
Abstract
Introduction:
Polycystic ovarian syndrome (PCOS) is a highly prevalent endocrine abnormality affecting women in the age group of 15–45 years. Women with PCOS typically exhibit an androgenic pattern of body fat distribution, characterised by central adiposity, and are frequently accompanied by insulin resistance (IR) and elevated androgen levels. The homeostasis model assessment (HOMA-IR) has been used as a detection method of IR. Neck circumference (NC) is an easy method and can be accurately correlated with HOMA-IR.
Methods:
After obtaining ethical approval, data were collected from 143 diagnosed cases of PCOS patients. Anthropometric measurements—including height (cm), weight (kg), body mass index (BMI), waist circumference (WC), hip circumference (HC), and NC—were recorded using standardised tools. All data were entered into Microsoft Excel 2013 and analysed using SPSS version 21.
Results:
In the present study, 80 (55%) PCOS patients were diagnosed with IR based on the HOMA-IR cut-off of > 2.5. The levels of fasting blood glucose, fasting insulin, and anthropometric indexes (NC, WC, BMI, and waist-to-hip ratio [WHR]) in the IR group were much higher than those in the control group. There was a strong correlation of NC with anthropometric ratios like WC, WHR and BMI, whereas the correlation was moderate with HOMA-IR. Receiver operating characteristic analysis demonstrated that NC ≥ 30.75 cm had a high probability of being a marker of IR in women with PCOS.
Conclusion:
NC correlates significantly with BMI, WC, and WHR.
Keywords
Introduction
Polycystic ovarian syndrome (PCOS) is a common endocrine disorder affecting women between the ages of 15 and 45. When diagnosed using Rotterdam’s 2003 criteria, its prevalence ranges from 4% to 21%.[1] PCOS is frequently linked to metabolic syndrome (MS), characterised by insulin resistance (IR), hyperandrogenism (HA), impaired glucose tolerance, obesity, overweight, and hypertension.[2]
Women with PCOS frequently present with obesity and a central, androgenic distribution of body fat. These patients often present with added features of IR and hyperandrogenemia.[3] Intra-abdominal fat and obesity have a detrimental impact on tissue IR because of the increased plasma levels of non-esterified fatty acids originating from the lipolysis of abdominal fat.[4] IR is the key factor associated with MS in PCOS, and can later in life lead to various cardiovascular complications and diabetes mellitus. So, early diagnosis of IR is needed for the prevention of MS in PCOS development.
The homeostasis model assessment (HOMA-IR) has been used as a detection method of IR. HOMA-IR was originally developed by Matthews and later modified by Levy et al.[5,6] HOMA-IR is calculated using the formula: Fasting insulin [(µIU/mL) × fasting glucose (mmol/l)]/22.5. Patients are considered to have IR when the HOMA-IR index is ≥2.6 × 10–6mol × U/l2.[7] Some studies have compared HOMA-IR with anthropometric parameters like body mass index (BMI), waist circumference (WC), hip circumference (HC), WC/HC and neck circumference (NC). Out of all these, NC is an easy method and can be accurately correlated with HOMA-IR. It is a marker of upper-body subcutaneous adipose tissue distribution. But there are limited studies in India which can establish the role of NC, especially in the eastern part of India, for the determination of IR in patients of PCOS.
So, the primary objective of this study is to determine the prevalence of IR in the study population using the HOMA-IR method. We also aim to find the relation between NC and IR.
Methodology
A hospital-based cross-sectional study was conducted in the gynaecology outpatient department of a tertiary care centre. The study included women aged 15–45 who were diagnosed with PCOS using the Rotterdam criteria. According to this definition, a diagnosis requires at least two of the following three criteria:
Menstrual irregularities, such as oligomenorrhea or amenorrhea (fewer than eight cycles per year or cycle intervals exceeding 35 days).
Biochemical or clinical HA, indicated by elevated levels of total or free testosterone, androstenedione, or dehydroepiandrosterone sulphate, or physical signs such as hirsutism, male-pattern alopecia, and acne.
Polycystic ovarian morphology (PCOM), characterised by at least one ovary containing 12 or more peripheral follicles (2–9 mm in diameter) or an ovarian volume of at least 10 mL, as observed via transvaginal or abdominal ultrasound.
Transvaginal ultrasonography was employed as the primary diagnostic tool for sexually active women, provided they were comfortable with the procedure. Women with diabetes mellitus, other causes of hyperandrogenaemia—including congenital adrenal hyperplasia, androgen-secreting tumours, or Cushing’s syndrome—or those outside the age range of 15–45 years were excluded from participation.
Drawing on findings from Kalra et al., which reported a 76.9% prevalence of IR among women with PCOS, the required sample size was calculated as 118, assuming an alpha of 0.05 and 80% statistical power.[8] To accommodate an anticipated 20% refusal rate, the final sample size was set at 143. Ethical clearance was obtained from the Institute Ethics Committee, and all participants provided written informed consent after receiving a detailed explanation of study procedures.
Data collection utilised a pre-tested semi-structured questionnaire to capture socio-demographic details, obstetric history, and clinical features of HA such as acne and hirsutism. Anthropometric measurements—including height, weight, BMI, WC, HC, and NC—were recorded using standardised instruments. NC was measured at the midpoint between the mid-cervical spine and the anterior neck with a non-stretchable plastic tape, accurate to the nearest millimetre, while participants stood upright.
Biochemical evaluation included fasting blood glucose (FBG), a 2-hour oral glucose tolerance test with 75 g of glucose, and fasting insulin levels, measured using an automated biochemical analyser with chemiluminescence technology. Ultrasound examinations were performed in real time with a high-resolution 6-MHz probe on a three-dimensional ultrasound system. For sexually active women, transvaginal ultrasonography was preferred. Ovarian follicle count (2–9 mm diameter) was assessed using the three-dimensional Sono AVC technique, and ovarian volume was calculated with specialised software.
Data entry was carried out in Microsoft Excel 2013, and statistical analysis was performed using SPSS version 21. Categorical variables were expressed as percentages, while continuous variables with normal distribution were presented as means with standard deviation or 95% confidence intervals (CI). Associations between socio-demographic and clinical variables were examined using chi-squared tests, and multivariate logistic regression was applied to identify predictors of IR. A receiver operating characteristic (ROC) curve was plotted to determine the optimal cut-off value of NC for detecting IR.
All participant information was kept strictly confidential, accessible only to study investigators. Reports generated from the study excluded personal identifiers.
Results
A total of 143 patients diagnosed with PCOS were included in the study. Out of these, 80 patients were found to be insulin resistant (IR), and 63 women were found to have no IR. Table 1 shows the percentage of PCOD patients with different phenotypes having IR and non-IR. Among the 143 patients of PCOD, 30 belonged to phenotype A with IR, but 15 (10.5%) of phenotype A PCOD patients were not insulin resistant. Of the total 20 phenotype B PCOD patients, 13 (9.1%) were insulin resistant. When the phenotype C PCOD patients were considered, 12 patients were insulin resistant, while eight patients were non-insulin resistant. Among the 78 phenotype D patients, 33 (23.1%) had no IR.
Phenotypic variation and insulin resistance
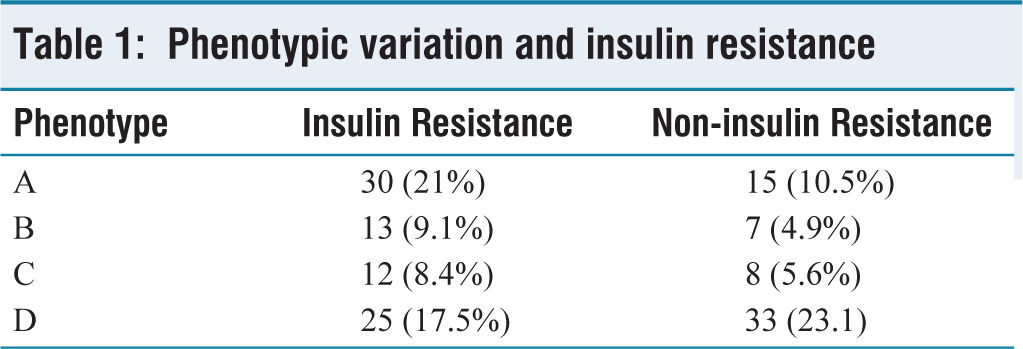
Table 2 depicts the anthropometric variation in the study population. The mean ages of the study population were 27.9 ± 5.93 (26.6–29.2) for those found to have IR, and 25.4 ± 6.05 (23.9–27) for those without IR (P = .01).
Anthropometric variables and biochemical characteristics characterised by the presence of IR in women with PCOS
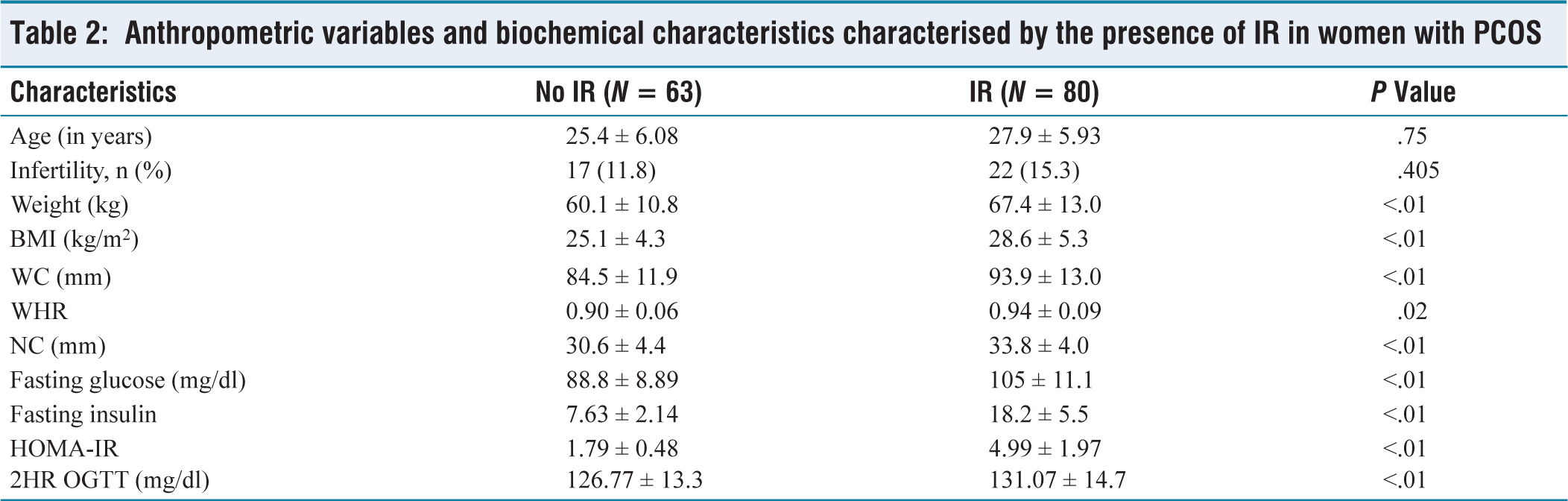
Among the 143 participants enrolled for the study, 80 (55%) were diagnosed with IR based on the HOMA-IR cut-off of >2.5. The participants were divided into two groups based on IR, that is, IR and those without IR (no IR). Two groups were comparable with respect to age (25.4 vs. 27.9 years, P = .75) and prevalence of infertility (11.8% vs. 15.3%, P = .4). As compared to participants without IR, the participants with IR had higher mean weight (MD = 7.3, P < .001), BMI (MD = 3.5, P < .001), WC (MD = 9.4, P < .001), waist hip ratio (MD = 0.4, P = .02), NC (MD = 3.2, P < .001), fasting glucose (MD = 16.2, P < .001), fasting insulin (MD = 10.57, P < .001) and 2 hour oral glucose tolerance test (MD = 4.3, P < .001).
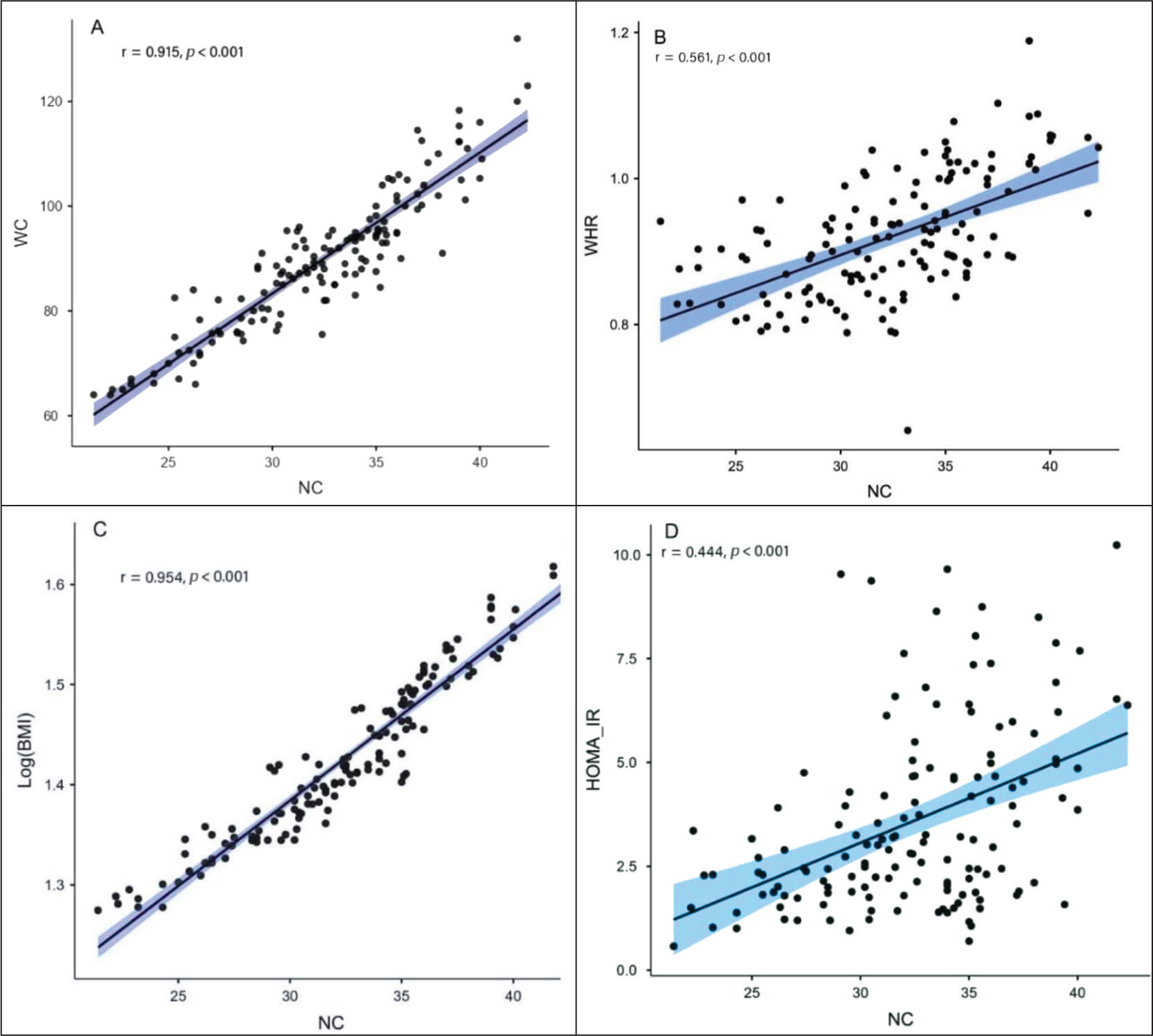
Figure 1A-1D depicts the correlation between NC with WC, waist-to-hip ratio (WHR), BMI (Log transformed) and HOMA-IR (Log transformed). Pearson correlation analysis was performed. NC in participants with PCOS was shown to be positively correlated with WC (r = 0.915; P < .001), WHR (r = 0.561.761; P < .001), BMI (r = 0.954; P < .001) and HOMA-IR (r = 0.444; P < .001) and HOMA-IR (r = 0.458; P < .001). Strong correlation of NC was observed with anthropometric ratios like WC, WHR and BMI, whereas the correlation was moderate with HOMA-IR.
Correlation between NC with WC, WHR, BMI (Log transformed) and HOMA-IR (Log transformed)
Additionally, multiple linear regression analysis was performed to explore the associations between NC with HOMA-IR (log transformed), with adjustment for different potential confounding factors. In the base model without any adjustment, NC was associated significantly with HOMA-IR (the unstandardised coefficient [B] 0.03; 95% CI = 0.02–0.04; P < .001). After the adjustment for potential confounders like age, the association was still found statistically significant (B = 0.03; 95% CI = 0.02–0.04; P < .001).
To further explore the association between NC and IR binary logistic regression analysis was performed. In the model without adjustment for any confounding factors, the OR was 1.192 (95% CI = 1.093–1.299; P < .001). After adjustment for age, the OR was 1.177 (95% CI = 1.073–1.290; P = .001).
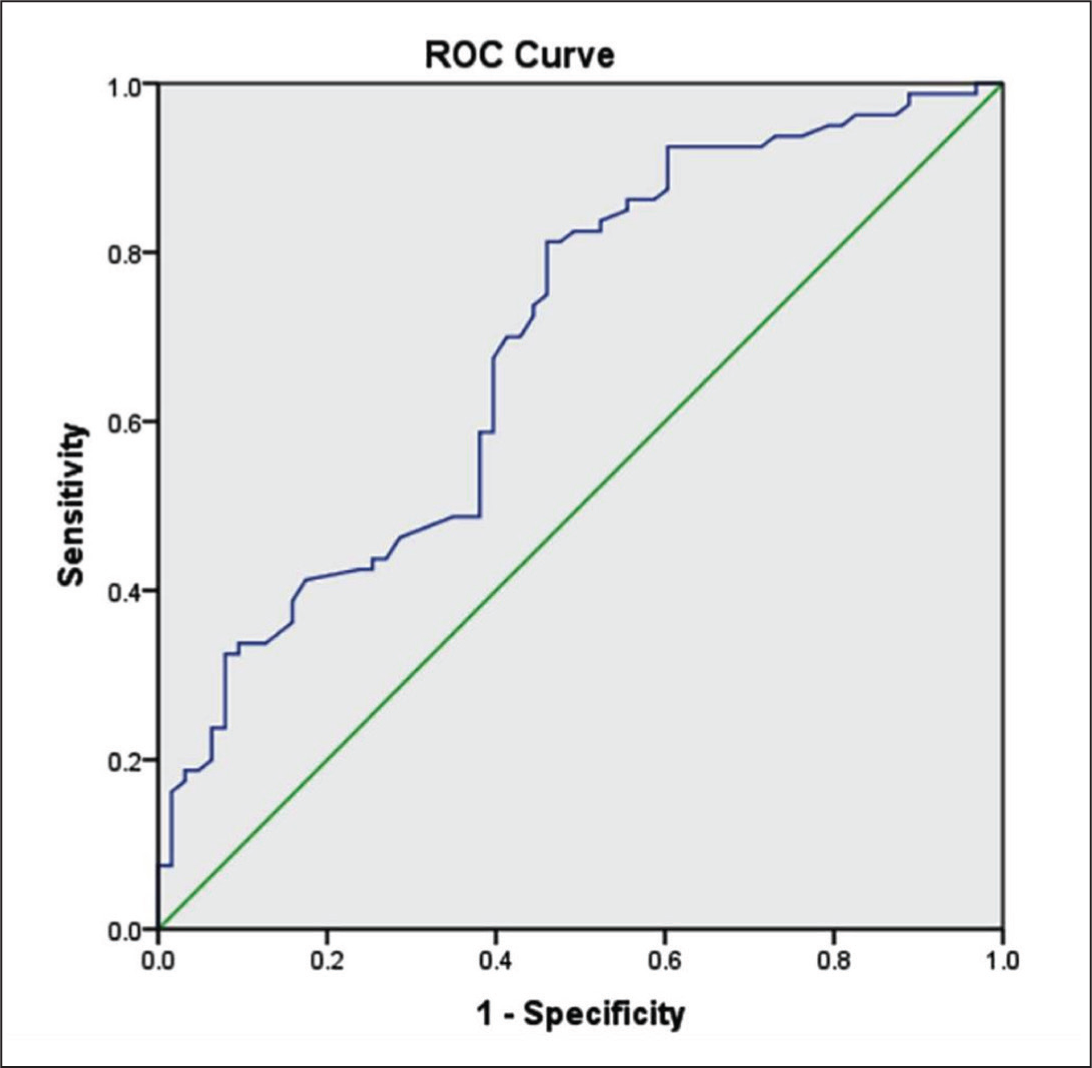
To find out the suggested cut-off values of NC for determining IR, the ROC analysis was used [Figure 2]. NC performed relatively well in classifying women with PCOS to IR. The area under the ROC curve (AUC) for NC was 0.693 (95% CI = 0.606–0.781; P < .01), which is similar to other independent variable for determining the IR like WC (AUC = 0.689, 95% CI = 0.602–0.776, P < .001), WHR (AUC = 0.604, 95% CI = 0.511–0.696, P < .05), and BMI (AUC = 0.693 95% CI = 0.605–0.781, P < .001). The best cut-off point of NC for determining IR is observed to be 30.75 cm (Youden index = 0.352).
Receiver operating characteristic (ROC) analysis.
Discussion and Review of Literature
PCOS is a complex endocrine disorder characterised by menstrual irregularities, excessive androgen levels, and PCOM.[9] Over the past three decades, significant efforts have been made to refine its diagnostic criteria. In 1990, the National Institutes of Health (NIH) established that both clinical and biochemical HA and chronic anovulation were necessary for a PCOS diagnosis.[10] Later, a consensus workshop sponsored by the European Society of Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM) proposed that a diagnosis should be based on the presence of at least two of the following three criteria:
Oligo/anovulation (OA), clinical or biochemical HA, PCOM observed via ultrasonography.[11]
In 2006, the Androgen Excess and PCOS (AE-PCOS) Society further refined these criteria, emphasising that HA, along with ovulatory dysfunction—either in the form of oligo-anovulation or PCOM—was essential for diagnosing PCOS.[12] Excess androgen production in the ovaries, driven by increased luteinising hormone (LH) secretion and bioactivity, is considered a central feature of PCOS. IR plays a key role in this process by contributing to hyperinsulinemia, which further promotes hyperandrogenaemia through two mechanisms: Enhancing ovarian androgen production in synergy with LH and reducing sex hormone-binding globulin (SHBG) levels, thereby increasing free androgen levels.
This cycle of IR and elevated androgen levels creates a self-sustaining positive feedback loop that can worsen over time.[13]
PCOS is frequently associated with MS, which includes IR, HA, impaired glucose tolerance, type 2 diabetes mellitus, obesity, and hypertension.[2] Studies indicate that the prevalence of MS among women with PCOS ranges from 34% to 46%.[14] IR in PCOS is considered the key component for the pathogenesis of the disease and is also common to MS.[15] Therefore, the early identification of IR in females with PCOS is essential to halt the cascade of events and prevent long-term morbidity. The prevalence of IR in PCOS patients is observed to be approximately 12% to 60%.[16]
In this study, 55% of PCOS patients (80 individuals) were diagnosed with IR based on a HOMA-IR cut-off value of >2.5. The insulin-resistant group exhibited significantly higher levels of FBG, fasting insulin, and anthropometric indices—including NC, WC, BMI, and WHR—compared to the control group. NC showed a strong correlation with WC, WHR, and BMI, while its correlation with HOMA-IR was moderate.
Multiple methods are available for detecting IR, including the hyperinsulinaemic euglycaemic clamp technique, the quantitative insulin sensitivity check index (QUICKI), and the HOMA-IR.[15] However, these techniques are costly, time-consuming, and require specialised equipment and trained personnel, making large-scale clinical application impractical.[17] In contrast, anthropometric indicators such as NC, WC, WHR, and BMI are simpler, effective predictors of MS and cardiovascular risk.[18,19] However, not all anthropometric measurements are feasible for routine clinical practice. Thus, identifying a quick, reliable, and accessible method for early detection of IR is crucial.
NC is increasingly recognised as a reliable indicator of upper-body subcutaneous fat and a potential predictor of cardiometabolic risk. It is a simple and time-efficient measurement that does not require patients to undress, and it remains unaffected by body movements, respiration, or variations in satiety.[19] In this study, ROC analysis showed that an NC measurement of ≥30.75 cm was highly predictive of IR in women with PCOS.
Recent studies have demonstrated a strong association between NC and markers of MS.[20] However, evidence specifically examining NC as a predictor of IR in women with PCOS remains limited. Research has indicated that increased NC is linked to a higher prevalence of both MS and PCOS in obese premenopausal women.[21] Furthermore, a meta-analysis of cross-sectional studies confirmed that NC shows a positive correlation with glycaemic parameters, including FBG, serum fasting insulin, HOMA-IR, and HbA1c.[22]
Limitations of the Study
As this was a cross-sectional study, the temporal association between NC and IR cannot be determined. This study was conducted at a single centre, which may limit the generalizability of the findings to the general population. The AUC for NC (0.693) indicates only moderate discriminative ability. While statistically significant, it may not be clinically robust enough for standalone screening and hence larger studies are required in this field.
Conclusion
This study has demonstrated that NC is a practical anthropometric measurement for predicting PCOS. The findings suggest that NC correlates significantly with other established markers of PCOS, such as BMI, WC, and WHR. Our findings suggest that NC is a practical and reliable screening measure. Incorporating NC assessment into routine clinical examinations may enhance the early detection of PCOS, thereby supporting timely intervention and effective management.
Future investigations should aim to refine population-specific NC cut-off values and explore the biological mechanisms underlying the association between increased NC and PCOS pathology. Moreover, longitudinal studies are warranted to evaluate the predictive utility of NC over time and its role in monitoring disease progression and treatment response.
In conclusion, integrating NC measurement into the diagnostic framework for PCOS offers significant potential to strengthen early diagnosis and improve health outcomes for women living with this condition.
Supplemental material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Farhad Ahmad for his contribution in designing the project.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Ethics committee approval code: T/IM-NF/Kalyani/21/03. Name of the institution where the work was done (if it is a research study): AIIMS Kalyani, India.
Credit author statement
Dr Ipsita Mohapatra: Conception of the work; Data acquisition, analysis, drafting, critically reviewing, final approval, accountable for all aspects of work.
Dr Subha Ranjan Samantaray: Data acquisition, analysis, drafting, critically reviewing, final approval, accountable for all aspects of work.
Data availability
All supporting data are available in the article.
Use of artificial intelligence
No generative artificial intelligence was used in the writing of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.