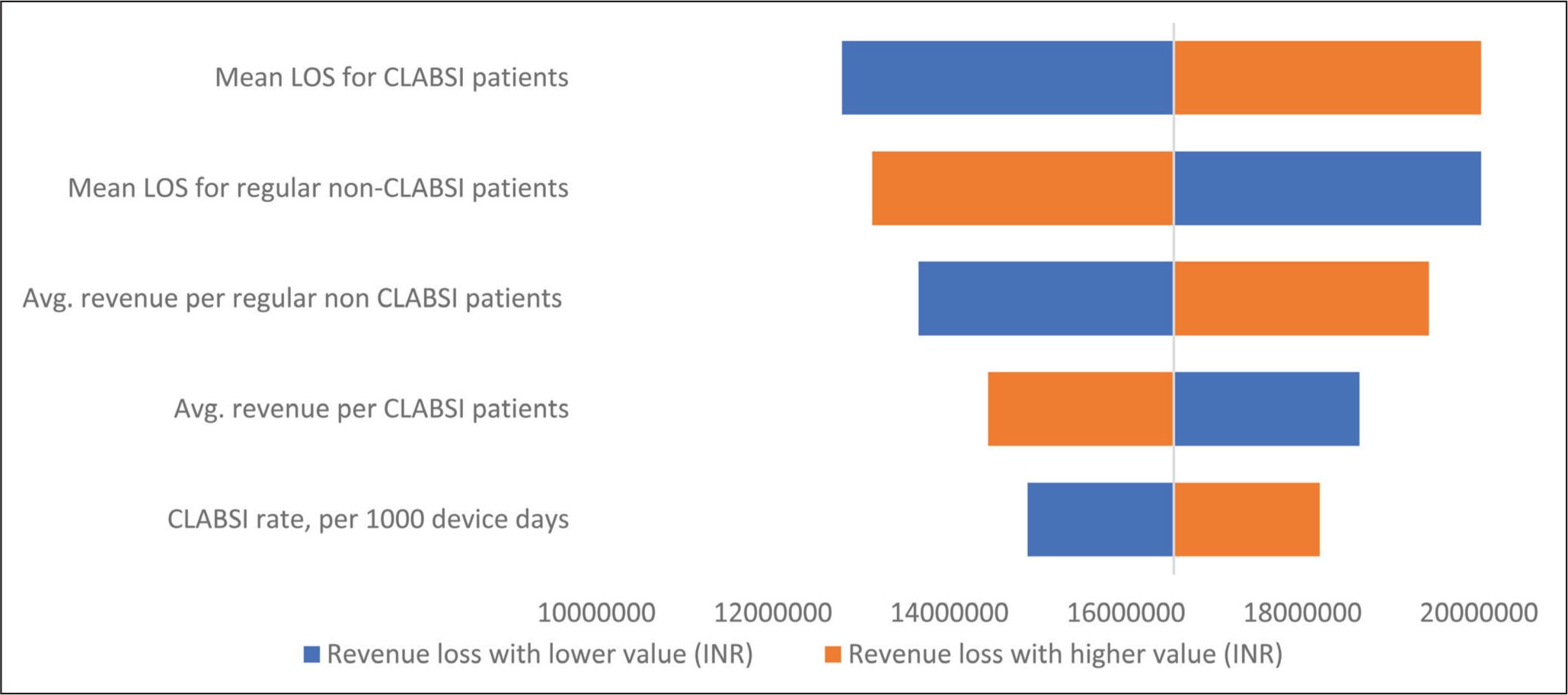
The OWSA evaluated the major input parameters in the model [Figure 3]. The tornado diagram illustrates the univariate sensitivity analysis of revenue loss between the CLABSI and non CLABSI scenario. Bar width reflects potential estimate variation, keeping other variables constant. The highest impact is attributed to the mean LOS for CLABSI patients, followed by the mean LOS for regular non-CLABSI patients, average revenue per regular non-CLABSI patient and average revenue per CLABSI patient. The CLABSI rate per 1,000 device days shows the smallest impact, as evidenced by its lower position and narrower bar [Figure 3].
Alternative Financial Impact in Non-surgical Settings
In purely medical ICUs, excluding surgical, haematological or chronic liver disease patients, the ARPOB is approximately ₹13,022 for HAI patients and ₹9,279 for non-HAI patients.[17]
This data indicates that CLABSI can increase per-bed-day revenue by around 40%, primarily due to the intensive use of costly antibiotics, diagnostics and prolonged billing for critical care services.
This results in a net revenue gain of about ₹14 million or 1.73% above the potential revenue in the non-CLABSI scenario. On a per-case basis, this equates to a gain of approximately ₹243,240 for each CLABSI case.
Tornado diagram of one-way sensitivity analysis (OWSA) showing the impact of different variables on the revenue loss, comparing the different rates of CLABSI
Discussion
The relationship between HAIs and hospital economics is complex. HAIs play a key role in readmission rates, influencing both financial metrics and overall hospital profitability.[22,24],25]] Even though hospitals recognise that reducing HAIs is critical for patient safety, investing in prevention programmes is often perceived as an additional financial burden.[20,21],25]] Many hospitals hesitate to invest in infection control initiatives due to perceived high costs and the lack of localised data demonstrating return on investment.[20–22]] To support these programmes, hospital administrators need robust economic data to strike a balance between revenue generation and strategic investment aimed at improving performance.
The current study attempted to evaluate the economic impact of HAIs in an Indian tertiary care setting and help demonstrate the financial ramifications associated with CLABSI. This study highlights the potential for substantial cost savings associated with reducing CLABSI rates in Indian tertiary care hospitals. By preventing CLABSI, hospitals can mitigate revenue losses, as demonstrated through our health economic model.
Many previous studies have failed to demonstrate the expected cost savings, even when HAI rates decline substantially.[26,27]] A growing body of evidence now challenges the traditional paradigm. Economic analyses, including detailed studies using Stanford Hospital data, have shown that successfully eliminating HAIs and increasing bed turnover can unexpectedly increase total hospital costs while simultaneously raising hospital contribution margin and profits. In fact, these studies found that while hospitals incur additional expenses to reduce HAIs, profits increase even more because higher revenue offsets these costs.[20,21]] Current study findings based on a hypothetical Indian hospital strongly support this counterintuitive yet increasingly well-documented and statistically analysed trend.
The underlying reason in the Indian context is driven by revenue per occupied bed-day, which is widely recognised as an important measure of a hospital’s financial performance and quality indicator.[28,29]] A typical hospital stay generally consists of two phases. The initial phase, often the first 1–2 days, tends to generate most of the revenue as major tests, procedures and treatments are carried out. This is followed by a maintenance phase, where revenue contribution becomes comparatively lower.[28] When CLABSI occurs after the initial phase, the patient’s stay is extended mainly in this low-revenue phase. Although treating CLABSI adds some costs, it does not generate incremental additional revenue for hospitals. This reduces the hospital’s ARPOB and overall profitability.
From the patient’s perspective, HAIs, particularly CLABSIs, substantially increase overall treatment expenses due to prolonged hospitalisation and additional care requirements.[11–18] By preventing HAIs and reducing unnecessary extended stays, hospitals can lower overall treatment costs for patients, minimise out-of-pocket expenses and improve access to timely care.[20,21] Preventing CLABSI shortens the LOS and releases beds for new admissions, which can help hospitals recover lost revenue. Better bed utilisation and resource optimisation ultimately benefit patients.[20] Therefore, if the hospital can backfill the bed, it could generate additional net revenue by admitting new patients. Efficient turnover ensures that resources are allocated to patients who need acute interventions rather than prolonged maintenance, enhancing both financial sustainability and better patient outcomes.[20,21] Further, if the hospital is unable to admit a new patient to occupy the vacated bed, the resulting revenue loss typically triggers adjustments in staffing, resource allocation and overall bed capacity.[20]
In the present study, the base model calculates a lower ARPOB for CLABSI cases compared to non-CLABSI cases, which is particularly relevant for mixed or procedure-heavy hospitals where infections delay high-turnover surgical cases.[20,21] In these clinical settings, the difference between the high-revenue phase and the low-revenue maintenance phase is significant, so prolonged stays due to CLABSI reduce overall revenue. However, in non-surgical medical ICU settings, these phases are less distinct because care remains intensive throughout the stay. CLABSI in such units often leads to higher ARPOB due to prolonged critical care and the use of costly antibiotics and diagnostics.[17] This means that in non-surgical ICUs, CLABSI may increase revenue per bed-day, highlighting that the financial impact of CLABSI is also dependent on case mix and care setting.[17] Another important point regarding ARPOB is that when annual occupancy is low, revenue per occupied bed-day becomes less significant.[28]
Sensitivity testing indicates that revenue loss is driven more by variations in LOS and per-patient revenue than by changes in CLABSI rates. These findings highlight the need for accurate data on LOS and revenue metrics to strengthen model reliability, while reinforcing the case for investing in CLABSI prevention to recover revenue through shorter stays and bed backfilling. The findings of the present investigation are similar to previous studies from other geographies.[20,21,30,31]
This analysis has certain limitations. First, ARPOB was estimated based on conceptual assumptions and did not account for factors such as case mix variability or payer differences due to the multi-payer status of the Indian healthcare system. Second, we were unable to calculate profitability due to the absence of detailed hospital cost data. Access to comprehensive cost datasets would enable more robust testing of the model and provide a better understanding of the economic implications of CLABSI on a hospital’s financial metrics.
Conclusion
Reducing HAI is not only crucial for patient safety but also offers significant financial benefits for hospitals. Effective implementation of HAI prevention strategies can lead to substantial cost savings and increased revenue, making it a profitable investment for healthcare institutions. Beyond hospital economics, these interventions directly benefit patients by lowering overall treatment costs, reducing OOPE and improving access to timely care. This study reinforces the need for continued and accurate funding of HAI prevention programmes as a strategic priority that aligns hospital profitability with patient-centric care. Future research should integrate detailed cost and occupancy data to refine these models and guide policy decisions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Not applicable.
Informed consent
Not applicable.
Credit author statement
PG, RA, AA: Study conception or design of the work, data collection, data analysis and interpretation, drafting the article, critical revision of the article and final approval of the version to be published and accountability for all aspects of the work.
Data availability
Data from the hypothetical cohort model will be made available upon reasonable request from Dr Akhil Agarwal.
Use of artificial intelligence
None.