
Abstract
Introduction:
Ovarian lesions are diverse with a broad clinical presentation from being asymptomatic to rarely symptomatic, presenting with pain, abdominal discomfort and abdominal mass. Histopathologic analysis of ovarian lesions guides clinicians in the accurate and early management of cases.
Aim:
To analyse ovarian lesions and categorise them into non-neoplastic and neoplastic based on histopathological examination.
Material and Methods:
This is a 2-year prospective study conducted from June 2023 to June 2025 at a district tertiary care institute, with a total of 96 cases.
Results:
A total of 96 cases were studied, of which 52 were non-neoplastic and 44 were neoplastic. Follicular cyst was the most common non-neoplastic lesion and benign mucinous cystadenoma was the most common neoplastic lesion in the present study.
Conclusion:
Most of the ovarian lesions are asymptomatic and diagnosed as part of the histomorphological evaluation of hysterectomy with bilateral salpingo-oophorectomy or cystectomy specimens. Clinicoradiologic and histomorphologic findings categorise ovarian lesions into non-neoplastic and neoplastic and guides in appropriate management.
Introduction
Ovarian lesions are diverse and present from the neonatal to the postmenopausal age group. They may be asymptomatic, diagnosed as incidental lesions on ultrasonography of the pelvis, histologic diagnosis of hysterectomy with bilateral salpingo-oophorectomy specimens or may present with recurrent abdominal discomfort, abdominal pain and mass. The three histologic compartments of the ovary are surface Mullerian epithelium, germ cells and sex-cord stromal cells from which originate non-neoplastic and neoplastic lesions. In India, the incidence of ovarian cancer is on the rise and may increase in the coming years. Ovarian cancer is often diagnosed late, being asymptomatic and present at an advanced stage.
Non-neoplastic and functional cysts are the most common lesions of the ovary. The most common cystic follicles, with a size up to 2 cm, originate from unruptured Graafian follicles or from ruptured follicles that have sealed. Follicle cysts exceed 2cm in size. Luteal cysts present in the ovaries of reproductive-age women contain luteinised granulosa cells and may rupture. Polycystic ovarian syndrome is a complex endocrine disorder with many cystic follicles or follicle cysts which enlarge the ovaries. Women with PCOS are at increased risk for endometrial hyperplasia and carcinoma, as free serum estrone levels are high.
The World Health Organisation Histological classification separates ovarian neoplasms according to the most probable tissue of origin.[1] Most ovarian tumours arise from one of the three ovarian histologic components-surface Mullerian epithelium, germ cells and sex -cord stromal cells. Surface epithelial-stromal tumours are serous, mucinous, endometrioid, clear cell, transitional cell and epithelial-stromal tumours. These tumours are further categorised as benign, borderline and malignant tumours. Sex-cord-stromal tumours include granulosa tumours, fibromas, fibrothecomas, thecomas, Sertoli-Leydig cell and steroid cell tumours. Germ cell tumours include teratoma- immature, mature, solid, cystic, monodermal, dysgerminoma, yolk sac tumour and mixed germ cell tumours. Metastatic tumours from the colon, appendix, gastric, pancreaticobiliary and breast to the ovary can occur.
Patients with ovarian cysts are asymptomatic or discovered incidentally during an ultrasound or routine pelvic examination. Some cysts are symptomatic with mild to severe symptoms, and malignant ovarian cysts typically are symptomatic until they reach an advanced stage. The stage at diagnosis is strongly associated with prognosis, and histologic grade plays a role in prognosis and predicting recurrence.[2] An accurate histological diagnosis guides to initiation of a proper management plan.[3] Histological examination remains the gold standard for diagnosing ovarian cancers.[4]
The non-neoplastic lesions, functional cysts and benign lesions may be asymptomatic or may present with vague abdominal pain and be found unexpectedly on pelvic examination, ultrasonography or during surgery or histopathologic examination of hysterectomy with salpingo-oophorectomy done for other causes like leiomyoma and endometrial pathology. Neoplastic tumours may present with abdominal pain, vaginal bleeding due to large size, compression or cancer invasion. The present study evaluates histomorphological features of ovarian lesions at our institute, classifying them into non-neoplastic and neoplastic along with age range, laterality and comparison with other studies.
Material and Methods
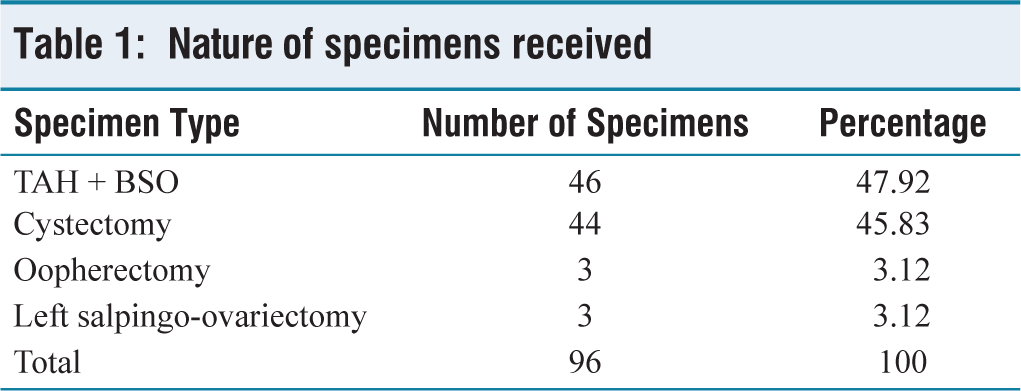
The present study is an observational, cross-sectional study conducted in the department of Pathology at Government Medical College, Nalgonda district, over a period of 2 years from June 2023 to June 2025. Inclusion criteria include lesions that are histologically diagnosed on ovarian specimens in the form of resected cystectomy specimens, ovarian masses, tubo-ovarian masses and hysterectomy with salpingo-oophorectomy [Table 1]. Exclusion criteria were normal ovaries on histology. A structured proforma is used to record clinical details, laboratory investigations of routine tests and ultrasonography. Surgically excised specimens are fixed in 10% buffered formalin overnight and grossly examined. Representative sections are taken, processed, and paraffin-embedded. Sections are cut, stained with Hematoxylin and Eosin and microscopically examined. One section (4–5 μm, magnification × 200–400) per patient is considered, and slides are viewed by two pathologists. The findings are categorised into non-neoplastic and neoplastic lesions based on gross, microscopic examination and evaluation according to age-wise distribution, laterality and histologic classification is done. All the collected data was entered and checked for completeness and consistency. Data analysis is done using SPSS 21.0 software for statistical data, presented as frequencies, percentages and represented in tables and graphs. Institutional ethics committee approval was obtained for the present study.
Nature of specimens received
Results
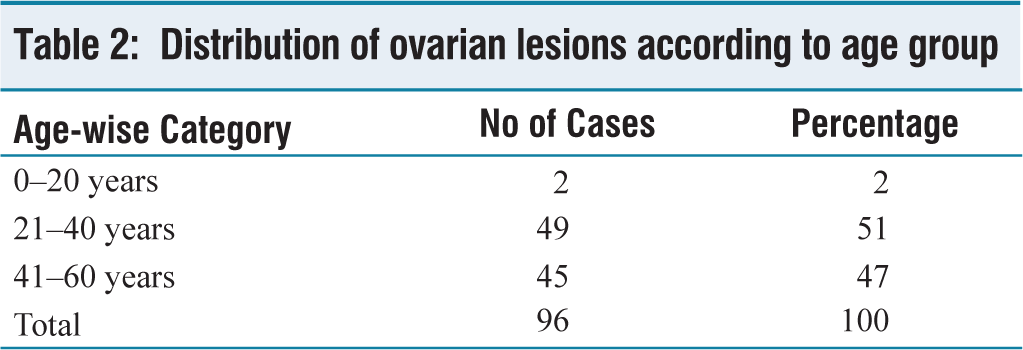
Distribution of ovarian lesions according to age group
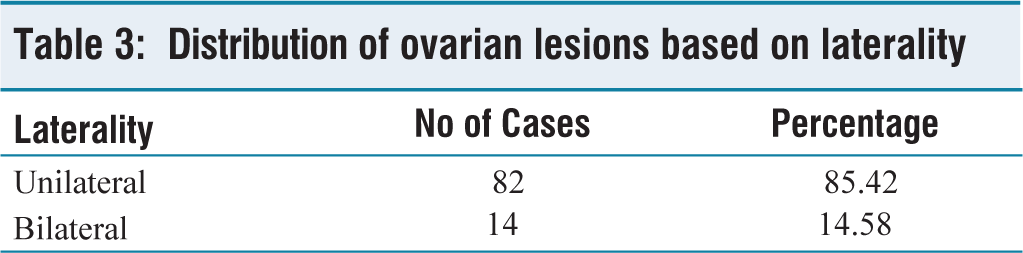
Distribution of ovarian lesions based on laterality
Discussion
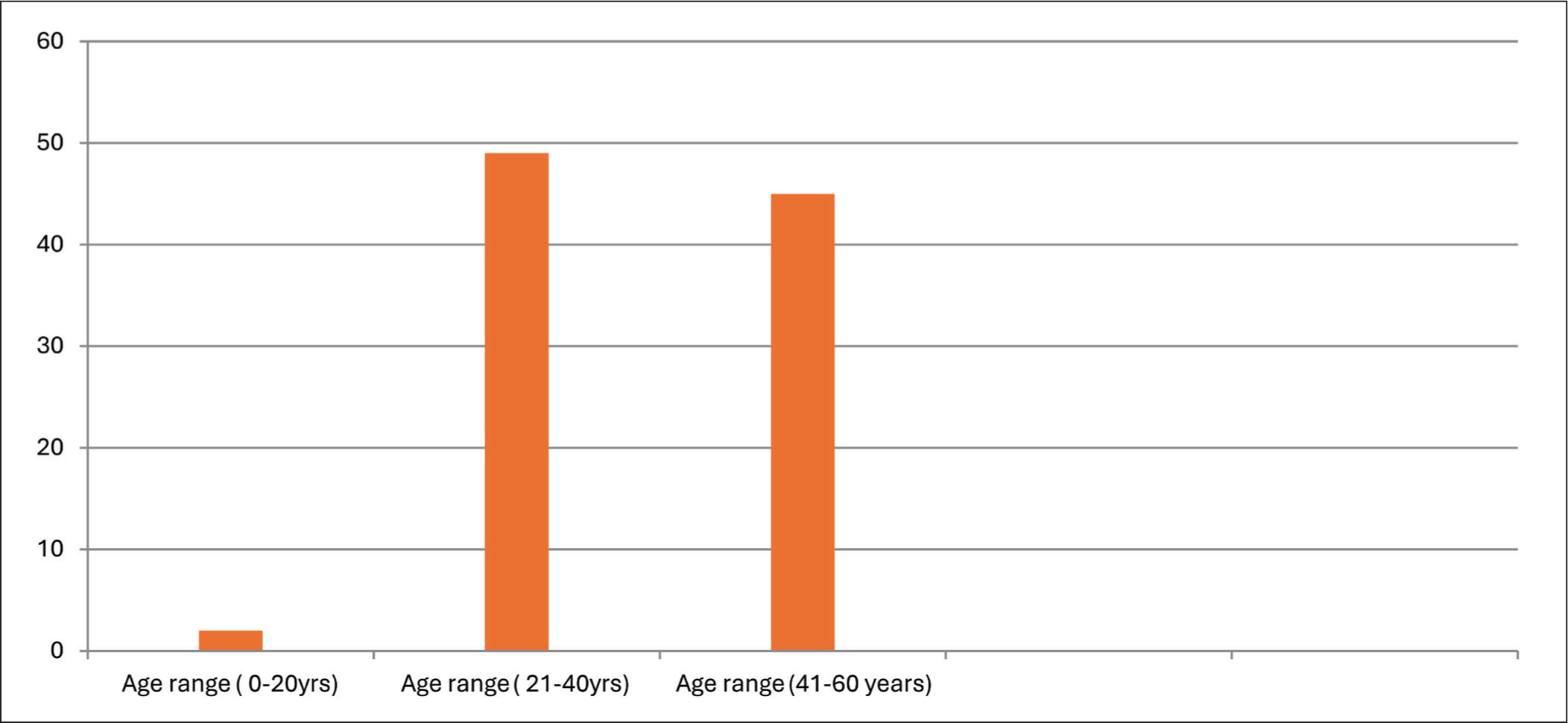
Ovarian lesions are diverse, with often similar clinical and radiologic features. Histopathologic examination confirms the non-neoplastic or neoplastic nature of ovarian lesions and thus aids in further management. The present study, conducted at a district tertiary hospital, included 96 cases of ovarian lesions. The peak incidence of ovarian lesions in the present study was in the second and third decades of life [Table 2 and Figure 1]. A study done by Yasmeen et al.[6] showed peak incidence in the third and fourth decades of life. The majority of ovarian lesions in the present study were unilateral (85.4%), similar to a study done by Yasmeen et al [Table 3].[6] with 87.8% unilateral ovarian lesions.
Distribution of cases based on age
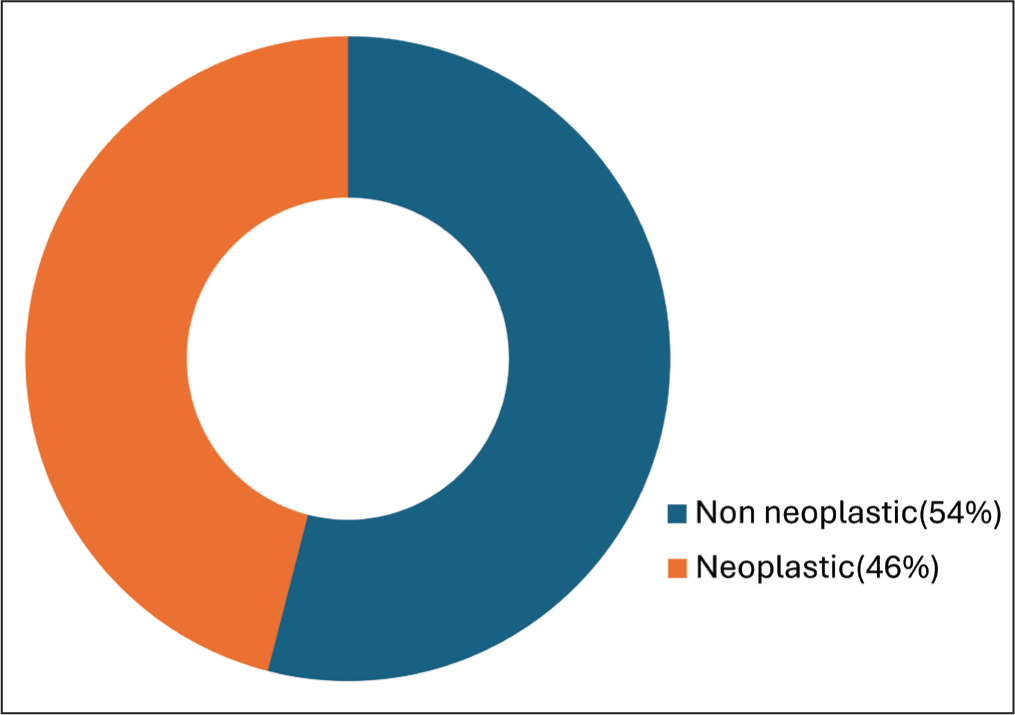
Histopathological examination of ovarian specimens showed predominantly non-neoplastic lesions (54%). Neoplastic lesions constituted 46% of the total cases [Table 4 and Figure 2]. Studies done by Gaikwad et al.[5] and Yasmeen et al.[6] also showed similar findings. In the study done by Gaikwad et al.[5] showed non-neoplastic (54.6%) and neoplastic (45.9%) ovarian lesions. A study done by Yasmeen et al.[6] showed 53.7% non-neoplastic and 46.2% neoplastic lesions [Table 5].
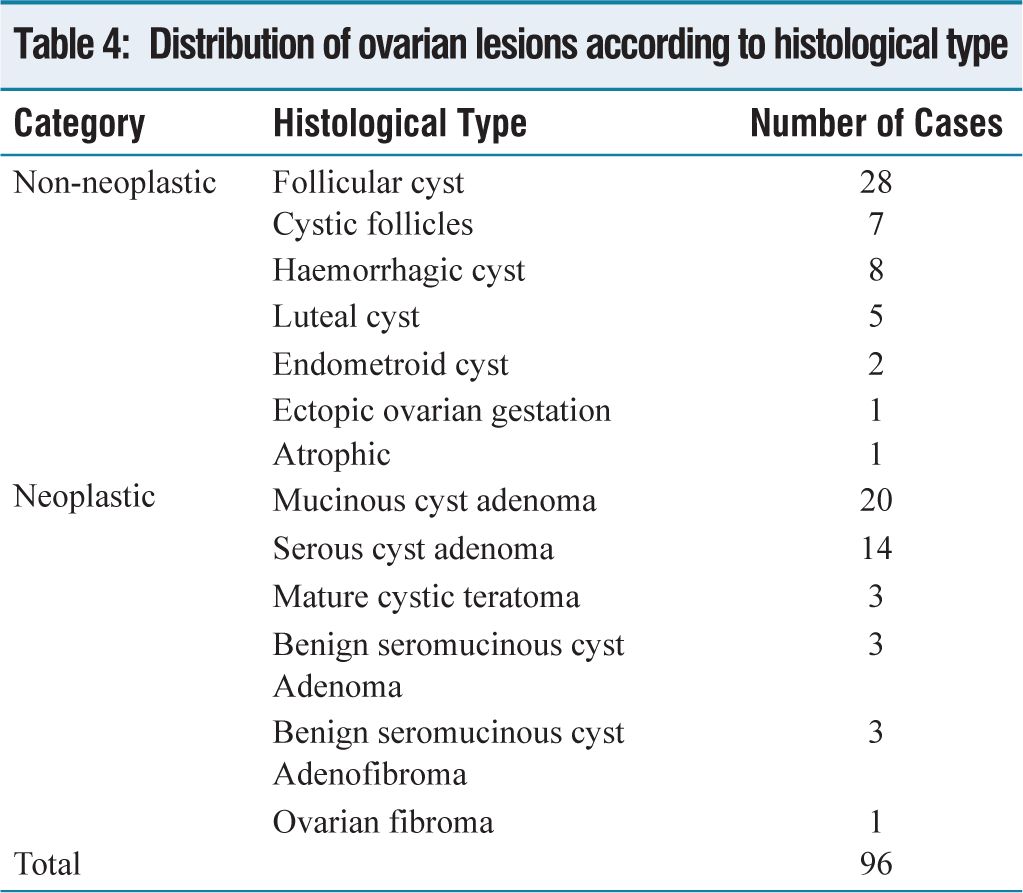
Distribution of ovarian lesions according to histological type
Comparison with other studies

Histologic classification of non-neoplastic and neoplastic ovarian lesions
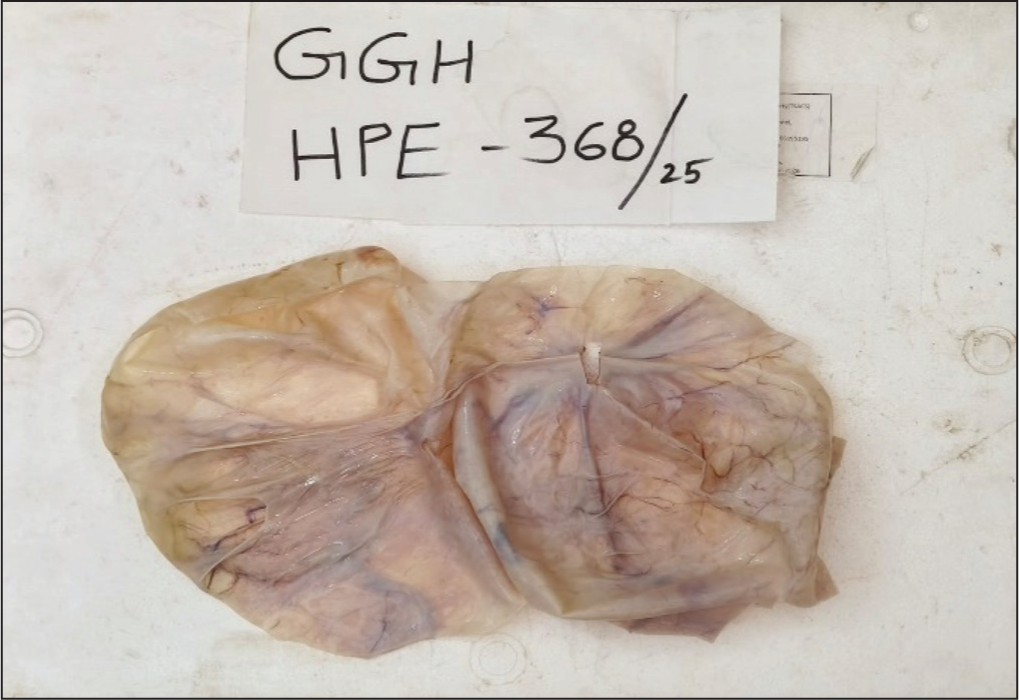
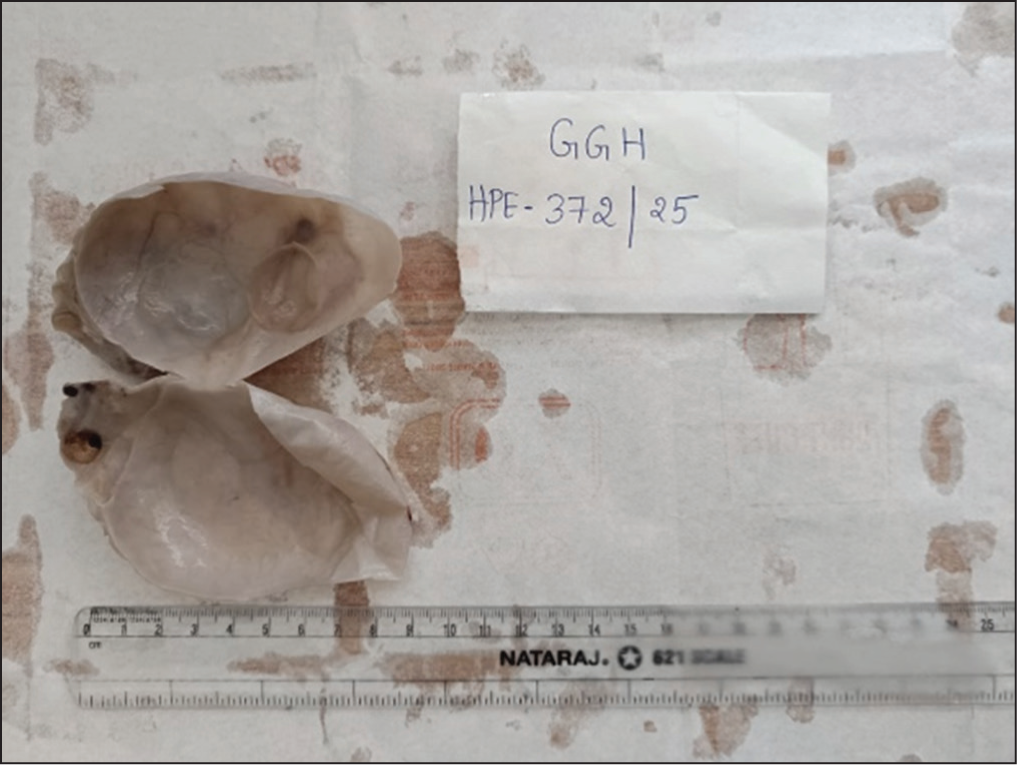
The present study showed follicular cyst as the most common non-neoplastic lesion (28/52 cases), followed by haemorrhagic cyst (8/52 cases) and benign mucinous cystadenoma (20/44 cases) as the most common neoplastic lesion, followed by benign serous cystadenoma (14/44 cases) [Figures 3-6]. A study done by Yasmeen et al.[6] also showed follicular cyst (48/71 cases) as the most common non-neoplastic lesion and mucinous cystadenoma (20/61 cases) as the most common neoplastic lesion. The present study showed only benign cases in the neoplastic category and no borderline or malignant cases, which indicates early diagnosis of cases.
Gross specimen of mucinous cystadenoma-multiloculated cyst
Microscopy of benign mucinous cystadenoma-bland mucinous epithelial lining of cyst
Gross specimen of serous cystadenoma-uniloculated cyst
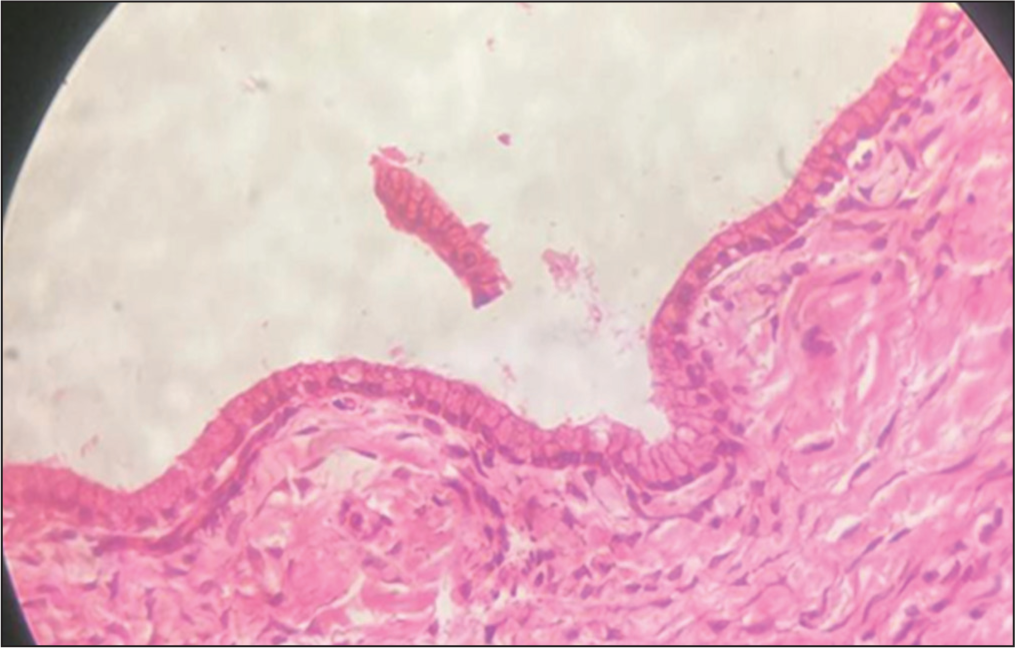
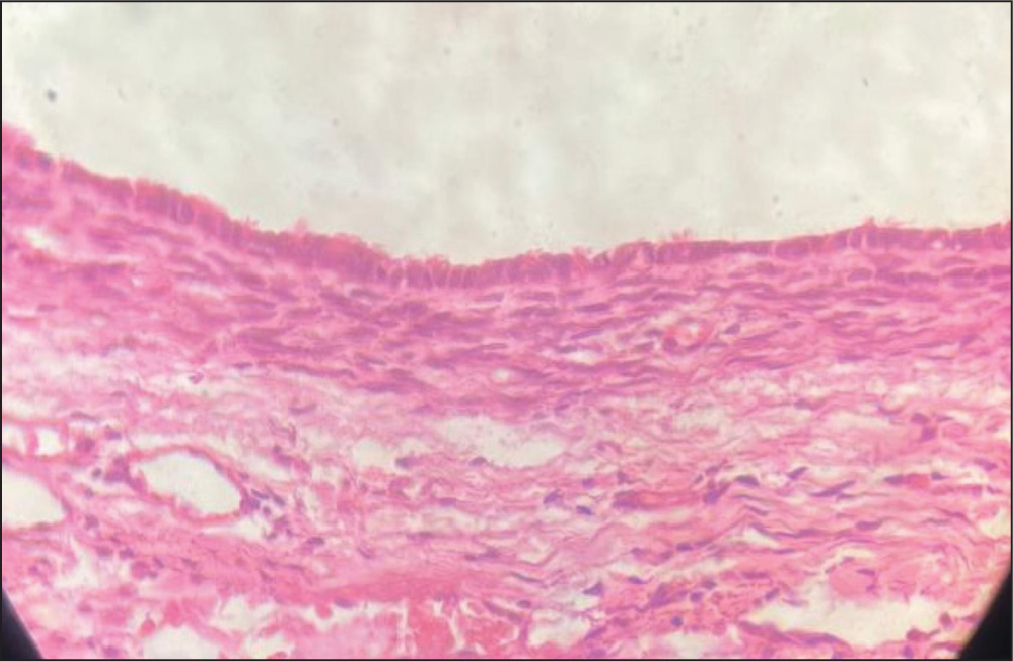
Microscopy of benign serous cystadenoma-bland tall ciliated columnar cell lining of cyst
The confirmation of non-neoplastic or neoplastic ovarian lesions is done by histopathological examination, as these lesions often present with similar clinical and radiological features. HPE diagnosis further aids in the proper management of ovarian lesions.
Conclusion
The present study, conducted at a district tertiary care hospital, Nalgonda, over a period of two years, included 96 cases, of which non-neoplastic ovarian lesions were more common (54%) than neoplastic (46%). The predominant age group affected was 21–40 years, with follicle cysts as the most common ovarian lesion. Benign mucinous cystadenoma is the most common neoplastic lesion seen. Clinicoradiologic and histomorphologic findings categorise ovarian lesions into non-neoplastic and neoplastic and guide the appropriate management of cases.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
The present study was done after ethics approval was obtained from the institutional ethics committee - GMC/NLG/2025/24.
Informed consent
Not applicable.