
Abstract
Background. Ethanol lock therapy (ELT) with systemic antimicrobial therapy is a promising therapy for catheter-related infection (CRI). The impact of ELT timing on treatment efficacy and costs is unknown. Procedures. A prospective study was conducted in the Hematology/Oncology Unit at the Children’s Hospital of Michigan. Patients with suspected CRI were randomized to Preemptive ELT arm or Rescue ELT arm after positive culture. Results. Five cases in Preemptive arm and 9 in Rescue arm had a confirmed CRI. All cases cleared infection with line salvage with no adverse events due to ELT or recurrence within 14 days. Our data showed a trend toward 36% reduction in average hospital costs and 40% reduction in average length of stay in Preemptive arm over Rescue arm. Conclusion. Although a small study, our data on preemptive ELT with systemic antimicrobial therapy suggest a potentially important treatment strategy in reducing length of stay as well as hospital costs.
Keywords
Introduction
Central catheters deliver various therapies to pediatric hematology, oncology, and bone marrow/hematopoetic stem cell transplant (H/O/HSCT) patients. A known complication is catheter-related infection (CRI), and the risk increases after only 7 days from catheter placement.1,2 In pediatric patients, central catheter use has increased to lessen both recurrent peripheral catheter placement and the pain associated with repetitive needle sticks despite the risk of infection. 3 The traditional recommended CRI treatment paradigm is catheter removal (for some organisms) with concomitant systemic antimicrobial therapy. 3 However, repeated replacement of central catheters should be avoided in pediatric patients because of the additional costs associated with replacement, the requirement for anesthesia, possible therapy delays, and limited vascular access sites. 2
Ethanol lock therapy (ELT) along with systemic antimicrobial therapy, is a promising therapy that has been used both to prevent,2,10-17 and treat CRI.4-9 Recently, daily ELT has been used in treatment of pediatric CRI for fungal infections and in a pediatric CRI salvage protocol.10,11 The benefit of ELT has been reviewed broadly 18 and specifically in H/O/HSCT patients. 19 Questions remain with regard to which specific treatment strategies utilizing adjunct ELT for CRI are the most effective and safe among pediatric H/O/HSCT patients.
In prior work, we retrospectively reviewed H/O/HSCT patients admitted to Children’s Hospital of Michigan (CHM) for CRI, and our data suggested a trend that ELT in combination with systemic antimicrobials had a higher salvage rate for infected catheters over antimicrobials alone. 20 Additionally, patients with earlier ELT (after 1 positive culture vs after persistent positive cultures) had a significantly (P = .018) shorter hospital length of stay (LOS) and attributable length of stay (ALOS) (P = .022), which was defined as time from admission to first negative culture. These findings formed the foundation for the present study. 20 In this study, we hypothesized that short-dwell preemptive ELT placed within 24 to 36 hours of admission (arm 1) versus ELT placement at time of first positive culture (arm 2) along with systemic antibiotics for CRI treatment in the pediatric H/O/HSCT population would result in shorter hospital LOS and lower hospital costs. A single-center, randomized trial was carried out in a pediatric H/O/HSCT unit at CHM over a 2-year period to test this hypothesis.
Methods
Research Design
ELT with concomitant systemic antimicrobials has become an accepted local standard of care (SOC) since 2007 for the treatment of CRI in hemodynamically stable patients in the H/O/HSCT unit where catheter salvage is desired.14-17,20 In this study, the research team compared hospital LOS, ALOS, and hospital costs of study participants in 2 study arms utilizing short-dwell ELT (4- to 24-hour dwell times per day, per lumen) at varying timing. The broad range of dwell times accommodated some patients with multiple concurrent infusion needs with limited intravenous access. Suspected CRI cases randomized to arm 1 received preemptive ELT (placed by 24-36 hours of admission) before any blood cultures were reported, while cases randomized to arm 2 received rescue-ELT at the time of first positive cultures. For clinical equipoise, ELT was provided in both arms in conjunction with systemic antibiotics for the treatment of CRI (suspected or proven) and only the timing of ELT was varied. Concomitant antimicrobial therapy was prescribed to all participants by treating clinicians and administered by oncology nursing staff. Our ELT protocol was described in more detail in a previously published work 14 (see the appendix).
All study participants were patients at CHM, a tertiary care pediatric hospital in Detroit, Michigan, from June 2014 to June 2016. Rate of clearance (sterilization) of the infected catheters after ELT and catheter salvage along with catheter reinfection with the same pathogen within 28 days from first ELT were assessed. Adverse events (AEs) after ELT were followed and CRI episodes meeting National Healthcare Safety Network (NHSN) criteria for laboratory-confirmed bloodstream infection (LCBSI) were recorded. 21
Inclusion Criteria
All patients (<21 years of age) with central catheters that developed clinical symptoms and were admitted with an underlying H/O/HSCT diagnosis for suspected CRI of the blood, including “rule out” sepsis, were screened and potentially enrolled for participation if further inclusion criteria were met. Clinical symptoms of suspected CRI included fever, chills, leukocytosis, hypotension, and tachycardia that were not suggestive of alternate or recent (prior) source of infection. Additionally, participants were required to have had their initial clinical blood cultures obtained from central (mandatory) and peripheral blood (as possible) on admission and be able to be enrolled within 24 to 36 hours of admission. Individual CRI cases in the same patient were defined as distinct CRI if separated by >28 days from prior ETL and/or caused by different organism(s) than that of prior CRI episode. Patients meeting all enrollment criteria were offered participation and completed informed consent.
Exclusion Criteria
Any child with ethanol allergy, blood cultures positive for growth within 12 hours, endovascular infection (including infective endocarditis, septic cardiac thrombus), or symptoms requiring immediate line removal were excluded.
Treatment Randomization
Enrolled participants were assigned to a treatment arm per randomization lists provided by the study biostatistician. Randomization procedure was stratified by immunocompromised state (Yes/No) 20 and a randomization list for each of the 2 groups (immune-compromised Yes/No) was generated with a 1:1 allocation ratio.
Specific ELT Protocol: Arm 1 (Preemptive ELT)
Participants in arm 1 had study ELT placed within 24 to 36 hours of admission into their central catheters per protocol (described above) for 4- to 24-hour dwell times per lumen per study day. On completion of study ELT dwell, the ethanol was flushed and repeat study central cultures were obtained, per lumen. A blood culture was obtained 48 hours after flush of study ELT (to document sterility with 2 negative cultures). If blood cultures from admission and post-ELT were negative for growth, no second blood culture was obtained. In such cases, the participant was deemed “not infected” and was continued in safety and reinfection follow-up.
Specific ELT Protocol: Arm 2 (Rescue ELT; Local SOC)
Participants enrolled in arm 2 had SOC ELT placed at the time of positive blood culture report, per ELT protocol (as above) for 4- to 24-hour dwell times per lumen per day. On completion of ELT dwell, the ethanol was flushed and clinically indicated, SOC repeat central cultures were obtained. A second study blood culture was obtained 48 hours post-ELT flush to confirm sterility.
Data Collection
All catheter data were recorded from interventional radiology and surgical records. Patient demographics, medical histories, clinical signs and symptoms, medications, LOS, ALOS, and laboratory results were prospectively collected from medical records. Costs data were collected from the CHM financial database.
Participant Safety
A Data Safety and Monitoring Board (DSMB) composed of 4 physicians periodically reviewed study progress. AEs were defined as any untoward occurrence in a participant administered ELT for up to 28 days post-ELT. The study coordinator followed up with the participants after receipt of ELT to assess for any possible side effects. The Wayne State University Human Investigation Committee approved this study and it was registered on clinicaltrials.gov: NCT02095951.
Study Definitions
Hospital LOS was defined as the number of hours between time of admission and discharge. ALOS was defined as the number of hours between time of admission and time of first negative blood culture, and was only available for cases with positive central blood culture. “Clearance” of the infected catheter was defined by negative blood culture(s) obtained from the infected central catheter 24 to 72 hours after ELT. “Failure to clear” was defined by persistent positive blood culture(s) obtained from the central catheter 24 to 72 hours after ELT with no other identified focus.
A catheter was considered a “salvage” if there was initial clearance (as above) followed by repeat negative central cultures for at least 14 days from ELT. A catheter was considered a “nonsalvage” if there was “failure to clear” (as above) and ≥1 positive cultures obtained >72 hours after ELT with no other identified focus of infection. Infection “recurrence” was defined as catheter reinfection with the same pathogen within 28 days of the initial ELT enrollment.
A central catheter was defined as any permanent or semipermanent foreign body inserted into the patients’ vasculature, including medi-ports (port), Broviac lines, and peripherally inserted central catheter (PICC) lines.
Detailed and Specific Analytical Approach, Statistical Analysis
The primary endpoints were LOS, ALOS, and hospital costs. Only facility-based costs were captured in this study utilizing the Detroit Medical Center (DMC) cost-accounting system. Secondary endpoints included infection clearance rate, catheter salvage rate, catheter reinfection rate within 28 days of ELT, and incidence of AEs. To compare ALOS, LOS, and hospital costs between the 2 study arms, 2-sample t tests as well as Wilcoxon rank sum tests were used. To compare the rate of catheter infection clearance and central line salvage, Fisher’s exact tests were used. SAS version 9.3 was used for analysis.
Results
A total of 135 cases were referred for screening. Of these, 54 did not meet enrollment criteria, 33 had refusal of informed consent/assent, and 12 had no parent available to give consent or had a language barrier to prevent understanding of informed consent. Of the 54 subjects not meeting enrollment criteria; 1 was not an actual H/O/HSCT patient, 3 required immediate line removal, 7 were beyond 36 hours of admission at time of referral, 8 had a blood culture that grew in <12 hours, 15 had alternate identified sources of fever, and 20 patients were on therapy for a prior infection. All participants were enrolled based on clinical symptoms and blood cultures drawn at time of hospital admission.
Thirty-six distinct cases of fever with central line presentadmitted to rule out sepsis that met all study inclusion/exclusion criteria were enrolled in the study which represented 30 distinct patients. One hypotensive case was subsequently withdrawn due to the need for continued intravenous fluids via a single lumen central catheter and no clinically feasible way to allow for minimum ELT dwell time. Two additional enrolled cases were excluded due to lack of positive central catheter blood culture or developing alternate infection source. This left us with 33 evaluable CRI (or suspected CRI) cases in 27 distinct patients for analysis. Six participants were enrolled twice for separate CRI evaluations which occurred >28 days apart from their initial episode.
Of the 33 evaluable cases, 15 were enrolled in arm 1 and 18 in arm 2. Mean age at enrollment was 7.5 years (range: 0.8 months to 18 years) with 22 (81%) being male.
Fourteen out the 33 cases resulted in a positive blood culture; 5 (33%) in arm 1 and 9 (50%) in arm 2. All 14 confirmed CRI cases were treated with pathogen appropriate systemic antimicrobials along with 1 ELT (per lumen), and had at least 2 negative follow-up blood cultures post-ELT. In addition, all 14 cases achieved clearance of central catheter infections and line salvage. None had recurrence of infection within 28 days after ELT, but 1 case did have new polymicrobial infection 30 days post–initial ELT with 1 of the same pathogens as the initial episode. There were 7 cases that met NHSN LCBSI criteria 1 and 3 cases that met criteria 2. 21 Four cases did not meet LCBSI criteria but were treated with antimicrobial therapy by treating clinician. Table 1 summarizes the characteristics of the14 cases with positive blood cultures.
Characteristics of 14 Confirmed CRI Cases.
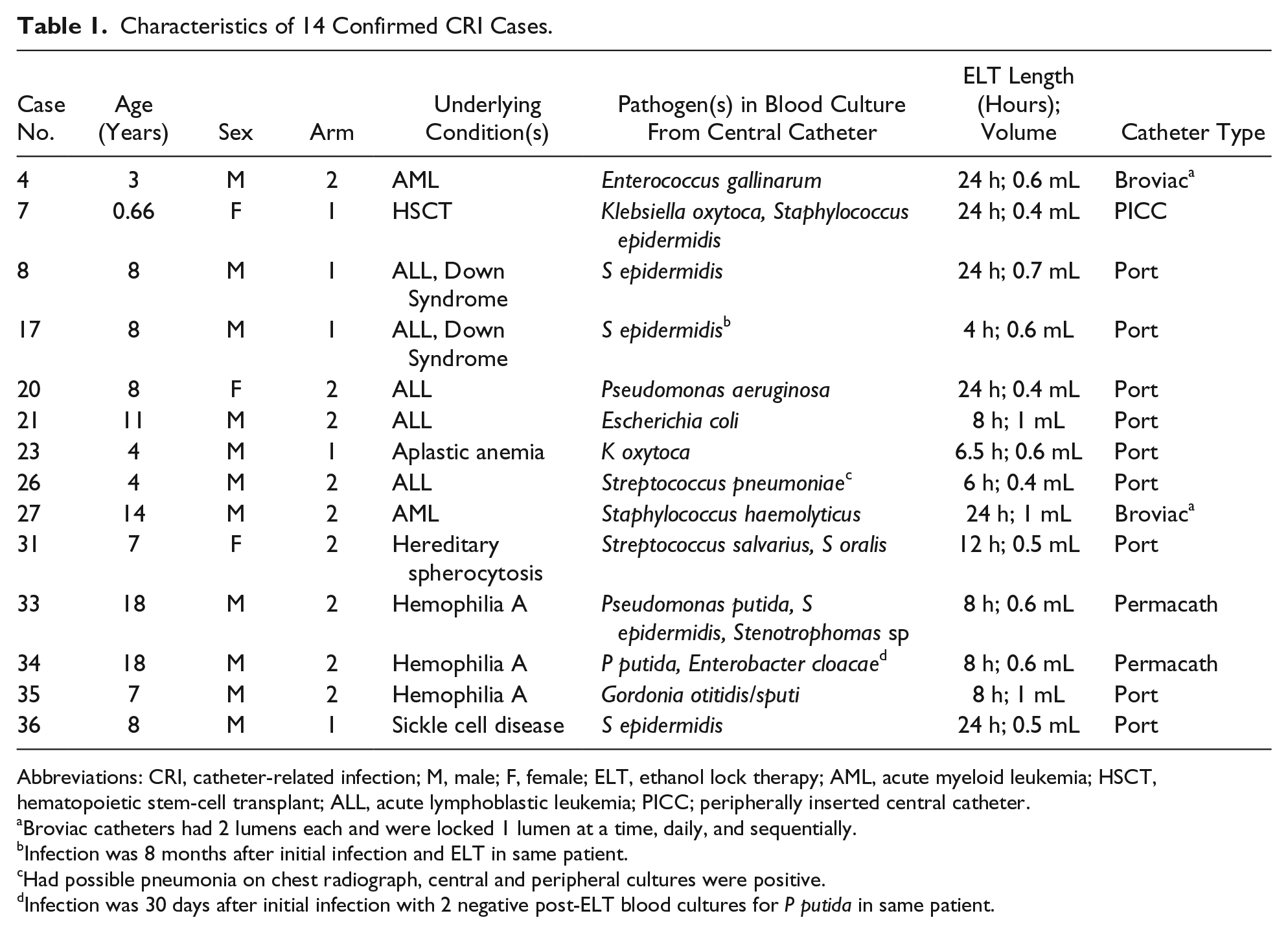
Abbreviations: CRI, catheter-related infection; M, male; F, female; ELT, ethanol lock therapy; AML, acute myeloid leukemia; HSCT, hematopoietic stem-cell transplant; ALL, acute lymphoblastic leukemia; PICC; peripherally inserted central catheter.
Broviac catheters had 2 lumens each and were locked 1 lumen at a time, daily, and sequentially.
Infection was 8 months after initial infection and ELT in same patient.
Had possible pneumonia on chest radiograph, central and peripheral cultures were positive.
Infection was 30 days after initial infection with 2 negative post-ELT blood cultures for P putida in same patient.
Intent-to-treat analysis of the 33 evaluable cases (n = 33) showed a reduction of 45% in mean hospital LOS and 58% in mean hospital costs in arm 1 as compared with arm 2 (see Table 2). A more clinically relevant analysis on the 14 confirmed CRI cases also showed a reduction of 40% in mean LOS, 34% in mean ALOS as well as 37% lower mean hospital costs in Arm 1 (see Table 3).
Hospital Costs, Charges, LOS, and ALOS in 33 Evaluable Cases.

Abbreviations: LOS, length of stay; ALOS, attributable length of stay.
Hospital Costs, Charges, LOS, and ALOS in 14 Confirmed CRI Cases.
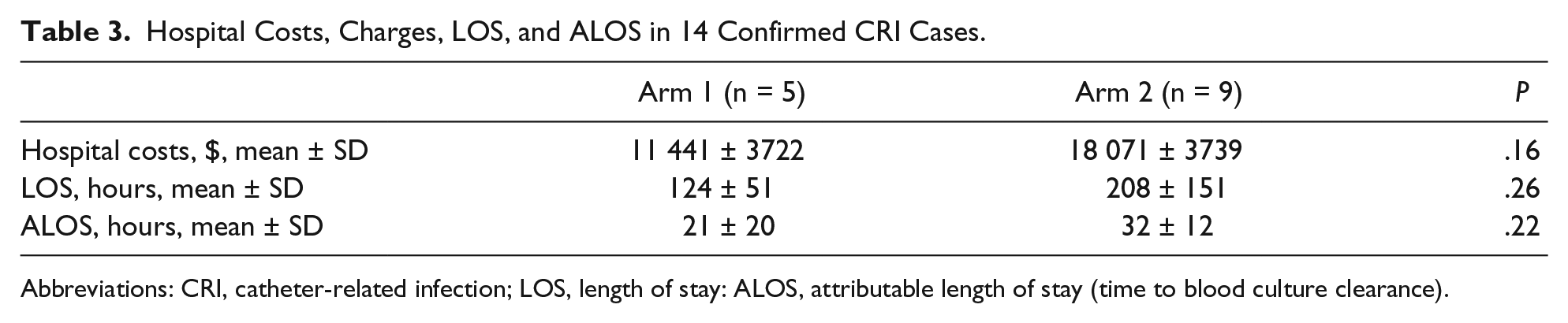
Abbreviations: CRI, catheter-related infection; LOS, length of stay: ALOS, attributable length of stay (time to blood culture clearance).
All 14 confirmed CRI cases resulted in catheter salvage per protocol definitions, but 3 cases did go on to have catheter removal and/or replacement beyond 14 days after initial CRI clearance. The patient for both case 33 and case 34 (arm 2) had a repeated polymicrobial infection 30 days after the initial episode with positive central culture growth for 2 pathogens (Enterobacter cloacae and Pseudomonas putida) and then his permacath removed 44 days after initial infection by same-day surgery with total cost of $1709. He had had 2 negative follow-up cultures after his initial episode. The subject for case 4 (arm 2) had his Broviac removed with total cost of $23 425 in an 11-day admission 18 days after his initial episode due to “frequent infections” and new infection with Bacillus cereus. Finally, the subject for case 36 (arm 1) had port removal and PICC line insertion 48 hours later with total cost of $19 028 during an 8-day admission for new CRI with Pseudomonas aeruginosa, 30 days after the initial episode.
The average dose of ELT given for CRI episode was 0.6 mL, per lumen locked. There were no significant AEs recorded during the study period related to ELT. Four of the analyzed cases with CRI had liver enzymes (alanine transaminase [ALT], aspartate transaminase [AST]) assessed clinically post-ELT which were normal in 2 cases, and in the other 2 cases both had similarly elevated ALT and AST before and after ELT. Two study cases in arm 1 received ELT without CRI and had ALT and AST assessed clinically after ELT; one of these had normal values and the other had similarly elevated abnormal pre- and post-ELT ALT and AST values.
Of the 2 enrolled but excluded cases without positive central line cultures, one had urosepsis due to Escherichia coli in the peripheral blood and urine culture, and the other case had only one peripheral blood culture positive for Ganulicatella adiacens.
Discussion
Our study evaluated the use and timing of ELT as adjunct therapy with systemic antimicrobial therapy in pediatric H/O/HSCT patients with suspected CRI. Because of difficulties in enrolling patients and the resulting small sample size, we were unable to establish statistical significance even though the observed savings in costs and reduction in LOS from a simple and inexpensive preemptive ELT intervention was clinically important. Preemptive ELT recipients in arm 1 had an 11 hours shorter mean ALOS (time from admission to first negative blood culture) than that of rescue ELT recipients in arm 2. The mean hospital costs in arm 1 was nearly half of that in arm 2. Both of these findings suggest a potentially important cost-benefit to earlier ELT initiation in H/O/HSCT patients with a suspected CRI. Most clinicians begin formal discharge plans for patients with CRI from the date of the first negative blood culture as many patients complete antimicrobial therapy at home. Additionally, a shorter hospital LOS for H/O/HSCT pediatric patients could lead to improved quality of life.
Each year in the United States approximately 80 000 CRI cases of the bloodstream occur in intensive care units. 22 ELT in pediatric hematology/oncology patients was recently reviewed by Wolf et al. 19 In that review, central line–associated bloodstream infection (CLABSI) rates were 1.6 to 2.8 episodes per 1000-catheters days (approximately 1 episode/patient in 16 months).23,24 Catheter removal occurs in 13% to 46% of CLABSI episodes.23,25,26 Patients with CLABSI required an additional average of 12 hospital days, which may delay chemotherapy.3,27 The cost of treating pediatric CLABSI has been reported to be from $39 219 to $46 133, per episode.28-30 Any novel treatment approach for pediatric CLABSI, including adjunct ELT, that is safe, inexpensive, and effective could yield significant health care savings as ELT is safe and reportedly costs only $16.00 per lock. 15
Based on current literature, ELT as adjunct therapy with systemic antimicrobials for pediatric H/O/HSCT CRI is not yet the national standard of care. However, clinical equipoise made having a true control group seem unethical based on prior experience.14-17,20 Therefore, although the authors agree that a large, multicenter randomized control trial of ELT for CRI is needed to prove a definitive benefit of ELT with antimicrobials over antimicrobials alone, we designed our trial such that all participants received ELT after 12 hours but varied the time to ELT initiation in arm 1 compared with arm 2, as detailed above.
Biofilms are organized microorganisms that adhere to living and non-living environmental surfaces, such as catheters, and secrete an extracellular substance matrix, firmly attaching them to the catheter.31,32 Formation of biofilms on intravascular devices is universal and occurs with Gram-positive, Gram-negative and fungal organisms. 31 It is theorized that, in CRI, the biofilm mass reaches a critical point and embolizes leading to clinical bacteremia and systemic symptoms.31,32 Antibiotic lock therapy, with concurrent systemic antimicrobials has been used in the treatment of CRI and the salvage of the catheter. Success rates of this process vary from 67% to 83%.3,33,34 With ELT use along with systemic antimicrobials, blood culture sterilization, and catheter salvage may be possible without mandatory catheter removal. The rate of catheter sterilization with catheter salvage in recent published pediatric studies utilizing ELT varies between 77% and 100%.11,15,35,36 In the present study, all subjects in both treatment arms with CRI achieved clearance and catheter salvage. However, 1 participant episode (No. 4) had CRI with a new pathogen 18 days out and later had catheter removal.
Exposure to 70% ethanol and water has killing activity against organisms in biofilms that include Gram-positive, Gram-negative and Candida spp. in 2 hours. 5 Biofilm eradication has been shown at various concentrations of ethanol alone or in combination with other agents with a wide microbial killing spectrum.5,37,38 Peters et al 38 reported treatment with 30% ethanol for minimum of 4 hours was inhibitory on monomicrobial and polymicrobial biofilms. In addition, incubation with at least 50% ethanol for 4 hours killed and inhibited Candida albicans and Staphylococcus aureus growth. 38 Furthermore, prolonged ethanol exposure to polyurethane and silicone did not significantly alter catheter integrity. 39 Time dependent elution of the polycarbonate diol component from carbothane dialysis catheters and some structural catheter changes were observed with ethanol exposures varying from 95% to 40% with more significant changes noted at the highest ethanol concentration. 40 In another study, no significant differences were found in silicone and carbothane hemodialysis catheters after 70% ethanol exposure for 26 weeks. 41
Our protocol was relative ethanol-sparing with only one ELT dwell given per lumen. Some studies used daily ELT during the treatment of CRI—typically a 10- to 14-day course.10,11,42 Additionally, small volumes of ethanol and water were used in our study with an average of 0.6 mL. A pilot study highlighted the safety of ethanol locks in small infants. 43 Short-dwell ELT use with small volume ethanol exposure to the catheter for no more than 24 to 72 hours likely has the smallest possible impact on catheter integrity and patient safety and the largest impact on CRI clearance and salvage rate over systemic antimicrobials alone. No specific AEs related to ELT were recorded during this study. No liver enzyme elevation was found in clinically assessed ALT and AST values in any patient that did not have similarly elevated ALT and AST elevations prior to ELT. Despite several articles raising concern for thrombus after ELT,19,44-46 no participants in our study had a catheter thrombus.
The economic implications of this research could be huge if these study results could be replicated in larger, multicenter trials. The cost savings are potentially 2-fold. First, according to our previous study data, using rescue ELT in pediatric CRI in conjunction with systemic antimicrobials may shorten the LOS and ALOS. 20 Second, if preemptive ELT as compared with rescue ELT could reduce the need for central line removal and replacement and further reduce LOS, then the potential healthcare dollar savings could be even more significant. Additionally, as noted in both articles by Rajpurkar et al15,16 for patients with hemophilia with CRI of the bloodstream, any therapy such as ELT with concomitant systemic antimicrobials that leads to catheter salvage may subvert the need for clotting factor, in which case savings could approach thousands of dollars per patient.
Our study limitations include small sample size and lack of statistical power. Poor acceptance of study protocols and refusal of parental informed consent leading to poor enrollment in supportive care trials in pediatric H/O/HSCT patients has been highlighted recently. 47 Because of low enrollment and small sample size, no subset analysis could be performed for immunocompromised state. When poor acceptance of the study was initially noted in the first several months, all H/O/HSCT clinical faculty joined the study as co-investigators to assist with enrollment. Additionally, costs for the treatment of the CRI could not be completely separated from the costs associated with the underlying medical condition.
In conclusion, these study results suggest that when preemptive ELT is used with systemic antimicrobial therapy for treatment of CRI in pediatric H/O/HSCT patients, there may be a potentially important reduction in LOS, the time to clearance of the blood cultures, and hospital costs. ELT use with systemic antimicrobial therapy was associated with 100% clearance of infection and catheter salvage, based on study definitions. Larger studies are needed to confirm our study results.
Author Contributions
All three authors developed and wrote the protocol and participated in carrying out the study. WD completed the statistical analysis. All three authors wrote, critically revised and reviewed the final manuscript.
Footnotes
Appendix
Acknowledgements
We thank the patients and parents who participated in this trial. The authors also thank Monica Malian, PharmD and May Faroun, PharmD from CHM Investigational Drug Services (Pharmacy); Gerald Kurdziel for Detroit Medical Center financial data/reports; the data safety and monitoring board (Kevin Valentine, MD (Chair); Meret Henry, MD; Roshni Kulkarni, MD; Bram Dolcourt, MD); Ron Thomas; Ranu Arora and Brittany Allen, research coordinators; Nora Maloy, PhD, at BCBSM Foundation; Jackie Parker and Julie McQueeny as well as Jamal Ameli from CHM general clinical research center; Angela Moore; the 6 West nursing staff, clinical services involved with the trial, nursing educator and 6 West nursing manager.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by an investigator-initiated research grant from the Blue Cross Blue Shield of Michigan Foundation.